
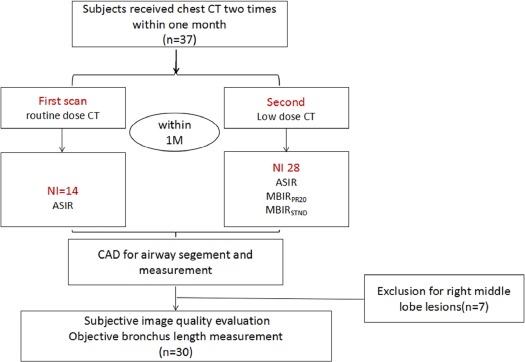
Objective
We aimed to evaluate a new model-based iterative reconstruction (MBIRn) algorithm either with spatial resolution and noise reduction balance (MBIR STND ) or spatial resolution preference (MBIR RP20 ) for quantitative analysis of airway in low-dose chest computed tomography (CT) with a computer-aided detection (CAD) software, in comparison to adaptive statistical iterative reconstruction (ASIR) in routine-dose CT.
Methods
Thirty patients who underwent both the routine-dose (noise index [NI] = 14 HU) and low-dose (at 30% level with NI = 28 HU) CT examination for pulmonary disease were included. Image acquisition was performed with 120 kVp tube voltage and automatic tube current modulation. Routine-dose scans were reconstructed with ASIR, whereas low-dose scans were reconstructed with ASIR, MBIR STND , and MBIR RP20 . Airway dimensions of the right middle lobe bronchus from the four reconstructions were measured using CAD software. Two radiologists used a semiquantitative 5 scoring criteria (−2, inferior to; +2, superior to; −1 slightly inferior to; +1, slightly superior to; and 0, equal to ASIR in routine-dose CT) to rate the subjective image quality of MBIR STND and MBIR RP20 of airway trees. The paired t test and Wilcoxon signed-rank test were used for statistical comparison.
Results
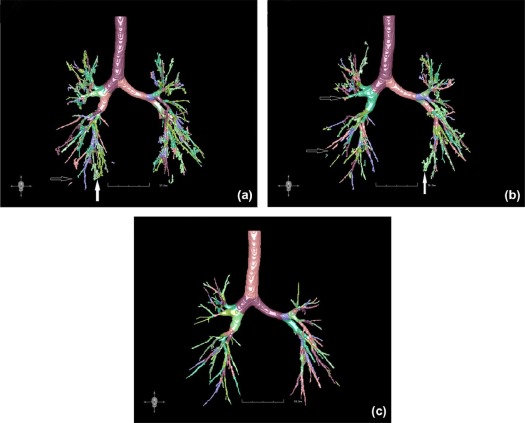
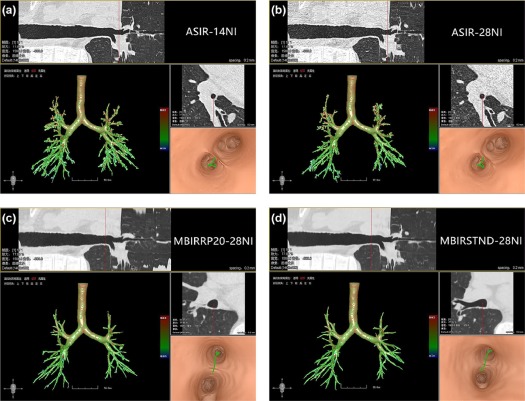
The low-dose CT provided 70.76% dose reduction compared to the routine-dose CT (0.88 ± 0.83 mSv vs 3.01 ± 1.89 mSv). MBIR STND and MBIR RP20 with low-dose CT provided longer bronchial length measurements and were better in measurement variability and continuity and completeness of bronchial walls than ASIR in routine-dose CT ( P < .05). MBIR STND was better for subjective noise and MBIR RP20 for showing distal branches .
Conclusions
MBIR STND and MBIR RP20 algorithms provide better airway quantification at 30% of the radiation dose, compared to ASIR at routine-dose CT.
Introduction
Multidetector computed tomography (MDCT) has been widely used for the diagnosis and identification of lung disease, but the potential risk of radiation-induced carcinogenesis, particularly in younger patients, might limit a wider use of this imaging method in clinical practice. Although the introduction of low-dose chest computed tomography (CT) protocols was found effective in detecting peripheral lung cancers and small lung structure in lung , it may be more difficult in low-dose screening with the increased image noise and thin slice thickness.
The isotropic imaging of MDCT makes it possible for imaging-based computer-aided detection (CAD) to provide a three-dimensional automatic approach to identify the airway tree , and to improve the objectivity and repeatability of imaging diagnosis and therefore increase the diagnostic accuracy for lung diseases. However, the image noise, motion artifacts, and partial volume effects caused by the uneven distribution of gray in the airway will lead to distal local wall fracture and segmentation of the bronchioles , and may diffuse to cause leakage in the lung parenchyma when using CAD .
Get Radiology Tree app to read full this article<
Material and Methods
General Information
Get Radiology Tree app to read full this article<
CT Examinations and Image Reconstruction
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Quantitative CT Airway Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Radiation Dose
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Patient and Lobe Selection
Get Radiology Tree app to read full this article<
Subjective Image Quality Scores
Get Radiology Tree app to read full this article<
TABLE 1
Subjective Image Quality Scores on CAD for Quantitative Analysis of Airway Trees Reconstructed with ASIR, MBIR STND , and MBIR RP20 in Low-dose Chest CT: Comparisonto Adaptive Statistical Iterative Reconstruction in Routine-dose CT
Comparison to ASIR in Routine-dose CT Number of Scores
(−2/−1/0/1/2) ASIR MBIR STND MBIR RP20 MBIR RP20 vs MBIR STND in Low-dose CT Subjective Image Quality of Airway Trees ASIR MBIR STND MBIR RP20 Z Value_P_ Value_Z_ Value_P_ Value Z Value_P_ Value_Z_ Value_P_ Value Subjective noise Reader 1 30/−0/0/0/0 0/0/0/6/24 0/0/3/9/18 −5.477 † .000 −5.108 \* .000 −4.730 \* .000 −2.310 † .021 Reader 2 30/−0/0/0/0 0/0/0/5/25 0/0/2/9/19 −5.477 † .000 −5.152 \* .000 −4.824 \* .014 −2.530 † .011 Continuity and completeness Reader 1 26/4/0/0/0 0/0/2/7/21 0/0/1/6/23 −5.503 † .000 −4.882 \* .000 −5.014 \* .000 −1.000 \* .317 Reader 2 25/5/0/0/0 0/0/1/6/23 0/0/0/6/24 −5.152 † .000 −5.014 \* .000 −5.108 \* .000 −1.414 \* .157 Bronchial end shows Reader 1 30/−0/0/0/0 0/0/4/15/11 0/0/0/10/20 −5.477 † .000 −4.604 \* .000 −4.983 \* .000 −3.153 \* .002 Reader 2 30/−0/0/0/0 0/0/3/16/11 0/0/0/8/22 −5.477 † .000 −4.696 \* .000 −5.035 \* .000 −3.500 \* .000
ASIR, adaptive statistical iterative reconstruction; CAD, computer-aided detection; CT, computed tomography; MBIR RP20 , model-based iterative reconstruction with spatial resolution; MBIR STND , model-based iterative reconstruction with balance spatial resolution and noise reduction.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Objective Measurement
Get Radiology Tree app to read full this article<
TABLE 2
Measured Right Middle Lobe Bronchus Length (mm) of Airway Trees with Images Reconstructed with ASIR, MBIR STND , and MBIR RP20 in Low-dose CT Compared to ASIR in Routine-dose CT (Mean ± Standard Deviation)
Compared to ASIR in Routine-dose ( P Value) ASIR
(NI = 14) ASIR
(NI = 28) MBIR RP20
(NI = 28) MBIR STND
(NI = 28) ASIR (NI = 28) MBIR RP20 (NI = 28) MBIR STND (NI = 28) Bronchus length 21.54 ± 2.97 19.50 ± 2.60 21.54 ± 3.08 21.76 ± 3.12 0.000 0.937 0.038
ASIR, adaptive statistical iterative reconstruction; CT, computed tomography; MBIR, model-based iterative reconstruction; MBIR RP20 , model-based iterative reconstruction with spatial resolution; MBIR STND , model-based iterative reconstruction with balance spatial resolution and noise reduction; NI, noise index.
Get Radiology Tree app to read full this article<
Radiation Doses
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. Manners D., Wong P., Murray C., et. al.: Correlation of ultra-low dose chest CT findings with physiologic measures of asbestosis. Eur Radiol 2017; 27: pp. 1-6.
2. Yu N., Li H., Wu B., et. al.: Computerized identification of bronchiectasis using a 3D quantitative CT protocol. J Med Imaging Health Inform 2016; 6: pp. 1303-1308.
3. Young S., Lo P., Kim G., et. al.: The effect of radiation dose reduction on computer-aided detection (CAD) performance in a low-dose lung cancer screening population. Med Phys 2017; 44: pp. 1337-1346.
4. Korfiatis P., Karahaliou A., Costaridou L.: Automated vessel tree segmentation: challenges in computer aided quantification of diffuse parenchyma lung diseases. IEEE Int Conf Inform Technol Appl Biomed 2009; pp. 1-4.
5. Kalra M.K., Maher M.M., Toth T.L., et. al.: Strategies for CT radiation dose optimization. Radiology 2004; 230: pp. 619-628.
6. Flicek K.T., Hara A.K., Silva A.C., et. al.: Reducing the radiation dose for CT colonography using adaptive statistical iterative reconstruction: a pilot study. AJR Am J Roentgenol 2010; 195: pp. 126-131.
7. Morimoto L.N., Kamaya A., Boulaycoletta I., et. al.: Reduced dose CT with model-based iterative reconstruction compared to standard dose CT of the chest, abdomen, and pelvis in oncology patients: intra-individual comparison study on image quality and lesion conspicuity. Abdom Radiol (NY) 2017; pp. 1-10.
8. Yasaka K., Katsura M., Hanaoka S., et. al.: High-resolution CT with new model-based iterative reconstruction with resolution preference algorithm in evaluations of lung nodules: comparison with conventional model-based iterative reconstruction and adaptive statistical iterative reconstruction. Eur J Radiol 2016; 85: pp. 599-606.
9. Gu S., Fuhrman C., Meng X., et. al.: Computerized identification of airway wall in CT examinations using a 3D active surface evolution approach. Med Image Anal 2013; 17: pp. 283-296.
10. Nan Y., Xiaomin X., Yan L., et. al.: Effect of computed tomography dose on quantitative measurement and automated segmentation of airway tree. J Med Imaging Health Inform 2015; 5: pp. 1-5.
11. National Lung Screening Trial Research Team : Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med 2011; 365: pp. 395-409.
12. Joemai R.M., Geleijns J.: Assessment of structural similarity in CT using filtered backprojection and iterative reconstruction: a phantom study with 3D printed lung vessels. Br J Radiol 2017; 20160519
13. Fleischmann D., Boas F.E.: Computed tomography—old ideas and new technology. Eur Radiol 2011; 21: pp. 510-517.
14. Deák Z., Grimm J.M., Treitl M., et. al.: Filtered back projection, adaptive statistical iterative reconstruction, and a model-based iterative reconstruction in abdominal CT: an experimental clinical study. Radiology 2013; 266: pp. 197-206.
15. Machida H., Takeuchi H., Tanaka I., et. al.: Improved delineation of arteries in the posterior fossa of the brain by model-based iterative reconstruction in volume-rendered 3D CT angiography. AJNR Am J Neuroradiol 2013; 34: pp. 971-975.
16. Hata A., Yanagawa M., Honda O., et. al.: Submillisievert CT using model-based iterative reconstruction with lung-specific setting: an initial phantom study. Eur Radiol 2016; pp. 1-8.
17. Al M.B., Brennan P.C., Mellothoms C.: A review of lung cancer screening and the role of computer-aided detection. Clin Radiol 2017; 1: pp. 1-10.
18. Ma J., Zhou Z., Ren Y., et. al.: Computerized detection of lung nodules through radiomics. Med Phys 2017; 44: pp. 4148-4158.
19. Brillet P.Y., Fetita C.I., Beigelman-Aubry C., et. al.: Quantification of bronchial dimensions at MDCT using dedicated software. Eur Radiol 2007; 17: pp. 1483-1489.
20. Pierre-Yves B., Fetita C.I., Amaury S., et. al.: Investigation of airways using MDCT for visual and quantitative assessment in COPD patients. Int J Chron Obstruct Pulmon Dis 2008; 3: pp. 97-107.
21. Wielpütz M.O., Wroblewski J., Lederlin M., et. al.: Computer-aided detection of artificial pulmonary nodules using an ex vivo lung phantom: influence of exposure parameters and iterative reconstruction. Eur J Radiol 2015; 84: pp. 1005-1011.
22. den Harder A.M., Willemink M.J., Budde R.P., et. al.: Hybrid and model-based iterative reconstruction techniques for pediatric CT. AJR Am J Roentgenol 2015; 204: pp. 645-653.
23. Den Harder A.M., Willemink M.J., van Hamersvelt R.W., et. al.: Effect of radiation dose reduction and iterative reconstruction on computer-aided detection of pulmonary nodules: intra-individual comparison. Eur J Radiol 2016; 85: pp. 346-351.
24. Gomezcardona D., Nagle S.K., Li K., et. al.: Influence of radiation dose and reconstruction algorithm in MDCT assessment of airway wall thickness: a phantom study. Med Phys 2015; 42: pp. 5919-5927.
25. Fontarensky M., Alfidja A., Perignon R., et. al.: Reduced radiation dose with model-based iterative reconstruction versus standard dose with adaptive statistical iterative reconstruction in abdominal CT for diagnosis of acute renal colic. Radiology 2015; 276: pp. 156-166.