
Rationale and Objectives
Pulmonary vascular alteration is one of the characteristic features of chronic obstructive pulmonary disease (COPD). Recent studies suggest that vascular alteration is closely related to endothelial dysfunction and may be further influenced by emphysema. However, the relationship between morphological alteration of small pulmonary vessels and the extent of emphysema has not been assessed in vivo. The objectives of this study are: to evaluate the correlation of total cross-sectional area (CSA) of small pulmonary vessels with the extent of emphysema and airflow obstruction using CT scans and to assess the difference of total CSA between COPD phenotypes.
Materials and Methods
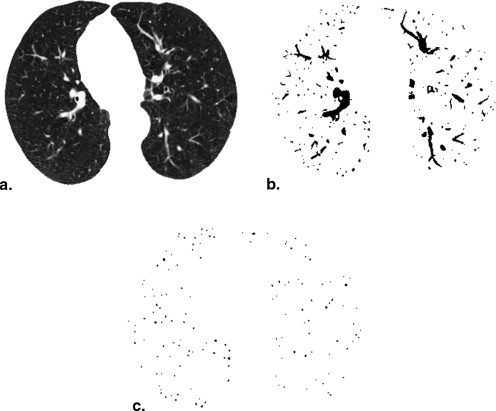
We measured CSA less than 5 mm 2 and 5–10 mm 2 , and calculated the percentage of the total CSA for the lung area (%CSA < 5, and %CSA5–10, respectively) using CT scans in 191 subjects. The extent of emphysema (%LAA-950) was calculated, and the correlations of %CSA < 5 and %CSA5–10 with %LAA-950 and results of pulmonary function tests (PFTs) were evaluated. The differences in %CSA between COPD phenotypes were also assessed.
Results
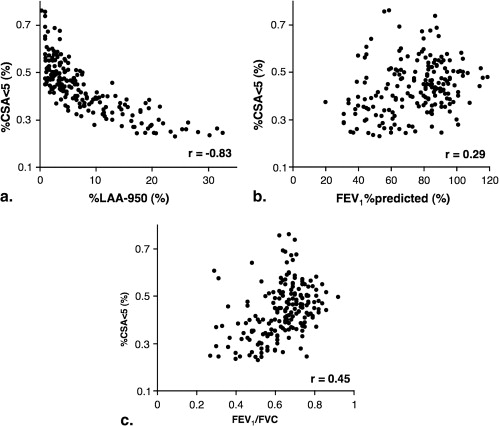
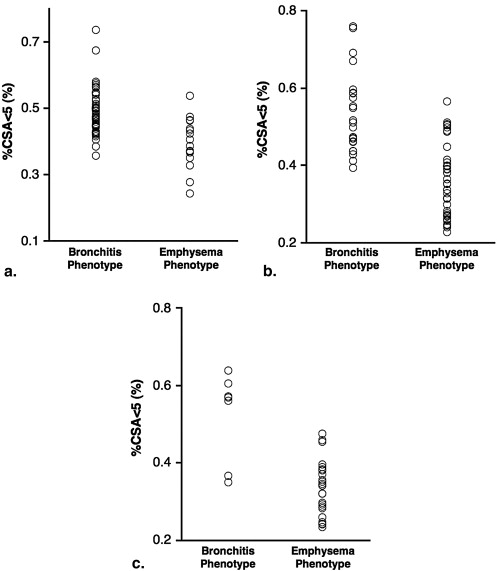
The %CSA < 5 had significant negative correlations with %LAA-950 ( r = -0.83, P < .0001). There was a weak but statistically significant correlation of %CSA < 5 with forced expiratory volume in 1 second (FEV1)% predicted ( r = 0.29, P < .0001) and FEV1/forced vital capacity ( r = 0.45, P < .0001). A %CSA 5–10 had weak correlations with %LAA-950 and results of PFTs. %CSA < 5 was significantly higher in bronchitis phenotype than in the emphysema phenotype ( P < .0001).
Conclusions
Total CSA of small pulmonary vessels at sub-subsegmental levels strongly correlates with the extent of emphysema (%LAA-950) and reflects differences between COPD phenotypes.
Pulmonary vascular alteration is a characteristic feature of chronic obstructive pulmonary disease (COPD). Early angiographic studies in patients with emphysema showed narrowing and reduction in the number of small pulmonary arteries at subsegmental or sub-subsegmental levels . Passive vascular compression by emphysema and hypoxic vasoconstriction has been considered the major pathogenesis of vascular alteration in COPD. Histologically, pulmonary vascular alterations are not exclusive to advanced COPD, however, because they are present in patients with mild COPD and even in smokers with normal pulmonary function . Recent studies suggest that both pulmonary and extrapulmonary vascular alterations in patients with COPD closely relate to endothelial dysfunction . Because of the important role played by the endothelium in regulating vascular tone and controlling cell growth, pulmonary arteries with endothelial dysfunction have a diminished ability to dilate . Consequently, the pulmonary vascular bed decreases, and structural vascular alterations lead to the functional impairments.
Recently, several researchers demonstrated the relationship between endothelial dysfunction and emphysema . Endothelial dysfunction results from changes in the expression and release of vasoactive mediators. In several vasoactive mediators, vascular endothelial growth factor (VEGF) plays an important role in the pathogenesis of both vascular alteration and emphysema . Kasahara et al demonstrated that the blockade of the VEGF receptor caused emphysema, and they simultaneously showed a pruning and decrease of the pulmonary arteries on angiography. More recently, Barr et al suggested that the extent of emphysema, rather than airway obstruction, is responsible for endothelial dysfunction in COPD. Considering these previous reports, we hypothesized that the vascular alteration, as estimated by the reduction in cross-sectional area (CSA) of small pulmonary vessels in patients with COPD, would be related to the extent of emphysema, and predicted a stronger correlation than that with decline of airflow obstruction. To test this hypothesis, we measured CSA of subsegmental and sub-subsegmental pulmonary vessels with CT images, and evaluated the correlation of total CSA with emphysema and airflow obstruction. In addition, previous studies showed the differences in the level of VEGF and vascular alteration between COPD phenotypes . We hypothesized that a difference in vascular alteration between COPD phenotypes existed and sought to measure it.
Methods
Subjects
Get Radiology Tree app to read full this article<
Multislice CT Scanning
Get Radiology Tree app to read full this article<
CT Measurement of Small Pulmonary Vessels
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Pulmonary Function Tests
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Characteristics of the Study Subjects
Get Radiology Tree app to read full this article<
Table 1
Patient Characteristics and Results of Pulmonary Function Tests ( n = 191)
Mean ± SD Age (y) 62 ± 5 Age (y): female 61 ± 4 Age (y): male 63 ± 5 Pack-years 52 ± 29 Current smokers (%) 56.0 FEV 1 (L) 2.3 ± 0.8 FEV 1 % predicted (%) 74.2 ± 20.5 FVC (L) 3.7 ± 0.9 FEV 1 /FVC 0.63 ± 0.13
SD, standard deviation; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity.
Get Radiology Tree app to read full this article<
CSA Measurements and Correlation with %LAA-950 and results of PFTs
Get Radiology Tree app to read full this article<
Table 2
Cross-sectional Area of Pulmonary Vessels and Correlations with %LAA-950 and Pulmonary Function Tests ( n = 191)
Cross-sectional Area Mean ± SD (%) %LAA-950 FEV1% predicted FEV1/FVC_r__P__r__P__r__P_ %CSA < 5 0.43 ± 0.11 -0.83 <.0001 0.29 <.0001 0.45 <.0001 %CSA5–10 0.10 ± 0.04 -0.25 .0004 0.26 .0003 0.22 .0025
%LAA-950, the percentage of low attenuation area less than -950 HU (defined as emphysema); FEV 1 , forced expiratory volume in 1 second; FVC, forced vital capacity; SD, standard deviation; %CSA < 5, percentage total cross-sectional area calculated from pulmonary vessels less than 5 mm 2 ; %CSA5–10, percentage total cross-sectional area calculated from pulmonary vessel size between 5 and 10 mm 2 .
Correlations were assessed using Spearman’s rank correlation analysis.
Get Radiology Tree app to read full this article<
CSA Measurements and COPD Phenotypes
Get Radiology Tree app to read full this article<
Table 3
Cross-sectional Area of COPD Phenotypes ( n = 130)
GOLD Stage %CSA < 5 (%) Bronchitis Phenotype Emphysema Phenotype_P_ Value All Stage 0.53 ± 0.10 0.35 ± 0.08 <0.0001 GOLD 1 0.52 ± 0.08 0.36 ± 0.05 <0.0001 GOLD 2 0.53 ± 0.10 0.36 ± 0.09 <0.0001 GOLD 3 and 4 0.52 ± 0.11 0.33 ± 0.07 <0.0001
GOLD, Global Initiative for Chronic Obstructive Lung Disease; COPD, chronic obstructive pulmonary disease; %CSA < 5, percentage total cross-sectional area calculated from pulmonary vessels less than 5 mm 2 .
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Cordasco E.M., Beerel F.R., Vance J.W., et. al.: Newer aspects of the pulmonary vasculature in chronic lung disease. A comparative study. Angiology 1968; 19: pp. 399-407.
2. Scarrow G.D.: The pulmonary angiogram in chronic bronchitis and emphysema. Proc R Soc Med 1965; 58: pp. 684-687.
3. Jacobson G., Turner A.F., Balchum O.J., et. al.: Vascular changes in pulmonary emphysema. The radiologic evaluation by selective and peripheral pulmonary wedge angiography. Am J Roentgenol Radium Ther Nucl Med 1967; 100: pp. 374-396.
4. Hale K.A., Niewoehner D.E., Cosio M.G.: Morphologic changes in the muscular pulmonary arteries: relationship to cigarette smoking, airway disease, and emphysema. Am Rev Respir Dis 1980; 122: pp. 273-278.
5. Wright J.L., Lawson L., Pare P.D., et. al.: The structure and function of the pulmonary vasculature in mild chronic obstructive pulmonary disease. The effect of oxygen and exercise. Am Rev Respir Dis 1983; 128: pp. 702-707.
6. Magee F., Wright J.L., Wiggs B.R., et. al.: Pulmonary vascular structure and function in chronic obstructive pulmonary disease. Thorax 1988; 43: pp. 183-189.
7. Barbera J.A., Riverola A., Roca J., et. al.: Pulmonary vascular abnormalities and ventilation perfusion relationships in mild chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1994; 149: pp. 423-429.
8. Santos S., Peinado V.I., Ramirez J., et. al.: Characterization of pulmonary vascular remodelling in smokers and patients with mild COPD. Eur Respir J 2002; 19: pp. 632-638.
9. Peinado V.I., Barbera J.A., Abate P., et. al.: Inflammatory reaction in pulmonary muscular arteries of patients with mild chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1999; 159: pp. 1605-1611.
10. Peinado V.I., Barbera J.A., Ramirez J., et. al.: Endothelial dysfunction in pulmonary arteries of patients with mild COPD. Am J Physiol 1998; 274: pp. L908-L913.
11. Kasahara Y., Tuder R.M., Taraseviciene-Stewart L., et. al.: Inhibition of VEGF receptors causes lung cell apoptosis and emphysema. J Clin Invest 2000; 106: pp. 1311-1319.
12. Santos S., Peinado V.I., Ramirez J., et. al.: Enhanced expression of vascular endothelial growth factor in pulmonary arteries of smokers and patients with moderate chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2003; 167: pp. 1250-1256.
13. Barr R.G., Mesia-Vela S., Austin J.H., et. al.: Impaired flow-mediated dilation is associated with low pulmonary function and emphysema in ex-smokers: the Emphysema and Cancer Action Project (EMCAP) Study. Am J Respir Crit Care Med 2007; 176: pp. 1200-1207.
14. Dinh-Xuan A.T., Higenbottam T.W., Clelland C.A., et. al.: Impairment of endothelium-dependent pulmonary-artery relaxation in chronic obstructive lung disease. N Engl J Med 1991; 324: pp. 1539-1547.
15. Kasahara Y., Tuder R.M., Cool C.D., et. al.: Endothelial cell death and decreased expression of vascular endothelial growth factor and vascular endothelial growth factor receptor 2 in emphysema. Am J Respir Crit Care Med 2001; 163: pp. 737-744.
16. Kanazawa H., Asai K., Hirata K., et. al.: Possible effects of vascular endothelial growth factor in the pathogenesis of chronic obstructive pulmonary disease. Am J Med 2003; 114: pp. 354-358.
17. Petrache I., Natarajan V., Zhen L., et. al.: Ceramide upregulation causes pulmonary cell apoptosis and emphysema-like disease in mice. Nat Med 2005; 11: pp. 491-498.
18. McAllister D.A., Maclay J.D., Mills N.L., et. al.: Arterial stiffness is independently associated with emphysema severity in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2007; 176: pp. 1208-1214.
19. Mills N.L., Miller J.J., Anand A., et. al.: Increased arterial stiffness in patients with chronic obstructive pulmonary disease: a mechanism for increased cardiovascular risk. Thorax 2008; 63: pp. 306-311.
20. Taraseviciene-Stewart L., Scerbavicius R., Choe K.H., et. al.: An animal model of autoimmune emphysema. Am J Respir Crit Care Med 2005; 171: pp. 734-742.
21. Tang K., Rossiter H.B., Wagner P.D., et. al.: Lung-targeted VEGF inactivation leads to an emphysema phenotype in mice. J Appl Physiol 2004; 97: pp. 1559-1566.
22. Tuder R.M., Zhen L., Cho C.Y., et. al.: Oxidative stress and apoptosis interact and cause emphysema due to vascular endothelial growth factor receptor blockade. Am J Respir Cell Mol Biol 2003; 29: pp. 88-97.
23. Voelkel N.F., Vandivier R.W., Tuder R.M.: Vascular endothelial growth factor in the lung. Am J Physiol Lung Cell Mol Physiol 2006; 290: pp. L209-L221.
24. Tuder R.M., Yoshida T., Fijalkowka I., et. al.: Role of lung maintenance program in the heterogeneity of lung destruction in emphysema. Proc Am Thorac Soc 2006; 3: pp. 673-679.
25. Kanazawa H., Asai K., Nomura S.: Vascular endothelial growth factor as a non-invasive marker of pulmonary vascular remodeling in patients with bronchitis-type of COPD. Respir Res 2007; 8: pp. 22.
26. Dransfield M.T., Washko G.R., Foreman M.G., et. al.: Gender differences in the severity of CT emphysema in COPD. Chest 2007; 132: pp. 464-470.
27. Miller M.R., Hankinson J., Brusasco V., et. al.: Standardisation of spirometry. Eur Respir J 2005; 26: pp. 319-338.
28. Coche E., Pawlak S., Dechambre S., et. al.: Peripheral pulmonary arteries: identification at multi-slice spiral CT with 3D reconstruction. Eur Radiol 2003; 13: pp. 815-822.
29. Gevenois P.A., de Maertelaer V., De Vuyst P., et. al.: Comparison of computed density and macroscopic morphometry in pulmonary emphysema. Am J Respir Crit Care Med 1995; 152: pp. 653-657.
30. Noma S., Moskowitz G.W., Herman P.G., et. al.: Pulmonary scintigraphy in elastase-induced emphysema in pigs. Correlation with high-resolution computed tomography and histology. Invest Radiol 1992; 27: pp. 429-435.
31. Pistolesi M., Camiciottoli G., Paoletti M., et. al.: Identification of a predominant COPD phenotype in clinical practice. Respir Med 2008; 102: pp. 367-376.
32. Makita H., Nasuhara Y., Nagai K., et. al.: Characterisation of phenotypes based on severity of emphysema in chronic obstructive pulmonary disease. Thorax 2007; 62: pp. 932-937.
33. Musk A.W.: Relation of pulmonary vessel size to transfer factor in subjects with airflow obstruction. AJR Am J Roentgenol 1983; 141: pp. 915-918.
34. Kuriyama K., Gamsu G., Stern R.G., et. al.: CT-determined pulmonary artery diameters in predicting pulmonary hypertension. Invest Radiol 1984; 19: pp. 16-22.
35. Tan R.T., Kuzo R., Goodman L.R., et. al.: Utility of CT scan evaluation for predicting pulmonary hypertension in patients with parenchymal lung disease. Medical College of Wisconsin Lung Transplant Group. Chest 1998; 113: pp. 1250-1256.