
Rationale and Objectives
To determine the current policies and practices of Society for Pediatric Radiology (SPR) members regarding the evaluation of pediatric patients with suspected pulmonary embolism (PE) with an emphasis on use of computed tomography pulmonary angiography (CTPA).
Materials and Methods
Institutional review board exemption was granted for this study. Surveys were mailed electronically to the 1575 members of the SPR representing 416 institutions. Information gathered included the existence of written policies, the imaging study of choice for suspected PE, routine acquisition of chest radiographs before CTPA, currently used CTPA techniques, modifications of protocols for radiation dose reduction, typical DLP (dose-length-product) for CTPA, and estimated annual frequency of performing CTPA for evaluating PE in children. Survey items pertaining to policies and practices were compared between practice settings and populations using chi-square analysis.
Results
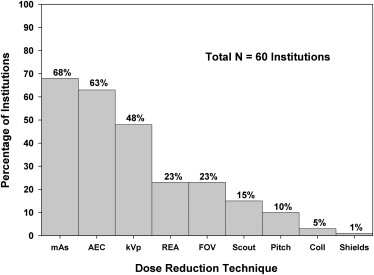
One hundred and sixty members representing 118 institutions responded, which resulted in a response rate of 28% (118/416), on an institutional basis. Of these 118 respondents, 104 (88%) perform CTPA in children with clinical suspicion of PE. Of the 104 respondents who perform CTPA, 26 (25%) have a written policy for CTPA, 93 (89%) perform CTPA as the first study choice, and 67 (64%) routinely obtain chest radiographs before CTPA. The most commonly used CTPA techniques in children with clinical suspicion of PE include intravenous contrast amount of 2 mL/kg, mechanical injection of intravenous contrast, and tailored bolus tracking method for CTPA scan initiation by observing the Hounsfield units of contrast in the central pulmonary artery on the monitoring scan. Sixty respondents (58%) modify CTPA imaging protocols for evaluating PE in children in order to decrease radiation dose. The two most common modifications for radiation dose reduction were reduced mAs in 41 (68%) and automatic exposure control in 38 (63%). The majority of respondents (88%) did not know the typical DLP for a 20-kg child during CTPA study performed to evaluate for PE. A significantly greater percentage of radiation dose-reduction techniques are performed within academic institutions compared with private institutions ( P = .03).
Conclusion
Most survey respondents perform CTPA as the study of choice for evaluating PE in children, but there is considerable variability in their policies and practices. Respondents from academic medical centers are more likely to employ radiation dose-reduction techniques for CTPA than those in private practice settings.
Although ventilation-perfusion scanning and conventional pulmonary angiography have traditionally served as the mainstay of imaging for suspected pulmonary embolism (PE) in children , recent studies suggest an increasing role of computed tomography pulmonary angiography (CTPA) for this indication . For example, a high prevalence of PE (14%–15%) has been reported when using CTPA to image children with clinically suspected PE at large pediatric tertiary care hospitals . Among children with clinically suspected but excluded PE, pneumonia and atelectasis have been found to be the most common alternative diagnoses on CTPA . Furthermore, optimizing contrast enhancement techniques with CTPA in children with congenital heart disease after a lateral tunnel Fontan have been also investigated .
However, to our knowledge, there is no published information regarding how CTPA is performed in children across different institutions in both academic and private practice settings. Therefore, the purpose of this study was to determine the current policies and practices of Society of Pediatric Radiology (SPR) members regarding the evaluation of children with clinical suspicion of PE with an emphasis on CTPA.
Materials and methods
Institutional Review Board Approval
Get Radiology Tree app to read full this article<
Survey Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Survey Responses
Get Radiology Tree app to read full this article<
Policies and Practice Patterns
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CTPA Technique Details
Amount of intravenous contrast
Get Radiology Tree app to read full this article<
Table 1
Summary of Currently Used CTPA Protocols by Responding Institutions
Technical Parameters Response Categories Amount of IV contrast 2 mL/kg (68; 65%) 1.5 mL/kg (12; 12%) Don’t know (9; 9%) 1.0 mL/kg (7; 7%) 3.0 mL/kg (5; 5%) 2.5 mL/kg (3; 3%) Methods of IV contrast administration Mechanical injection (58; 56%) Dependent on the size of the IV catheter
(43; 41%) Hand injection
(3; 3%) Timing of CTPA scan initiation Tailored bolus tracking method
(80; 77%) Fixed time method
(22; 21%) Don’t know
(2; 2%)
CTPA, computed tomography pulmonary angiography; IV, intravenous.
Get Radiology Tree app to read full this article<
Methods of IV contrast administration
Get Radiology Tree app to read full this article<
Timing of CTPA scan initiation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Modifications of CTPA protocols for dose reduction in children
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
DLP for CTPA information
Get Radiology Tree app to read full this article<
Demographics of Respondents
Get Radiology Tree app to read full this article<
Comparison between Practice Settings and Practice Population Regarding Policy and Practices of CTPA in Children
Get Radiology Tree app to read full this article<
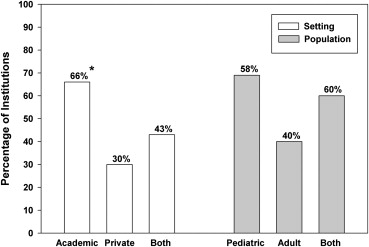
Table 2
CTPA Policies and Practices for Evaluating PE in Children by Primary Practice Setting
Survey Item Total
( n = 104) Academic
( n = 73) Private
( n = 10) Both
( n = 21)P Value Written policy for evaluating PE 26 (25%) 19 (26%) 1 (10%) 6 (29%) .50 First study choice CTPA 93 (89%) 64 (88%) 9 (90%) 20 (95%) V/Q scan 10 (10%) 9 (12%) 1 (10%) 0 (0%) Conventional 1 (1%) 0 (0%) 0 (0%) 1 (5%) .16 PA Radiograph before CTPA 67 (64%) 50 (69%) 7 (70%) 10 (48%) .46 Use of dose-reduction techniques 60 (58%) 48 (66%) 3 (30%) 9 (43%) .03 ∗ CTPA frequency to evaluate PE/year 1–5 51 (49%) 34 (47%) 5 (50%) 12 (57%) 6–10 23 (22%) 17 (23%) 1 (10%) 5 (24%) 11–15 12 (12%) 8 (11%) 2 (20%) 2 (10%) >15 18 (17%) 14 (19%) 2 (20%) 2 (10%) .84
CTPA, computed tomography pulmonary angiography; PE, pulmonary embolism; V/Q, ventilation and perfusion; PA, pulmonary angiography.
Get Radiology Tree app to read full this article<
Table 3
CTPA Policy and Practices for Evaluating PE in Children by Primary Practice Population
Survey Item Total
( n = 104) Pediatric
( n = 69) Adult
( n = 5) Both
( n = 30)P Value Written policy for evaluating PE 26 (25%) 20 (29%) 0 (0%) 6 (20%) .27 First study choice CTPA 93 (89%) 63 (91%) 5 (100%) 25 (84%) V/Q scan 10 (10%) 6 (9%) 0 (0%) 4 (13%) Conventional 1 (1%) 0 (0%) 0 (0%) 1 (3%) .45 PA Radiograph before CTPA 67 (64%) 44 (64%) 4 (80%) 19 (63%) .95 Use of dose-reduction techniques 60 (58%) 40 (58%) 2 (40%) 18 (60%) .70 CTPA frequency to evaluate PE/year 1–5 51 (49%) 34 (49%) 5 (100%) 12 (40%) 6–10 23 (22%) 16 (23%) 0 (0%) 7 (23%) 11–15 12 (12%) 8 (12%) 0 (0%) 4 (13%) >15 18 (17%) 11 (16%) 0 (0%) 7 (23%) .37
CTPA, computed tomography pulmonary angiography; PE, pulmonary embolism; V/Q, ventilation and perfusion; PA, pulmonary angiography.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Appendix 1
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. The PIOPED Investigators. Value of the ventilation/perfusion scan in acute pulmonary embolism. Results of the prospective investigation of pulmonary embolism diagnosis (PIOPED). JAMA 1990; 263: pp. 2753-2759.
2. Andrew M., David M., Adams M., et. al.: Venous thromboembolic complications (VTE) in children: first analyses of the Canadian Registry of VTE. Blood 1994; 83: pp. 1251-1257.
3. Revel-Vilk S., Massicotte P.: Thromboembolic diseases of childhood. Blood 2003; 17: pp. 1-6.
4. Babyn P.S., Gahunia H.K., Massicotte P.: Pulmonary thromboembolism in children. Pediatr Radiol 2005; 35: pp. 258-274.
5. Victoria T., Mong A., Altes T., et. al.: Evaluation of pulmonary embolism in a pediatric population with high clinical suspicion. Pediatr Radiol 2009; 39: pp. 35-41.
6. Kritsaneepaiboon S., Lee E.Y., Zurakowski D., et. al.: MDCT pulmonary angiography evaluation of pulmonary embolism in children. AJR Am J Roentgenol 2009; 192: pp. 1246-1252.
7. Lee E.Y., Kritsaneepaiboon S., Zurakowski D., et. al.: Beyond the pulmonary arteries: alternative diagnoses in children with MDCT pulmonary angiography negative for pulmonary embolism. AJR AM J Roentgenol 2009; 193: pp. 888-984.
8. Prabhu S.P., Mahmood S., Sena L., et. al.: MDCT evaluation of pulmonary embolism in children and young adults following a lateral tunnel Fontan procedure: optimizing contrast-enhancement techniques. Pediatr Radiol 2009; 39: pp. 938-944.
9. Altman D.G.: Practical statistics for medical research.1991.Chapman & Hall/CRCBoca Raton, FL p. 241–253
10. Chodick G., Kim K.P., Shwartz M., et. al.: Radiation risks from pediatric computed tomography scanning. Pediatr Endocrinol Rev 2009; 7: pp. 109-116.
11. Frush D.P.: Radiation, CT, and children: the simple answer is … it’s complicated. Radiology 2009; 252: pp. 4-6.
12. Cohen M.D.: Pediatric CT radiation dose: how low can you go?. AJR Am J Roentegenol 2009; 192: pp. 1292-1303.
13. Linet M.S., Kim K.P., Rajaraman P.: Children’s exposure to diagnostic medical radiation and cancer risk: epidemiologic and dosimetric considerations. Pediatr Radiol 2009; 1: pp. S4-S26.
14. Frush D.P., Yoshizumi T.: Conventional and CT angiography in children: dosimetry and dose comparisons. Pediatr Radiol 2006; 36: pp. 154-158.
15. Brody A.S., Frush D.P., Huda W., et. al.: Radiation risk to children from computed tomography. Pediatrics 2007; 120: pp. 677-682.
16. Huda W.: Radiation doses and risks in chest computed tomography examinations. Proc Am Thorac Soc 2007; 4: pp. 316-320.
17. Strauss K.J., Goske M.J., Kaste S.C., et. al.: Image gently: ten steps you can take to optimize image quality and lower CT dose for pediatric patients. AJR Am J Roentgenol 2010; 194: pp. 868-873.
18. Image Gently. CT Resources. Available at: http://www.pedrad.org/associations/5364/ig/index.cfm?page=369 . Accessed July 11, 2010.
19. Nievelstein R.A., van Dam I.M., van der Molen A.J.: Multidetector CT in children: current concepts and dose reduction strategies. Pediatr Radiol 2010; 40: pp. 1324-1344.
20. Kim J.E., Newman B.: Evaluation of a radiation dose reduction strategy for pediatric chest CT. AJR Am J Roentgenol 2010; 194: pp. 1188-1193.
21. Schuster M.E., Fishman J.E., Copeland J.F., et. al.: Pulmonary embolism in pregnancy patients: a survey of practices and policies for CT pulmonary angiography. AJR Am J Roentgenol 2003; 181: pp. 1295-1498.
22. Jeudy J., White C.S., Munden R.F., et. al.: Management of small (3–5 mm) pulmonary nodules at chest CT: global survey of thoracic radiologists. Radiology 2008; 247: pp. 847-853.