
Rationale and Objectives
Pulmonary vascular complications of liver disease have a substantial impact on morbidity and mortality in patients who undergo liver transplant. The effect of liver transplantation on the pulmonary vasculature in patients without pulmonary vascular disease, however, has not been described. This study was undertaken to characterize the regional effect of liver transplant on the cross-sectional area (CSA) of pulmonary vessels.
Materials and Methods
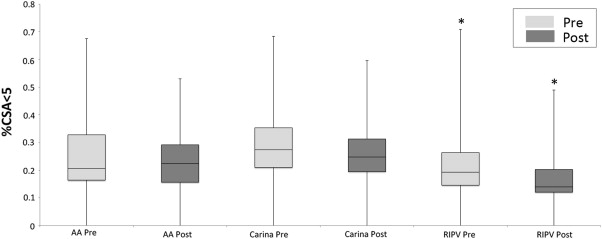
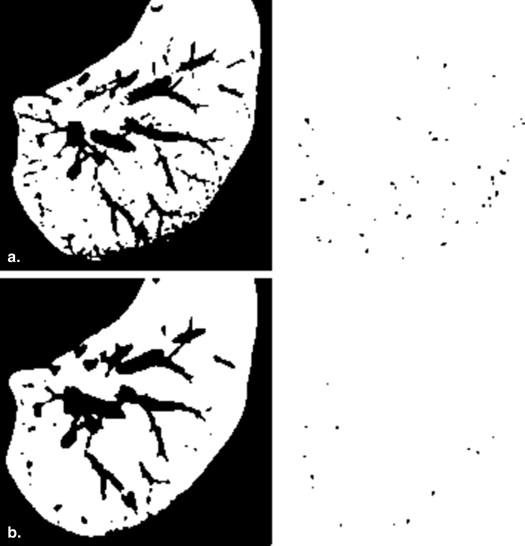
We performed a single-center, retrospective, cohort study of patients who had a liver transplant between 2002 and 2012 and who had chest computed tomography scans within 1 year before and after transplant. Using ImageJ software, we measured the CSA of small pulmonary vessels (0–5 mm 2 ) and the total lung CSA to calculate the percent CSA of pulmonary vessels <5 mm (%CSA<5) at the level of the aortic arch, carina, and right inferior pulmonary vein (RIPV). Pretransplant and posttransplant, %CSA<5 were compared, and associations of pretransplant %CSA<5 with clinical parameters were measured.
Results
There was a significant decrease in %CSA<5 at the level of the RIPV (0.19% [interquartile range {IQR}, 0.15–0.26] before vs. 0.15% [IQR, 0.12–0.21] after; P = .0003), with a median change of −16.2% (IQR, −39.3 to 3.9) posttransplant. Changes at the level of the aortic arch and carina were not significant. Pretransplant RIPV %CSA<5 was not significantly correlated with severity of liver disease or oxygenation but was inversely correlated with percent change in %CSA<5 (r = −0.39; P = .0039).
Conclusions
This is the first study to describe a significant regional change in the pulmonary vessels of patients without known pulmonary vascular disease who undergo liver transplant.
Pulmonary vascular complications of liver disease, such as hepatopulmonary syndrome (HPS) and portopulmonary hypertension (POPH), have a substantial impact on morbidity and mortality in patients with cirrhosis and portal hypertension , but the relationship between the liver and the pulmonary vasculature remains poorly understood. HPS, characterized by intrapulmonary vascular dilation, and POPH, characterized by elevated pulmonary arterial pressure and pulmonary vascular resistance, also have implications for postoperative outcomes in liver transplantation . The current Model for End Stage Liver Disease (MELD) exception policy highlights the importance of these pulmonary vascular complications by favoring organ allocation to expedite liver transplantation in patients who meet certain criteria for HPS or POPH . Outcomes of these diseases with liver transplant, however, are variable. HPS typically improves with liver transplant , whereas outcomes of POPH are more unpredictable . Even less is known about the effect of liver transplantation on the pulmonary vasculature in patients with liver disease who do not meet criteria for HPS or POPH.
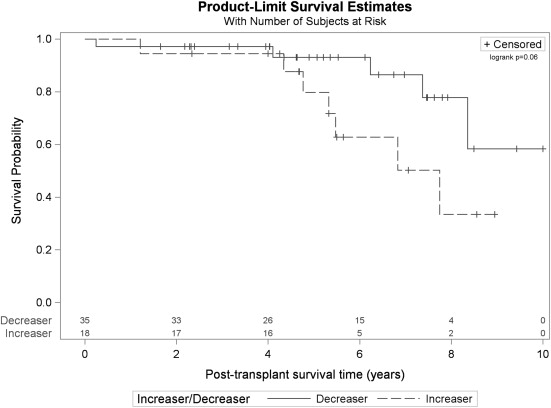
This study was undertaken to further characterize the effect of liver transplant on the cross-sectional area (CSA) of small pulmonary vessels in a cohort of patients with cirrhosis and portal hypertension. Because diseases such as HPS have a basilar predominance, we also sought to determine the regional effect of liver transplant on pulmonary vessel CSA at three anatomic levels. Additionally, we wanted to characterize the relationship between pretransplant CSA and clinical parameters such as liver disease severity determined by the MELD score, etiology of liver disease, percent predicted diffusion capacity for carbon monoxide corrected for hemoglobin (%DLCO[Hb]), arterial partial pressure of oxygen (PaO2), and alveolar–arterial oxygen (A-a) gradient, as well as mortality. Finally, we wanted to determine if there was a difference in mortality between patients who had an increase versus a decrease in percent CSA of pulmonary vessels <5 mm 2 (%CSA<5) with transplant.
Materials and methods
Study Design and Subject Selection
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
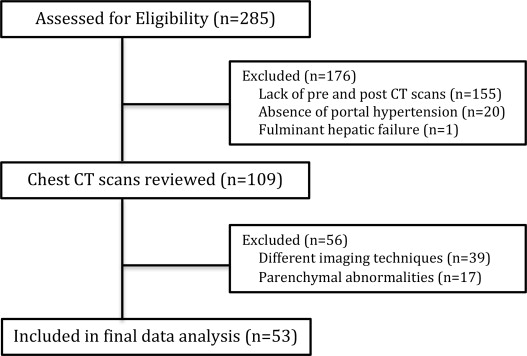
Table 1
Patient Characteristics
Characteristic % (n) or Median (IQR) Male 85 (45) Age (years) 56 (51–61) Race/ethnicity Caucasian 72 (38) Hispanic/Latino 11 (6) Asian 7.5 (4) African American 2 (1) Not specified 7.5 (4) Comorbidities Hepatocellular carcinoma 87 (46) Diabetes mellitus 34 (18) Hypertension 28 (15) HIV 6 (3) Asthma 6 (3) COPD 2 (1) Etiology of liver disease Hepatitis C 53 (28) Alcohol 17 (9) Hepatitis C and alcohol 9 (5) Hepatitis B 11 (6) Nonalcoholic steatohepatitis 4 (2) Autoimmune 2 (1) Other 4 (2) Laboratory MELD score 12 (9–16)
COPD, chronic obstructive pulmonary disease; HIV, human immunodeficiency virus; MELD, Model for End Stage Liver Disease.
Data expressed as % ( n ) or median (interquartile range).
Get Radiology Tree app to read full this article<
Imaging
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Percent Cross-sectional Area of 0–5 mm 2 Pulmonary Vessels
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Correlation with Clinical Parameters
Get Radiology Tree app to read full this article<
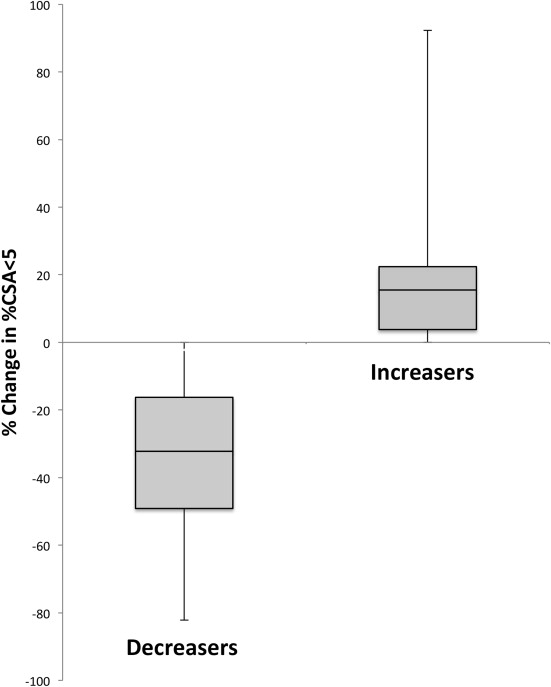
%CSA<5 Decreasers versus Increasers
Get Radiology Tree app to read full this article<
Table 2
Comparison of Patients Who Had a Decrease in %CSA<5 Posttransplant (Decreasers) to Those Who Had an Increase in %CSA<5 Posttransplant (Increasers)
Characteristic Decreasers ( n = 35) Increasers ( n = 18)P Value Male 88.5 (31) 78 (14) .30 Age (years) 57.0 (51.5–62.9) 53.5 (49.5–56.9) .07 Race/ethnicity .25 Caucasian 71 (25) 72 (13) Hispanic/Latino 6 (2) 22 (4) Asian 11 (4) 0 African American 3 (1) 0 Not specified 9 (3) 6 (1) Comorbidities Hepatocellular carcinoma 86 (30) 89 (16) Diabetes mellitus 31 (11) 39 (7) Hypertension 29 (10) 28 (5) HIV 6 (2) 6 (1) Asthma 3 (1) 11 (2) COPD 3 (1) 0 Etiology of liver disease .63 Hepatitis C 51 (18) 56 (10) Alcohol 14 (5) 17 (3) Hepatitis C and alcohol 8.5 (3) 17 (3) Hepatitis B 14 (5) 7 (1) Nonalcoholic steatohepatitis 6 (2) 0 Autoimmune 0 7 (1) Other 6 (2) 0 Laboratory MELD score 12 (9–21) 12 (10–15) .81 Percent change in %CSA<5 −32.2 (−49.1 to −16.2) 15.5 (3.8–22.4) <.0001 PaO2 (mm Hg) 86 (80–92) ( n = 31) 90 (88–102) ( n = 12) .09 A-a gradient 17 (12–26) ( n = 31) 14 (8–16) ( n = 12) .4 DLCO[Hb] (% predicted) 82 (63–91) ( n = 33) 84 (72–94) ( n = 18) .87 Unadjusted all-cause # deaths/100 person years (2002–2013) 2.7/100 person years (5) 7.2/100 person years (7) .08
A-a, alveolar–arterial oxygen; COPD, chronic obstructive pulmonary disease; %CSA<5, cross-sectional area of pulmonary vessels <5 mm; DLCO[Hb], diffusion capacity for carbon monoxide corrected for hemoglobin; HIV, human immunodeficiency virus; MELD, Model for End Stage Liver Disease; PaO2, partial pressure of oxygen.
Data expressed as % ( n ) or median (interquartile range).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Potential Mechanisms
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Considerations in Hepatopulmonary Syndrome
Get Radiology Tree app to read full this article<
Mortality
Get Radiology Tree app to read full this article<
Limitations
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Krowka M.J., Miller D.P., Barst R.J., et. al.: Portopulmonary hypertension: a report from the US-based REVEAL registry. Chest 2012; 41: pp. 906-915.
2. Fallon M.B., Krowka M.J., Brown R.S., et. al.: Impact of hepatopulmonary syndrome on quality of life and survival in liver transplant candidates. Gastroenterology 2008; 135: pp. 1168-1175.
3. Swanson K.L., Wiesner R.H., Krowka M.J.: Natural history of hepatopulmonary syndrome: impact of liver transplantation. Hepatology 2005; 41: pp. 1122-1129.
4. Krowka M.J., Wiesner R.H., Heimbach J.K.: Pulmonary contraindications, indication and MELD exceptions for liver transplantation: a contemporary view and look forward. J Hepatol 2013; 59: pp. 367-374.
5. Fritz J.S., Fallon M.B., Kawut S.M.: Pulmonary vascular complications of liver disease. Am J Respir Crit Care Med 2013; 187: pp. 133-143.
6. Eriksson L.S., Söderman C., Ericzon B.G., et. al.: Normalization of ventilation/perfusion relationships after liver transplantation in patients with decompensated cirrhosis: evidence for a hepatopulmonary syndrome. Hepatology 1990; 12: pp. 1350-1357.
7. Lange P.A., Stoller J.K.: The hepatopulmonary syndrome. Effect of liver transplantation. Clin Chest Med 1996; 17: pp. 115-123.
8. Taille C., Cadranel J., Bellocq A., et. al.: Liver transplantation for hepatopulmonary syndrome: a ten-year experience in Paris, France. Transplantation 2003; 75: pp. 1482-1489.
9. Matsuoka S., Washko G.R., Yamashiro T., et. al.: Pulmonary hypertension and computed tomography measurement of small pulmonary vessels in severe emphysema. Am J Respir Crit Care Med 2010; 181: pp. 218-225.
10. Kowalski H.J., Abelmann W.H.: The cardiac output at rest in Laennec’s cirrhosis. J Clin Invest 1953; 32: pp. 1025-1033.
11. Groszmann R.J.: Hyperdynamic circulation of liver disease 40 years later: pathophysiology and clinical consequences. Hepatology 1994; 20: pp. 1359-1363.
12. Moller S., Henrikson J.H.: Cirrhotic cardiomyopathy: a pathophysiological review of circulatory dysfunction in liver disease. Heart 2002; 87: pp. 9-15.
13. Glauser F.L.: Systemic hemodynamic and cardiac function changes in patients undergoing orthotopic liver transplantation. Chest 1990; 98: pp. 1210-1215.
14. Piscaglia F., Zironi G., Gaiani S., et. al.: Systemic and splanchnic hemodynamic changes after liver transplantation for cirrhosis: a long-term prospective study. Hepatology 1999; 30: pp. 58-64.
15. Navasa M., Feu F., Garcva-Pagan J.C., et. al.: Hemodynamic and humoral changes after liver transplantation in patients with cirrhosis. Hepatology 1993; 17: pp. 355-360.
16. Gadano A., Hadengue A., Widmann J.J., et. al.: Hemodynamics after orthotopic liver transplantation: study of associated factors and long-term effects. Hepatology 1995; 22: pp. 458-465.
17. El-Sherif A.M., Abou-Shady M.A., Al-Bahrawy A.M., et. al.: Exhaled nitric oxide levels in chronic liver disease patients with and without esophageal varices. Hepatol Int 2008; 2: pp. 341-345.
18. Martin P., Gines P., Schrier R.: Nitric oxide as a mediator of hemodynamic abnormalities and sodium and water retention in cirrhosis. N Engl J Med 1998; 339: pp. 533-541.
19. Vallance P., Moncada S.: Hyperdynamic circulation in cirrhosis: a role for nitric oxide?. Lancet 1991; 337: pp. 776-778.
20. Rolla G., Brussino L., Colagrande P., et. al.: Exhaled nitric oxide levels and oxygenation abnormalities in hepatic cirrhosis. Hepatology 1997; 26: pp. 842-847.
21. Pascasio J.M., Grillo I., Lopez-Pardo F.J., et. al.: Prevalence and severity of hepatopulmonary syndrome and its influence on survival in cirrhotic patients evaluated for liver transplantation. Am J Transplant 2014; 14: pp. 1391-1399.