
Rationale and Objectives
Pulmonary enhancement imaging (PEI) derived from dual-energy computed tomographic (CT) imaging has been used to detect perfusion defects from pulmonary embolism (PE). The purpose of this study was to compare the ability of PEI, planar, single photon-emission CT (SPECT) perfusion scintigraphy, and SPECT-CT fusion images to detect perfusion defect in a PE rabbit model.
Materials and Methods
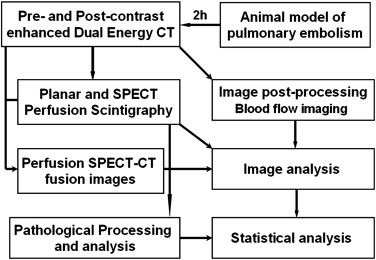
A PE model was made by injecting Gelfoam into the femoral veins of rabbits ( n = 16). After 2 hours, 16 experimental rabbits and three control rabbits underwent contrast-enhanced dual-energy CT scans, from which PEI and CT pulmonary angiography were created, and planar, SPECT, and SPECT-CT fusion images were then obtained and evaluated. Pathologic determination of locations and numbers of lung lobes with PE were recorded. The sensitivity and specificity of the above-mentioned modalities were calculated using the histopathologic results as reference standards.
Results
Emboli were present in 31 pulmonary lobes and absent in 64 lung lobes in histopathologic analysis. With the histopathologic findings as the gold standard, sensitivities and specificities of PEI, planar, SPECT, and SPECT-CT fusion images to detect PE were 100% and 96.9%, 71.0% and 84.4%, 77.4% and 90.6%, and 74.2% and 93.8%, respectively. McNemar’s tests showed that PEI had higher diagnostic accuracy for the detection of PE than three scintigraphic images (all P values < .05), while three scintigraphic images had similar diagnostic accuracy (all P values = NS).
Conclusions
This study demonstrates that PEI from dual-energy CT imaging can provide higher diagnostic accuracy for detecting PE than planar, SPECT, and SPECT-CT fusion images in a rabbit model.
Pulmonary embolism (PE) is ranked as the third leading cause of death in the United States, with as many as 300,000 fatalities per year . However, an estimated 400,000 diagnoses of PE are missed annually in the United States, largely because of nonspecific clinical signs and symptoms. The accurate diagnosis of PE continues to be a challenge for both clinicians and imaging specialists. Misdiagnosis is critically problematic because death occurs in up to 90% of patients with unrecognized PE, whereas in treated patients, PE accounts for <10% of deaths; furthermore, unnecessary treatment with anticoagulation can place a patient at risk for bleeding .
Imaging techniques, including pulmonary angiography, computed tomographic (CT) imaging, magnetic resonance imaging, and scintigraphy, play an important role in the detection of PE. Of these imaging modalities, pulmonary scintigraphy and CT pulmonary angiography (CTPA) are currently the most widely available and most widely used methods for imaging patients with suspected PE. Multidetector CT (MDCT) pulmonary angiography has been widely used in clinical practice, largely replacing conventional pulmonary angiography and scintigraphy for the evaluation of possible PE; MDCT pulmonary angiography is accepted as the reference standard for the diagnosis of acute PE . The Prospective Investigation of Pulmonary Embolism Diagnosis (PIOPED) II has recommended CTPA as the procedure of choice for the diagnosis of PE . However, many nuclear medicine practitioners have emphasized the merits of single photon-emission CT (SPECT) scintigraphy compared to planar scintigraphy and/or MDCT pulmonary angiography for imaging of PE, citing fewer contraindications, reduced radiation dose, and fewer nondiagnostic findings compared to CTPA as well as improved sensitivity and specificity and fewer nondiagnostic findings compared to planar scintigraphy . Prior studies have also demonstrated that coregistered SPECT-CT fusion images can provide important anatomic and functional information serving as a useful adjunct to CTPA for the diagnosis of acute PE . With recently available dual-source CT scanners, functional and anatomic information can be provided with a single contrast-enhanced dual-energy CT (DECT) scan; DECT methods may overcome the limitations of prior MDCT approaches to improve sensitivity for the detection of PE .
Get Radiology Tree app to read full this article<
Materials and methods
Animal Model
Get Radiology Tree app to read full this article<
DECT Imaging
Imaging protocols
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image reconstruction and analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Perfusion Planar and SPECT Scintigraphy
Imaging protocols
Get Radiology Tree app to read full this article<
Image analysis
Get Radiology Tree app to read full this article<
Coregistered SPECT-CT Imaging
Get Radiology Tree app to read full this article<
Image analysis
Get Radiology Tree app to read full this article<
Pathologic Processing
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Location and Total Number of Pulmonary Emboli Detected for Each Imaging Modality
Modality Right Lung ( n ) Left Lung ( n ) Summary Upper Middle Lower Upper Lower PEI 0 6 (2 ∗ ) 11 3 13 33 Planar scintigraphy 2 (2 ∗ ) 2 (1 ∗ , 3 † ) 11 (3 ∗ , 3 † ) 2 (1 ∗ , 2 † ) 13 (1 ∗ , 1 † ) 30 SPECT 2 (2 ∗ ) 1 (1 ∗ , 4 † ) 13 (3 ∗ , 1 † ) 1 (2 † ) 13 30 SPECT-CT 1 (1 ∗ ) 1 (1 ∗ , 4 † ) 12 (2 ∗ , 1 † ) 1 (2 † ) 12 (1 † ) 27 Histopathology 0 4 11 3 13 31
CT, computed tomography; PEI, pulmonary enhancement imaging; SPECT, single photon-emission computed tomography.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
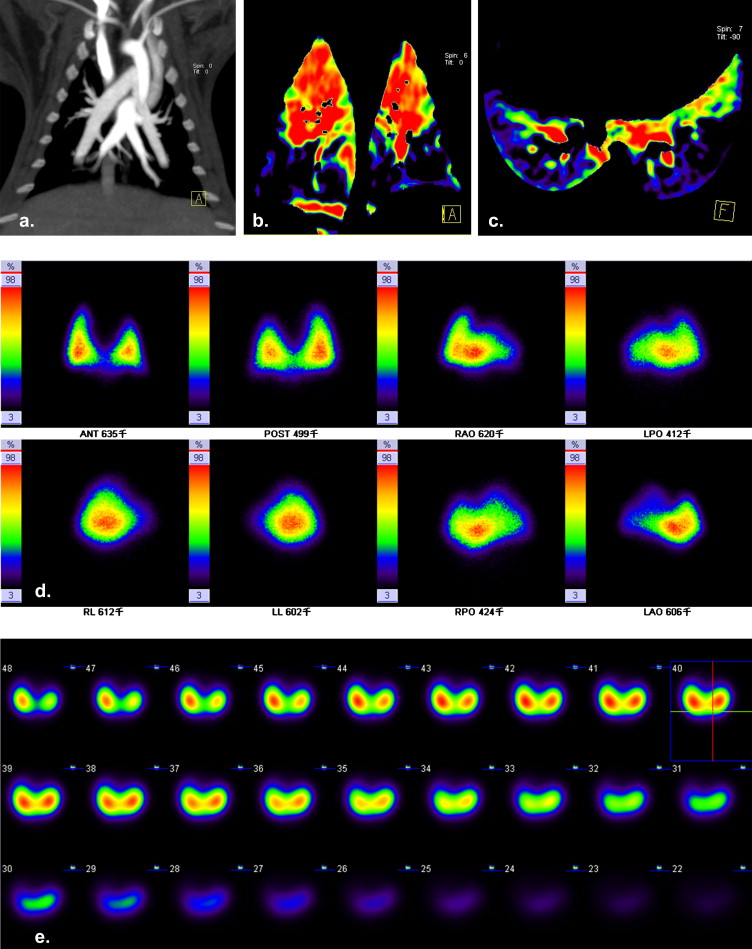
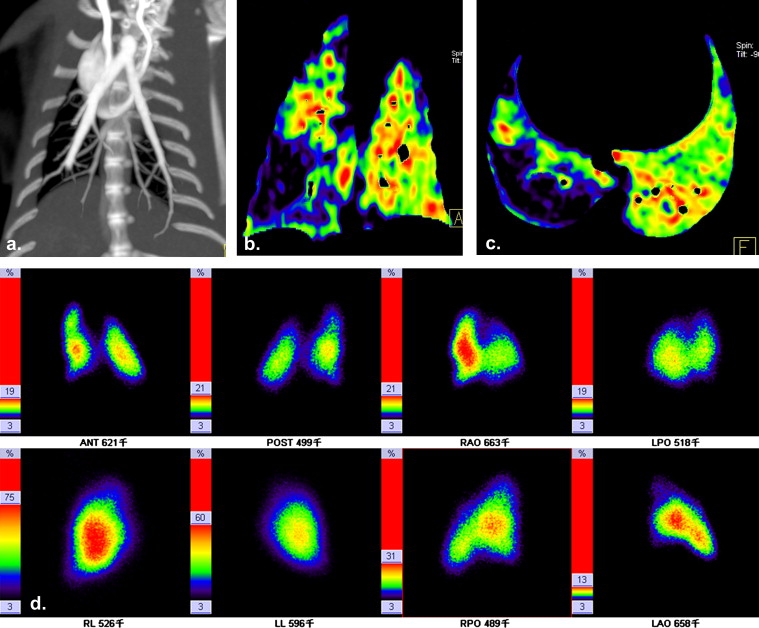
Table 2
Diagnostic Performance of Each Imaging Modality for the Detection of Pulmonary Embolism
Modality Results ( n ) Statistical Analysis (%) TP TN FP FN Sensitivity Specificity PPV NPV Accuracy PEI 31 62 2 0 100 (31/31) 96.9 (62/64) 93.9 (31/33) 100 (62/62) 97.9 (93/95) Planar scintigraphy 22 56 8 9 71.0 (22/31) 84.4 (56/64) 73.3 (22/30) 86.2 (56/65) 82.1 (78/95) SPECT 24 58 6 7 77.4 (24/31) 90.6 (58/64) 80.0 (24/30) 89.2 (58/65) 86.3 (82/95) SPECT-CT 23 60 4 8 74.2 (23/31) 93.8 (60/64) 85.2 (23/27) 88.2 (60/68) 87.4 (83/95)
CT, computed tomography; FN, false-negative results; FP, false-positive results; NPV, negative predictive value; PEI, pulmonary enhancement imaging; PPV, positive predictive value; SPECT, single photon-emission computed tomography; TN, true-negative results; TP, true-positive results.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Acknowledgment
Get Radiology Tree app to read full this article<
References
1. Tapson V.F.: Acute pulmonary embolism. N Engl J Med 2008; 358: pp. 1037-1052.
2. Kuriakose J., Patel S.: Acute pulmonary embolism. Radiol Clin North Am 2010; 48: pp. 31-50.
3. Remy-Jardin M., Pistolesi M., Goodman L.R., et. al.: Management of suspected acute pulmonary embolism in the era of CT angiography: a statement from the Fleischner Society. Radiology 2007; 245: pp. 315-329.
4. Stein P.D., Fowler S.E., Goodman L.R., et. al.: PIOPED II Investigators. Multidetector computed tomography for acute pulmonary embolism. N Engl J Med 2006; 354: pp. 2317-2327.
5. Miles S., Rogers K.M., Thomas P., et. al.: A comparison of SPECT lung scintigraphy and CTPA for the diagnosis of pulmonary embolism. Chest 2009; 136: pp. 1546-1553.
6. Bajc M., Jonson B.: Ventilation/perfusion SPECT—an essential but underrated method for diagnosis of pulmonary embolism and other diseases. Eur J Nucl Med Mol Imaging 2009; 36: pp. 875-878.
7. Zophel K., Bacher-Stier C., Pinkert J., et. al.: Ventilation/perfusion lung scintigraphy: what is still needed? A review considering technetium-99m-labeled macro-aggregates of albumin. Ann Nucl Med 2009; 23: pp. 1-16.
8. Freeman L.M., Haramati L.B.: V/Q scintigraphy: alive, well and equal to the challenge of CT angiography. Eur J Nucl Med Mol Imaging 2009; 36: pp. 499-504.
9. Reid J.H., Coche E.E., Inoue T., et. al., International Atomic Energy Agency Consultants’ Group: Is the lung scan alive and well? Facts and controversies in defining the role of lung scintigraphy for the diagnosis of pulmonary embolism in the era of MDCT. Eur J Nucl Med Mol Imaging 2009; 36: pp. 505-521.
10. Roach P.J., Bailey D.L., Schembri G.P.: Reinventing ventilation/perfusion lung scanning with SPECT. Nucl Med Commun 2008; 29: pp. 1023-1025.
11. Bajc M., Olsson B., Palmer J., et. al.: Ventilation/Perfusion SPECT for diagnostics of pulmonary embolism in clinical practice. J Intern Med 2008; 264: pp. 379-387.
12. Roach P.J., Thomas P., Bajc M., et. al.: Merits of V/Q SPECT scintigraphy compared with CTPA in imaging of pulmonary embolism. J Nucl Med 2008; 49: pp. 167-168.
13. Bajc M., Olsson C.G., Olsson B., et. al.: Diagnostic evaluation of planar and tomographic ventilation/perfusion lung images in patients with suspected pulmonary emboli. Clin Physiol Funct Imaging 2004; 24: pp. 249-256.
14. Reinartz P., Wildberger J.E., Schaefer W., et. al.: Tomographic imaging in the diagnosis of pulmonary embolism: a comparison between V/Q lung scintigraphy in SPECT technique and multislice spiral CT. J Nucl Med 2004; 45: pp. 1501-1508.
15. Suga K., Kawakami Y., Zaki M., et. al.: Pulmonary perfusion assessment with respiratory gated 99mTc macroaggregated albumin SPECT: preliminary results. Nucl Med Commun 2004; 25: pp. 183-193.
16. Collart J.P., Roelants V., Vanpee D., et. al.: Is a lung perfusion scan obtained by using single photon emission computed tomography able to improve the radionuclide diagnosis of pulmonary embolism?. Nucl Med Commun 2002; 23: pp. 1107-1113.
17. Bajc M., Bitzén U., Olsson B., et. al.: Lung ventilation/perfusion SPECT in the artificially embolized pig. J Nucl Med 2002; 4: pp. 640-647.
18. Bajc M., Neilly J.B., Miniati M., et. al.: EANM guidelines for ventilation/perfusion scintigraphy: part 2. Algorithms and clinical considerations for diagnosis of pulmonary emboli with V/P (SPECT) and MDCT. Eur J Nucl Med Mol Imaging 2009; 36: pp. 1528-1538.
19. Gutte H., Mortensen J., Jensen C.V., et. al.: Comparison of V/Q SPECT and planar V/Q lung scintigraphy in diagnosing acute pulmonary embolism. Nucl Med Commun 2010; 31: pp. 82-86.
20. Gutte H., Mortensen J., Jensen C.V., et. al.: Detection of pulmonary embolism with combined ventilation-perfusion SPECT and low-dose CT: head-to-head comparison with multidetector CT angiography. J Nucl Med 2009; 50: pp. 1987-1992.
21. Stein P.D., Freeman L.M., Sostman H.D., et. al.: SPECT in acute pulmonary embolism. J Nucl Med 2009; 50: pp. 1999-2007.
22. Suga K., Yasuhiko K., Iwanaga H., et. al.: Relation between lung perfusion defects and intravascular clots in acute pulmonary thromboembolism: assessment with breath-hold SPECT-CT pulmonary angiography fusion images. Eur J Radiol 2008; 67: pp. 472-480.
23. Suga K., Kawakami Y., Iwanaga H., et. al.: Automated breath-hold perfusion SPECT/CT fusion images of the lungs. AJR Am J Roentgenol 2007; 189: pp. 455-463.
24. Fink C., Johnson T.R., Michaely H.J., et. al.: Dual-energy CT angiography of the lung in patients with suspected pulmonary embolism: initial results. Rofo 2008; 180: pp. 879-883.
25. Pontana F., Faivre J.B., Remy-Jardin M., et. al.: Lung perfusion with dual-energy multidetector-row CT (MDCT): feasibility for the evaluation of acute pulmonary embolism in 117 consecutive patients. Acad Radiol 2008; 15: pp. 1494-1504.
26. Thieme S.F., Becker C.R., Hacker M., et. al.: Dual energy CT for the assessment of lung perfusion—correlation to scintigraphy. Eur J Radiol 2008; 68: pp. 369-374.
27. Miniati M., Pistolesi M., Marini C., et. al.: Value of perfusion lung scan in the diagnosis of pulmonary embolism: results of the Prospective Investigative Study of Acute Pulmonary Embolism Diagnosis (PISA-PED). Am J Respir Crit Care Med 1996; 154: pp. 1387-1393.
28. Sostman H.D., Miniati M., Gottschalk A., et. al.: Sensitivity and specificity of perfusion scintigraphy combined with chest radiography for acute pulmonary embolism in PIOPED II. J Nucl Med 2008; 49: pp. 1741-1748.
29. Sostman H.D., Stein P.D., Gottschalk A., et. al.: Acute pulmonary embolism: sensitivity and specificity of ventilation-perfusion scintigraphy in PIOPED II study. Radiology 2008; 246: pp. 941-946.
30. Zhang L.J., Zhao Y.E., Wu S.Y., et. al.: Pulmonary embolism detection with dual-energy CT: experimental study of dual-source CT in rabbits. Radiology 2009; 252: pp. 61-70.
31. Zhang L.J., Chai X., Wu S.Y., et. al.: Detection of pulmonary embolism by dual energy CT: correlation with perfusion scintigraphy and histopathological findings in rabbits. Eur Radiol 2009; 19: pp. 2844-2854.
32. Hoey E.T., Gopalan D., Screaton N.J.: Dual-energy CT pulmonary angiography: a new horizon in the imaging of acute pulmonary thromboembolism. AJR Am J Roentgenol 2009; 192: pp. W341-W342.
33. Zhang L.J., Yang G.F., Zhao Y.E., et. al.: Detection of pulmonary embolism using dual-energy computed tomography and correlation with cardiovascular measurements: a preliminary study. Acta Radiol 2009; 50: pp. 892-901.
34. Tunariu N., Gibbs S.J., Win Z., et. al.: Ventilation-perfusion scintigraphy is more sensitive than multidetector CTPA in detecting chronic thromboembolic pulmonary disease as a treatable cause of pulmonary hypertension. J Nucl Med 2007; 48: pp. 680-684.