
Rationale and Objectives
Evaluate quantification of the aortic regurgitant fraction and volume with computed tomography (CT).
Materials and Methods
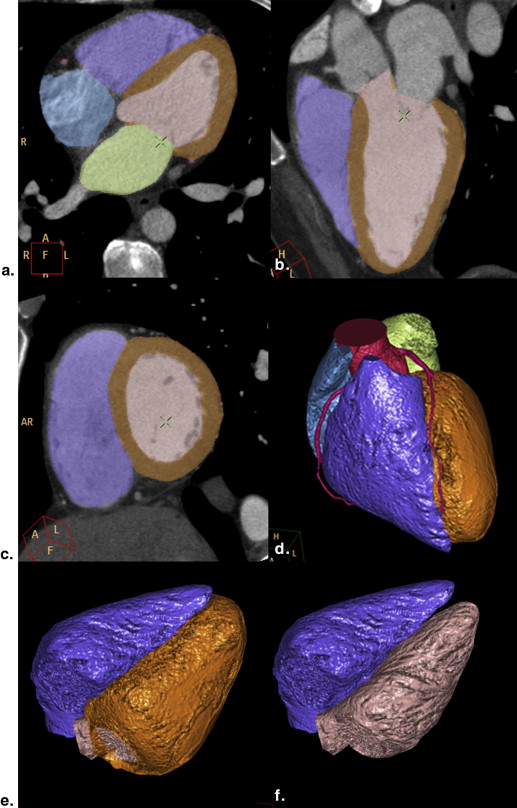
Fifty-three patients with aortic regurgitation (AR) and 29 controls were examined with 64-multi-detector CT coronary angiography and transthoracic echocardiography (TTE). A dedicated software algorithm employing three-dimensional segmentation of left ventricle (LV) and right ventricle (RV) volumes and LV mass was applied. AR volume and fraction was calculated based on RV and LV stroke volumes (SV) and compared with echocardiography. The aortic regurgitant orifice area (ROA) was measured by CT.
Results
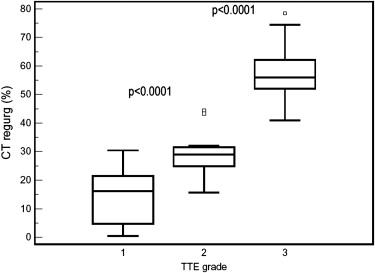
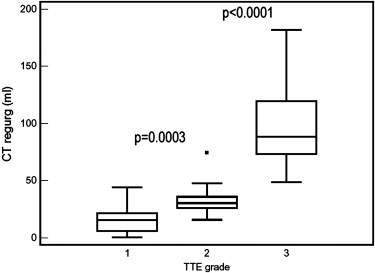
A good correlation of the AR fraction and AR volume determined by CT compared to echocardiography was found for mild, moderate, and severe AR with 14.2% ± 9, 28.8% ± 8, and 57.9% ± 9 ( r = 0.95, P < .001) for AR fraction, and 15.7 mL ± 11.33 mL ± 14, and 98.9 mL ± 36 for AR volume ( r = 0.92, P < .0001), respectively. CT correctly classified severity of AR in 93% of patients based of AR-fraction, and in 89% based on AR volume. The sensitivity and specificity of CT were 98% and specificity 90.3%. The specificity improved to 97%, if the ROA by CT was added as diagnostic criterion.
Conclusion
Aortic regurgitation fraction and volume can be accurately quantified from CT coronary angiography datasets. These parameters can assist clinical management, e.g. in case of pending cardiac surgery decision.
The prognosis of patients with chronic aortic regurgitation (AR) depends on determining the optimal time point of aortic valve surgery. There is consensus that surgery is indicated in symptomatic patients with severe AR, but controversy exists regarding the management and timing of surgery in asymptomatic or mildly symptomatic patients .
In these patients, the indication for surgery is based on accurately staging severity of AR and on identifying early signs of left ventricular (LV) dysfunction or pathological ventricular dilatation. LV ejection fraction (EF) is an independent predictor of overall survival besides the AR severity ; however, left ventricular ejection fraction (LVEF) is not the most sensitive parameter to identify early signs of impaired contractile dysfunction .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Study Population and Design
Get Radiology Tree app to read full this article<
Inclusion criteria
Get Radiology Tree app to read full this article<
Exclusion criteria
Get Radiology Tree app to read full this article<
CT Examination Technique
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Postprocessing
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TTE
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Study Population (82 Patients)
Age (y) 58 ± 16 (range, 31–87) Gender ( n ) 29 females (35%) Body surface area (m 2 ) 1.8 ± 0.3 (1.4–2.4) Height (cm) 172 ± 7.7 (157–193) Weight (kg) 74 ± 12.8 (43–111) Aortic regurgitation grade by TTE Mild (n/n, %) 19/53 (36%) Moderate (n/n, %) 15/53 (28%) Severe (n/n, %) 19/53 (36%) Normal (control) (n) 29 Functional anatomy of AR (types 1–3 ∗ ) (53 patients) Type 1 (root dilatation) 25 (47%) Type 2 (cusp prolapsed) 6 (11.3%) Type 3 (IE or restrictive) † 3 (5.6%) None of above (eg, degenerative-asymmetric valve closure) 17 (32%) Aortic dissection 2 (3.8%) Aortic root size (cm) 3.5 ± 0.7 (range, 1.9–6.3) Concomitant aortic stenosis 17/53 (32%) Mild AR 15/19 (79%) Moderate AR 2/15 (1.3%) Severe AR 0/19 (0%)
AR, aortic regurgitation; IE, infective endocarditis; TTE, transthoracic echocardiography.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Quantification of AR
Get Radiology Tree app to read full this article<
Table 2
Aortic Regurgitant Fraction, Volume, and the Anatomic Regurgitant Orifice Area (ROA): CT versus TTE
Aortic Regurgitation TTE n = 53 Control
Group
n = 29P Value ∗ Mild
n = 19 Moderate
n = 16 Severe
n = 19 CT AR-fract (%) 14.2 ± 9 28.8 ± 8 57.9 ± 9 −0.4 ± 7 <.001 AR vol (mL) 15.7 ± 11 32.8 ± 3.8 98.9 ± 36 0.5 ± 7 <.001 Correct graduationby AR fract%(n/n, %) 19/19 (100%) 12/15 (80%) 18/19 (94.8%) 26/31 (84%) Correct graduation byAR vol (n/n, %) 18/19 (94.8%) 12/15 (80%) 17/19 (89.5%) 26/31 (84%) ROA (cm 2 ) 0.09 ± 0.1 (range, 0–0.46) 0.4 ± 0.1 (range, 0.38–64) 0.80 ± 0.4 (range,0.32–1.53)
AR vol, aortic regurgitant volume; AR-fract, aortic regurgitant fraction; ROA, regurgitation orifice area.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Quantification of LV and RV Volumes, Function, and Myocardial Mass
Get Radiology Tree app to read full this article<
Table 3
LV and RV Volume, Function, and Myocardial Mass
Aortic Regurgitationby TTE n = 53 Control
Group
n = 29P Value Mild
n = 19 Moderate
n = 16 Severe
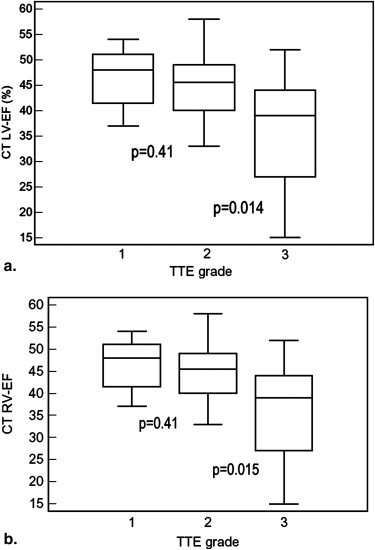
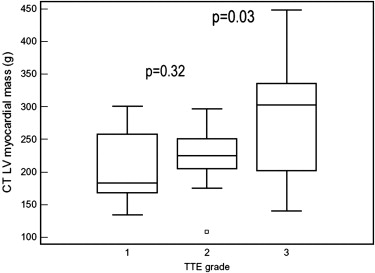
n = 19 Total in AR CT LVESV (mL) 59.4 ± 5 83 ± 14 142 ± 16 96 ± 62 60 ± 18 <.001 ∗ LVEDV (mL) 162 ± 36 194 ± 52 312 ± 99 224.5 ± 96 147 ± 24 .001 LVSV (mL) 101 ± 22 111 ± 22 161 ± 51 129 ± 47 87 ± 16 <.001 ∗ LVEF (%) 63 ± 9 59 ± 14 55 ± 12 59.5 ± 12 60.6 ± 8 .69 RVEDV (mL) 181 ± 33 175 ± 29 195 ± 56 184 ± 42 170 ± 31 .188 RVESV (mL) 97 ± 21 96 ± 23 116 ± 36 104 ± 36 86 ± 21 .03 ∗ RVSV (mL) 84 ± 21 87 ± 23 81 ± 53 78 ± 20 84 ± 16 .243 RVEF (%) 46 ± 5 44 ± 6 37 ± 10 42 ± 9 51 ± 6 <.001 ∗ LV mass (g) 205 ± 41 223 ± 59 287 ± 91 240 ± 46 139 ± 10 <.001
CT, computed tomography; EDV, end-diastolic volume; EF, ejection fraction; ESV, end-systolic volume; LV, left ventricular; RV, right ventricular.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Limitations
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Bonow R.O., Carabello B.A., Chatterjee K., et. al.: ACC/AHA 2006 guidelines for the management of patients with valvular heart disease. J Am Coll Cardiol 2006; 48: pp. e1-e148.
2. Dujardin K.S., Enriquez-Sarano M., Schaff H.V., et. al.: Mortality and morbidity of aortic regurgitation in clinical practice. A long-term follow-up study. Circulation 1999; 99: pp. 1851-1857.
3. Taniguchi K., Nakano S., Kawashima Y., et. al.: Left ventricular ejection performance, wall stress, and contractile state in aortic regurgitation before and after aortic valve replacement. Circulation 1990; 82: pp. 798-807.
4. Miyake Y., Hozumi T., Mori I., et. al.: Automated quantification of aortic regurgitant volume and regurgitant fraction using the digital colour Doppler velocity profile integration method in patients with aortic regurgitation. Heart 2002; 88: pp. 481-484.
5. Detaint D., Messika-Zeitoun D., Maalouf J., et. al.: Quantitative echocardiographic determinants of clinical outcome in asymptomatic patients with aortic regurgitation: a prospective study. JACC Cardiovasc Imaging 2008; 1: pp. 1-11.
6. Budoff M.J., Dowe D., Jollis J.G., et. al.: Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial. J Am Coll Cardiol 2008; 52: pp. 1724-1732.
7. Janne d’Othée B., Siebert U., Cury R., et. al.: A systematic review on diagnostic accuracy of CT-based detection of significant coronary artery disease. Eur J Radiol 2008; 65: pp. 449-641.
8. Meijboom W.B., Mollet N.R., Van Mieghem C.A., et. al.: Pre-operative computed tomography coronary angiography to detect significant coronary artery disease in patients referred for cardiac valve surgery. J Am Coll Cardiol 2006; 48: pp. 1658-1665.
9. Scheffel H., Leschka S., Plass A., et. al.: Accuracy of 64-slice computed tomography for the preoperative detection of coronary artery disease in patients with chronic aortic regurgitation. Am J Cardiol 2007; 100: pp. 701-706.
10. Alkadhi H., Desbiolles L., Husmann L., et. al.: Aortic regurgitation: assessment with 64-Section CT. Radiology 2007; 245: pp. 111-121.
11. Feuchtner G.M., Dichtl W., Schachner T., et. al.: Diagnostic performance of multidetector CT in detecting aortic valve regurgitation. AJR Am J Roentgenol 2006; 186: pp. 1676-1681.
12. Feuchtner G.M., Dichtl W., Müller S., et. al.: 64-MDCT for diagnosis of aortic regurgitation in patients referred to CT coronary angiography. AJR Am J Roentgenol 2008; 1: pp. W1-W7.
13. Jassal D.S., Shapiro M.D., Neilan T.G., et. al.: 64-slice multidetector computed tomography (MDCT) for detection of aortic regurgitation and quantification of severity. Invest Radiol 2007; 42: pp. 507-512.
14. Li X., Tang L., Zhou L., et. al.: Aortic valves stenosis and regurgitation: assessment with dual source computed tomography. Int J Cardiovasc Imaging 2009; 25: pp. 591-600.
15. Dewey M., Müller M., Eddicks S., et. al.: Evaluation of global and regional left ventricular function with 16-slice computed tomography, biplane cineventriculography, and two-dimensional transthoracic echocardiography: comparison with magnetic resonance imaging. J Am Coll Cardiol 2006; 48: pp. 2034-2044.
16. Abadi S., Roguin A., Engel A., et. al.: Feasibility of automatic assessment of four-chamber cardiac function with MDCT: initial clinical application and validation. Eur J Radiol 2009 Mar 2; (Epub ahead of print)
17. Hendel R.C., Patel M.R., Cramer C.M., et. al.: ACCF/ACR/SCCT/SCMR/ASNC/NASCI/SCAI/SIR 2006. Appropriateness criteria for cardiac computed tomography and cardiac magnetic resonance imaging. J Am Coll Cardiol 2006; 48: pp. 1475-1497.
18. Cheitlin M.D., Alpert J.S., Armstrong W.F., et. al.: ACC/AHA guidelines for the clinical application of echocardiography. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Clinical Application of Echocardiography). Developed in collaboration with the American Society of Echocardiography. Circulation 1997; 95: pp. 1686-1744.
19. Scheffel H., Alkadhi H., Leschka S., et. al.: Low-dose CT coronary angiography in the step-and-shoot mode: diagnostic performance. Heart 2008 Jun 2; (Epub ahead of print)
20. Reiter S.J., Rumberger J.A., Stanford W., et. al.: Quantitative determination of aortic regurgitant volumes in dogs by ultrafast computed tomography. Circulation 1987; 76: pp. 728-735.
21. Rosen B.D., Edvardsen T., Lai S., et. al.: Left ventricular concentric remodeling is associated with decreased global and regional systolic function: the Multi-Ethnic Study of Atherosclerosis. Circulation 2005; 112: pp. 984-991.
22. Taniguchi K., Takahashi T., Toda K., et. al.: Left ventricular mass: impact on left ventricular contractile function and its reversibility in patients undergoing aortic valve replacement. Eur J Cardiothorac Surg 2007; 32: pp. 588-595.
23. Pattynama P.M., Lamb H.J., Van der Velde E.A., et. al.: Reproducibility of MRI-derived measurements of right ventricular volumes and myocardial mass. Magn Reson Imaging 1995; 3: pp. 53-63.
24. Bruners P., Mahnken A.H., Knackstedt C., et. al.: Assessment of global left and right ventricular function using dual-source computed tomography (DSCT) in comparison to MRI: an experimental study in a porcine model. Invest Radiol 2007; 42: pp. 756-764.
25. Dourvas I.N., Parharidis G.E., Efthimiadis K., et. al.: Right ventricular diastolic function in patients with chronic aortic regurgitation. Am J Cardiol 2004; 93: pp. 115-117.
26. Abbara S., Chow B.J., Pena A.J., et. al.: Assessment of left ventricular function with 16- and 64-slice multidetector computed tomography. Eur J Radiol 2008; 67: pp. 481-486.
27. Annuar B.R., Liew C.K., Chin S.P., et. al.: Assessment of global and regional left ventricular function using 64-slice multislice computed tomography and 2D echocardiography: a comparison with cardiac magnetic resonance. Eur J Radiol 2008; 65: pp. 112-119.
28. Wu Y.W., Tadamura E., Kanao S., et. al.: Left ventricular functional analysis using 64-slice multidetector row computed tomography: comparison with left ventriculography and cardiovascular magnetic resonance. Cardiology 2007; 109: pp. 135-142.
29. van der Vleuten P.A., Willems T.P., Götte M.J., et. al.: Quantification of global left ventricular function: comparison of multidetector computed tomography and magnetic resonance imaging. A meta-analysis and review of the current literature. Acta Radiol 2006; 47: pp. 1049-1057.
30. Belge B., Coche E., Pasquet A., et. al.: Accurate estimation of global and regional cardiac function by retrospectively gated multidetector row computed tomography: comparison with cine magnetic resonance imaging. Eur Radiol 2006; 16: pp. 1424-1433.
31. Mor-Avi V., Sugeng L., Weinert L., et. al.: Fast measurement of left ventricular mass with real-time three-dimensional echocardiography: comparison with magnetic resonance imaging. Circulation 2004; 110: pp. 1814-1818.
32. Hausleiter J., Meyer T., Hadamitzky M., et. al.: Radiation dose estimates from cardiac multislice computed tomography in daily practice: impact of different scanning protocols on effective dose estimates. Circulation 2006; 113: pp. 1305-1310.
33. Stolzmann P., Scheffel H., Schertler T., et. al.: Radiation dose estimates in dual-source computed tomography coronary angiography. Eur Radiol 2008; 18: pp. 592-599.
34. Waroux de Polain J.B., Pouleur A.C., Goffinet C., et. al.: Functional anatomy of aortic regurgitation: accuracy, prediction of surgical repairablity, and outcome implications of transesophaeal echocardioraphy. Circulation 2007; 116: pp. 264-269.
35. Cawley P., Maki J., Catherine O.M.: Cardiovascular magnetic resonance imaging for valvular heart disease: technique and validation. Circulation 2009; 119: pp. 468-478.
36. Bettencourt N., Rocha J., Carvalho M., et. al.: Multislice computed tomography in the exclusion of coronary artery disease in patients with presurgical valve disease. Circulation Cardiovasc Imaging 2009; 2: pp. 306-313.
37. Feuchtner G.M., Alkadhi H., Karlo C., et. al.: Cardiac CT angiography for the diagnosis of mitral valve prolapse: comparison with echocardiography. Radiology 2010; 254: pp. 374-383.