
Rationale and Objectives
To determine the potential of multidetector computed tomography (MDCT) in assessing, at 72 hours, the effects of distal coronary microembolization on myocardial structure and function.
Materials and Methods
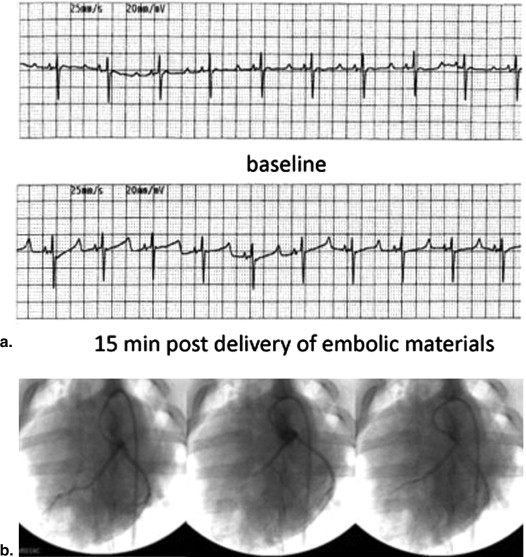
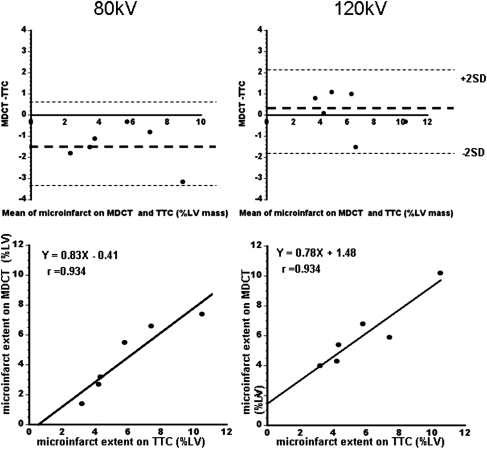
Microembolic material (total volume=16 mm 3 of 40–120 μm diameter) was selectively delivered in the left anterior descending coronary artery under x-ray fluoroscopy ( n = 6 pigs). After 72 hours, 64-slice MDCT was used to assess LV function, perfusion, and viability. For comparison between the measurements at 80 kV, 120 kV, and postmortem we used Bland-Altman and Pearson correlation. Histochemical and histopathological staining was used for quantitative and qualitative characterization of microinfarct.
Results
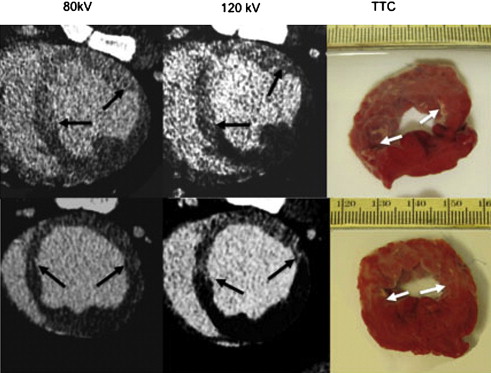
Cine MDCT showed the deleterious effects of microembolization on systolic wall thickening, LV volumes, and ejection fraction. Perfusion parameters, such as max upslope, peak attenuation, and time to peak, differed between microinfarct territory and remote myocardium. Inconsistency in visualizing microinfarct was observed using tube voltages of 80 kV and 120 kV. The extent of heterogeneous microinfarct was 4.5 ± 1.0 % of LV mass at 80 kV, 6.1 ± 0.9% LV at 120 kV, and 5.9 ± 1.1% LV on postmortem. There was significant difference in the extent of microinfarct measured on 80 kV MDCT compared with 120 kV and postmortem. Microscopic examination revealed the random distribution of obstructed microvessels surrounded by myocardial necrosis and inflammatory cells in all animals.
Conclusion
Both visible and nonvisible microinfarct cause perfusion deficit and LV dysfunction. MDCT is sensitive for quantifying early functional changes in LV caused by microembolization. Further improvement in spatial resolution of this technology is needed to improve visualization of microinfarct.
Distal coronary microembolization occurs during percutaneous coronary interventions (PCI) and other diseases, such as atherosclerosis plaque rupture, valvular disease, endocarditis, arrhythmias, heart-lung bypass surgery, and in-patient with congenital heart disease. It is also seen in patients with hypertension, diabetes, systemic lupus erythematosus, and sickle cell disease. Distal coronary microembolization causes microinfarct, arrhythmia, and sudden death .
Microinfarct imaging is a challenge because of the low spatial resolution of conventional diagnostic scanners and motion artifacts. Doppler ultrasound has been used for detection of coronary microembolization during PCI procedures . Porto et al found that the extent of microinfarct is related to the volume of embolic material . Choi et al described the association between microinfarct and impaired myocardial perfusion in 14 patients . Multiple clinical studies highlighted the importance of distal coronary microembolization. In the 2007 guidelines, the American College of Cardiology and European Society of Cardiology confirmed the deleterious effects of distal coronary microembolization.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Experimental Protocol
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Microemboli Volume
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
MDCT Imaging
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Histochemical and Histopathological Studies
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Selective Delivery of Microemboli
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Microinfarct
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Perfusion and Function
Get Radiology Tree app to read full this article<
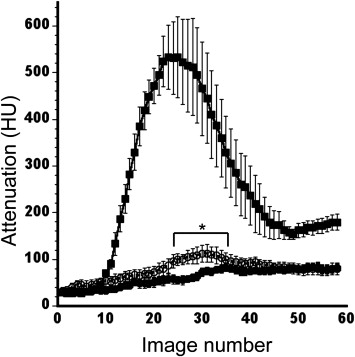
Table 1
Multidetector Computed Tomography Data Obtained 72 Hours after Selective Left Anterior Descending Artery Delivery of 16 mm 3 Volume of 40–120 μm Diameter Embolic Materials
Body weight (kg) 32 ± 1 Heart rate (beats/min) 81 ± 3 Stroke volume (mL) 27.0 ± 1.4 End diastolic volume (mL) 79.1 ± 3.5 End systolic volume (mL) 52.0 ± 4.1 Ejection fraction (%) 34.7 ± 2.5 Left ventricular mass (g) 85.7 ± 1.9
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
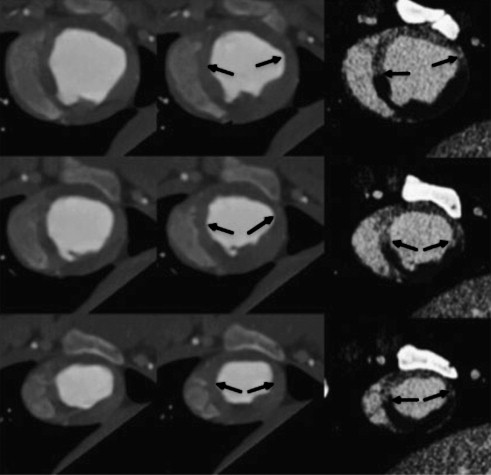

Table 2
First-pass Multidetector Computed Tomography Perfusion Parameters Obtained in Remote Myocardium and Microinfarct Subregion 72 Hours after Delivery of Embolic Materials
Left Ventricular blood Remote Myocardium Microinfarct Max upslope (seconds -1 ) 82 ± 9 16 ± 2 6 ± 2 ∗ Peak attenuation (Hounsfield units) 635 ± 47 123 ± 15 83 ± 7 ∗ Time to the peak (seconds) 11.7 ± 2.1 15.7 ± 1.9 22.3 ± 2.6 ∗
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Histopathology
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Microinfarct
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Function and Perfusion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Technical Considerations
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Practical Applications
Get Radiology Tree app to read full this article<
References
1. Topol E.J., Yadav J.S.: Recognition of the importance of embolization in atherosclerotic vascular disease. Circulation 2000; 101: pp. 570-580.
2. Skyschally A., Leineweber K., Gres P., et. al.: Coronary microembolization. Basic Res Cardiol 2006; 101: pp. 373-382.
3. Schwartz R.S., Burke A., Farb A., et. al.: Microemboli and microvascular obstruction in acute coronary thrombosis and sudden coronary death: relation to epicardial plaque histopathology. J Am Coll Cardiol 2009; 54: pp. 2167-2173.
4. Bahrmann P., Werner G.S., Heusch G., et. al.: Detection of coronary microembolization by Doppler ultrasound in patients with stable angina pectoris undergoing elective percutaneous coronary interventions. Circulation 2007; 115: pp. 600-608.
5. Porto I., Selvanayagam J.B., Van Gaal W.J., et. al.: Plaque volume and occurrence and location of periprocedural myocardial necrosis after percutaneous coronary intervention: insights from delayed-enhancement magnetic resonance imaging, thrombolysis in myocardial infarction myocardial perfusion grade analysis, and intravascular ultrasound. Circulation 2006; 114: pp. 662-669.
6. Choi J.W., Gibson C.M., Murphy S.A., et. al.: Myonecrosis following stent placement: association between impaired TIMI myocardial perfusion grade and MRI visualization of microinfarction. Catheter Cardiovasc Interv 2004; 61: pp. 472-476.
7. Jacquier A., Revel D., Saeed M.: MDCT of the myocardium: a new contribution to ischemic heart disease. Acad Radiol 2008; 15: pp. 477-487.
8. Furtado A.D., Carlsson M., Wintermark M., et. al.: Identification of residual ischemia, infarction, and microvascular impairment in revascularized myocardial infarction using 64-slice MDCT. Contrast Media Mol Imaging 2008; 3: pp. 198-206.
9. Kwong R.Y., Chan A.K., Brown K.A., et. al.: Impact of unrecognized myocardial scar detected by cardiac magnetic resonance imaging on event-free survival in patients presenting with signs or symptoms of coronary artery disease. Circulation 2006; 113: pp. 2733-2743.
10. Gu Y., Bai Y., Wu J., et. al.: Establishment and characterization of an experimental model of coronary thrombotic microembolism in rats. Am J Pathol 2010; 177: pp. 1122-1130.
11. Dorge H., Neumann T., Behrends M., et. al.: Perfusion-contraction mismatch with coronary microvascular obstruction: role of inflammation. Am J Physiol Heart Circ Physiol 2000; 279: pp. H2587-H2592.
12. Di Mario C., Ferrante G.: Embolization: the “dark side” of percutaneous coronary interventions. JACC Cardiovasc Interv 2008; 1: pp. 277-278.
13. Okamura A., Ito H., Iwakura K., et. al.: Clinical implications of distal embolization during coronary interventional procedures in patients with acute myocardial infarction: quantitative study with Doppler guidewire. JACC Cardiovasc Interv 2008; 1: pp. 268-276.
14. Carlsson M., Wilson M., Martin A.J., et. al.: Myocardial microinfarction after coronary microembolization in swine: MR imaging characterization. Radiology 2009; 250: pp. 703-713.
15. Schuleri K.H., Centola M., George R.T., et. al.: Characterization of peri-infarct zone heterogeneity by contrast-enhanced multidetector computed tomography: a comparison with magnetic resonance imaging. J Am Coll Cardiol 2009; 53: pp. 1699-1707.
16. George R.T., Jerosch-Herold M., Silva C., et. al.: Quantification of myocardial perfusion using dynamic 64-detector computed tomography. Invest Radiol 2007; 42: pp. 815-822.
17. Heiberg E., Engblom H., Engvall J., et. al.: Semi-automatic quantification of myocardial infarction from delayed contrast enhanced magnetic resonance imaging. Scand Cardiovasc J 2005; 39: pp. 267-275.
18. Carlsson M., Saloner D., Martin A.J., et. al.: Heterogeneous microinfarcts caused by coronary microemboli: evaluation with multidetector CT and MR imaging in a swine model. Radiology 2010; 254: pp. 718-728.
19. Bland J.M., Altman D.G.: Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986; 1: pp. 307-310.
20. Angelini A., Rubartelli P., Mistrorigo F., et. al.: Distal protection with a filter device during coronary stenting in patients with stable and unstable angina. Circulation 2004; 110: pp. 515-521.
21. Jennings R.B., Steenbergen C., Reimer K.A.: Myocardial ischemia and reperfusion. Monogr Pathol 1995; 37: pp. 47-80.
22. Angeli F.S., Shapiro M., Amabile N., et. al.: Left ventricular remodeling after myocardial infarction: characterization of a swine model on beta-blocker therapy. Comp Med 2009; 59: pp. 272-279.
23. Gu Y., Bai Y., Wu J., et. al.: Establishment and characterization of an experimental model of coronary thrombotic microembolism in rats. Am J Pathol 2010; 177: pp. 1122-1130.
24. Malyar N.M., Gossl M., Beighley P.E., et. al.: Relationship between arterial diameter and perfused tissue volume in myocardial microcirculation: a micro-CT-based analysis. Am J Physiol Heart Circ Physiol 2004; 286: pp. H2386-H2392.
25. Carlsson M., Osman N.F., Ursell P.C., et. al.: Quantitative MR measurements of regional and global left ventricular function and strain after intramyocardial transfer of VM202 into infarcted swine myocardium. Am J Physiol Heart Circ Physiol 2008; 295: pp. H522-H532.
26. Bogaert J., Kalantzi M., Rademakers F.E., et. al.: Determinants and impact of microvascular obstruction in successfully reperfused ST-segment elevation myocardial infarction. Assessment by magnetic resonance imaging. Eur Radiol 2007; 17: pp. 2572-2580.
27. Hardoff R., Shefer A., Gips S., et. al.: Predicting late restenosis after coronary angioplasty by very early (12 to 24 h) thallium-201 scintigraphy: implications with regard to mechanisms of late coronary restenosis. J Am Coll Cardiol 1990; 15: pp. 1486-1492.
28. Jain A., Mahmarian J.J., Borges-Neto S., et. al.: Clinical significance of perfusion defects by thallium-201 single photon emission tomography following oral dipyridamole early after coronary angioplasty. J Am Coll Cardiol 1988; 11: pp. 970-976.
29. Hendel R.C., Patel M.R., Kramer C.M., et. al.: ACCF/ACR/SCCT/SCMR/ASNC/NASCI/SCAI/SIR 2006 appropriateness criteria for cardiac computed tomography and cardiac magnetic resonance imaging: a report of the American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group, American College of Radiology, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, American Society of Nuclear Cardiology, North American Society for Cardiac Imaging, Society for Cardiovascular Angiography and Interventions, and Society of Interventional Radiology. J Am Coll Cardiol 2006; 48: pp. 1475-1497.
30. Einstein A.J.: Radiation protection of patients undergoing cardiac computed tomographic angiography. JAMA 2009; 301: pp. 545-547.
31. Lund G.K., Wegian E., Saeed M., et. al.: 64-Slice spiral computed tomography of the coronary arteries: dose reduction using an optimized imaging protocol including individual weight-adaptation of voltage and current-time product. Eur Radiol 2009; 19: pp. 1132-1138.
32. Mahnken A.H., Jost G., Bruners P., et. al.: Multidetector computed tomography (MDCT) evaluation of myocardial viability: intraindividual comparison of monomeric vs. dimeric contrast media in a rabbit model. Eur Radiol 2009; 19: pp. 290-297.
33. Chen C.I., Iguchi Y., Garami Z., et. al.: Analysis of emboli during carotid stenting with distal protection device. Cerebrovasc Dis 2006; 21: pp. 223-228.
34. Dae M.W., Lee R.J., Ursell P.C., et. al.: Heterogeneous sympathetic innervation in German shepherd dogs with inherited ventricular arrhythmia and sudden cardiac death. Circulation 1997; 96: pp. 1337-1342.