
Rationale and Objectives
Academic and clinical interest in reducing radiation from computed tomography (CT) examinations has increased, and the purpose of this study was to determine the capabilities of reduced-dose multidetector-row CT (MDCT) in assessing lung destruction and pulmonary functional loss in pulmonary emphysema patients.
Materials and Methods
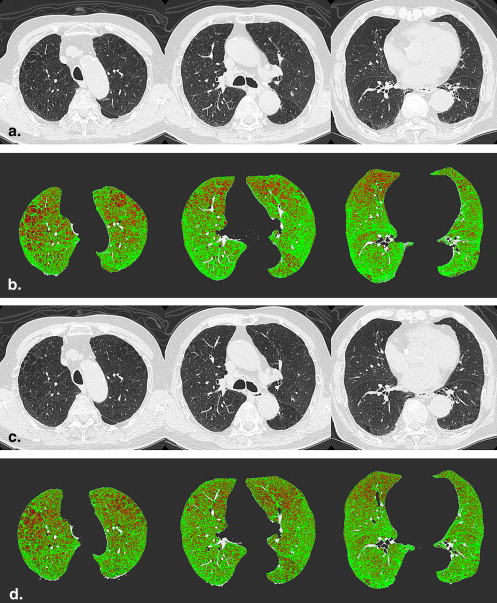
Twenty-five consecutive smokers (15 men and 10 women; mean age 67.9 years; age range 49–86 years) underwent MDCT examinations using two different effective tube currents (standard-dose protocol [150 mAs] and reduced-dose protocol [50 mAs]). For quantitative and qualitative assessments of lung destruction in each subject, percentage of low attenuation emphysematous destruction areas (%LAAs) were computationally calculated, and visual emphysema scores (ESs) were determined for both protocols. To determine the capabilities for quantitative and qualitative assessments of lung destruction by using reduced-dose protocol, %LAAs and ESs of both protocols were compared statistically. To compare the capabilities for quantitative and qualitative assessments of pulmonary functional loss, %LAAs and ESs of both protocols were correlated with forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC).
Results
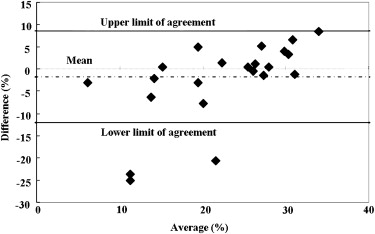
%LAAs and ESs had significant correlations between both protocols (%LAAs: r = 0.95, P < .001; ESs: r = 0.97, P < .001). The limits of agreement of %LAAs were −1.8 ± 9.2%. The agreement of ESs between both protocols was substantial (κ = 0.70). %LAAs and ESs of both protocols had significant correlations with FEV1/FVC (%LAAs of 150 mAs: r = −0.49, P < .05; %LAAs of 50 mAs: r = −0.44, P < .05; ESs of 150 mAs: r = −0.67, P < .001; ESs of 50 mAs: r = −0.66, P < .001).
Conclusion
Reduced-dose MDCT had a potential of substitution for standard-dose MDCT on the both assessments in pulmonary emphysema patients.
With recent advances in multidetector-row computed tomography (MDCT), computed tomography (CT) is now a powerful tool for the assessment of the diagnosis and management of lung diseases. Recently, quantitative and qualitative lung functional assessments with MDCT have become a popular method for assessing the extent and severity of pulmonary emphysema . Before now, assessments using MDCT have mainly been evaluated by low attenuation area (LAA) analysis for quantitative assessments and visual qualitative scores to assess lung destruction in pulmonary emphysema patients. There have been many reports that CT assessment is effective regarding pulmonary functional loss . Results of preliminary studies suggest that CT may have a role in patient selection for lung volume reduction surgery . In addition, it is important to have a sensitive and accurate test for assessing the degree of pulmonary emphysema to promote early detection of disease and monitoring of response to treatment under development of a variety of pharmacologic and endobronchial treatments of patients with smoking-related emphysema .
On the other hand, because the increasing frequency of CT examinations makes radiation dose an important issue, academic and clinical interest in reducing radiation from chest CT examinations has also increased greatly in the last decade . The effect of dose reduction on chest CT examinations has been investigated using subjective assessments of image quality or diagnostic performance . The results have suggested that the tube current–time product could be dramatically reduced for certain applications. These applications include pulmonary angiography, the detection of lung nodules, bronchiectasis, ground-glass opacity, chronic infiltrative lung disease, and pleural and pulmonary asbestos-related abnormalities . Assessments of the repeatability of low-dose quantitative chest CT on the assessment of pulmonary emphysema have suggested the utility of low-dose quantitative chest CT .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Subjects
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Pulmonary Function Tests
Get Radiology Tree app to read full this article<
Scan Protocols
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Analysis
Quantitative assessment of lung destruction and pulmonary functional loss
Get Radiology Tree app to read full this article<
Qualitative assessment of lung destruction and pulmonary functional loss
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
The Agreement on Qualitative Emphysema Scores between both Radiation Dose Protocols
Emphysema score 1 2 3 4 5 κ 150 mAs 161 38 11 7 3 50 mAs 155 46 9 10 0 0.70
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<


Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Mishima M., Oku Y., Kawakami K., et. al.: Quantitative assessment of the spatial distribution of low attenuation areas on X-ray CT using texture analysis in patients with chronic pulmonary emphysema. Front Med Biol Eng 1997; 8: pp. 19-34.
2. Nakano Y., Muller N.L., King G.G., et. al.: Quantitative assessment of airway remodeling using high resolution CT. Chest 2002; 122: pp. 271S-275S.
3. Goldin J.G.: Quantitative CT of emphysema and the airways. J Thorac Imaging 2004; 19: pp. 235-240.
4. Maki D.D., Miller W.T., Aronchick J.M., et. al.: Advanced emphysema: preoperative chest radiographic findings as predictors of outcome following lung volume reduction surgery. Radiology 1999; 212: pp. 49-55.
5. Wan I.Y., Toma T.P., Geddes D.M., et. al.: Bronchoscopic lung volume reduction for end-stage emphysema: report on the first 98 patients. Chest 2006; 129: pp. 518-526.
6. Mayo J.R., Aldrich J., Müller N.L.: Radiation exposure at chest CT: a statement of the Fleischner Society. Radiology 2003; 228: pp. 15-21.
7. Ravenel J.G., Scalzetti E.M., Huda W., et. al.: Radiation exposure and image quality in chest CT examinations. AJR Am J Roentgenol 2001; 177: pp. 279-284.
8. Tack D., De Maertelaer V., Petit W., et. al.: Multi-detector row CT pulmonary angiography: comparison of standard-dose and simulated low-dose techniques. Radiology 2005; 236: pp. 318-325.
9. Ley-Zaporozhan J., Ley S., Krummenauer F., et. al.: Low dose multi-detector CT of the chest (iLEAD Study): visual ranking of different simulated mAs levels. Eur J Radiol 2008 Dec 1; [Epub ahead of print]
10. Madani A., De Maertelaer V., Zanen J., et. al.: Pulmonary emphysema: radiation dose and section thickness at multidetector CT quantification—comparison with macroscopic and microscopic morphometry. Radiology 2007; 243: pp. 250-257.
11. Yuan R., Mayo J.R., Hogg J.C., et. al.: The effects of radiation dose and CT manufacturer on measurements of lung densitometry. Chest 2007; 132: pp. 617-623.
12. Gierada D.S., Pilgram T.K., Whiting B.R., et. al.: Comparison of standard- and low-radiation-dose CT for quantification of emphysema. AJR Am J Roentgenol 2007; 188: pp. 42-47.
13. Trotta B.M., Stolin A.V., Williams M.B., et. al.: Characterization of the relation between CT technical parameters and accuracy of quantification of lung attenuation on quantitative chest CT. AJR Am J Roentgenol 2007; 188: pp. 1683-1690.
14. Zaporozhan J., Ley S., Weinheimer O., et. al.: Multidetector CT of the chest: influence of dose onto quantitative evaluation of severe emphysema: a simulation study. J Comput Assist Tomogr 2006; 30: pp. 460-468.
15. Mayo J.R., Whittall K.P., Leung A.N., et. al.: Simulated dose reduction in conventional chest CT: validation study. Radiology 1997; 202: pp. 453-457.
16. Swensen S.J., Aughenbaugh G.L., Brown L.R.: High-resolution computed tomography of the lung. Mayo Clin Proc 1989; 64: pp. 1284-1294.
17. Matsuoka S., Kurihara Y., Yagihashi K., et. al.: Morphological progression of emphysema on thin-section CT: analysis of longitudinal change in the number and size of low-attenuation clusters. J Comput Assist Tomogr 2006; 30: pp. 669-674.
18. Ohno Y., Hatabu H., Higashino T., et. al.: Oxygen-enhanced MR imaging: correlation with postsurgical lung function in patients with lung cancer. Radiology 2005; 236: pp. 704-711.
19. Ohno Y., Koyama H., Nogami M., et. al.: Dynamic oxygen-enhanced MRI versus quantitative CT: pulmonary functional loss assessment and clinical stage classification of smoking-related COPD. AJR Am J Roentgenol 2008; 190: pp. W93-W99.
20. Ohno Y., Iwasawa T., Seo J.B., et. al.: Oxygen-enhanced magnetic resonance imaging versus computed tomography: multicenter study for clinical stage classification of smoking-related chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2008; 177: pp. 1095-1102.
21. Goddard P.R., Nicholson E.M., Laszlo G., et. al.: Computed tomography in pulmonary emphysema. Clin Radiol 1982; 33: pp. 379-387.
22. Bland J.M., Altman D.G.: Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986; 1: pp. 307-310.
23. Svanholm H., Starklint H., Gundersen H.J., et. al.: Reproducibility of histomorphologic diagnoses with special reference to the kappa statistic. APMIS 1989; 97: pp. 689-698.
24. Gierada D.S.: Radiologic assessment of emphysema for lung volume reduction surgery. Semin Thorac Cardiovasc Surg 2002; 14: pp. 381-390.