
Rationale and Objectives
Malignant pleural mesothelioma (MPM) is a neoplasm that grows circumferentially along the pleura. The tumor and concurrent pleural effusion may reduce lung function by restricting or preventing lung expansion. The purpose of this study was to provide objective evidence that pleurectomy/decortication (P/D) allows trapped lung to reexpand, quantify the reexpansion based on computed tomography (CT) scans, and investigate whether the expansion persists after surgery.
Materials and Methods
A database of 12 patients demonstrating unilateral MPM was collected. Each patient underwent a presurgical CT scan, surgical debulking by P/D, and two postsurgical CT scans (at 1 and 4 months). The lung volume was measured in each scan using an automated algorithm and compared for each patient across time.
Results
An increase in the ipsilateral postsurgical lung volume was observed for 10 of 12 patients (83%) 1 month after surgery. The median ipsilateral volume increase was 44% relative to the presurgical ipsilateral volume and 21% relative to the contralateral volume. A statistically significant change in ipsilateral lung volume was not observed between 1‑month and 4‑month postsurgical scans, implying that the volume improvement persisted months after surgery.
Conclusions
Debulking of MPM with P/D substantially increased the ipsilateral lung volume relative to both the presurgical ipsilateral volume and the contralateral lung volume. This improvement persisted months after surgery.
Malignant pleural mesothelioma (MPM) is a neoplasm of the mesothelial cells principally caused by asbestos exposure. MPM is a primarily unilateral disease that grows nonuniformly along the parietal and visceral pleurae and encases the lung. MPM often presents in computed tomography (CT) scans as pleural thickening growing circumferentially about the lung parenchyma with or without concurrent effusion. Pressure on the lung parenchyma from the tumor and effusion may reduce lung function by restricting or preventing lung expansion (a condition known as trapped/encased lung or restrictive pleurisy) .
Extrapleural pneumonectomy (EPP) and pleurectomy/decortication (P/D) are the principal surgical approaches for MPM. EPP is an aggressive surgical procedure with strict selection criteria that limit its applicability to the general MPM population . The procedure consists of removing the lung, pericardium, diaphragm, and pleura with extrapleural dissection, then reconstructing the pericardium and diaphragm . EPP is associated with increased patient survival, but also high morbidity and mortality rates (although recent studies suggest that these rates are less in centers specially trained for EPP surgical procedures) .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Table 1
Patient Staging, Histology, and Chemotherapeutic Treatment History
Patient Staging Histology Presurgical Treatments Postsurgical Treatments Treatment Initiation (Months after Surgery) 1 T4 Nx Mx Stage IV Epithelioid No AZD2171 3 2 T3 N0 Mx Stage III Mixed No Bevacizumab, pemetrexate, and cisplatin 1 3 T3 Nx Mx Stage III Epithelioid No Pemetrexed and carboplatin 3 4 T2 N0 Mx Stage II Epithelioid No Pemetrexed and carboplatin 1 5 T3 N0 Mx Stage III Epithelioid No Pemetrexed and carboplatin 1 6 T3 N0 Mx Stage III Epithelioid No Pemetrexed and carboplatin 2 7 T3 Nx Mx Stage III Mixed No Pemetrexed and cisplatin 3 8 T3 N0 Mx Stage III Epithelioid No Pemetrexed and carboplatin 1 9 T2 N1 Mx Stage III Mixed No Pemetrexed and carboplatin 3 10 T2 Nx Mx Stage II/III Mixed No Pemetrexed and carboplatin 2 11 T3 N0 Mx Stage III Epithelioid No None N/A 12 T3 Nx Mx Stage III Epithelioid No Pemetrexed and carboplatin 1
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
ΔVabs=(Vtz,ipsVtz,contra)−(Vt1,ipsVt1,contra) Δ
V
abs
=
(
V
t
z
,
ips
V
t
z
,
contra
)
−
(
V
t
1
,
ips
V
t
1
,
contra
)
where V is the lung volume, ips indicates the ipsilateral lung, contra indicates the contralateral lung, t indicates scan time, and ΔV abs is the change in normalized lung volume. A Wilcoxon signed-rank test (5% significance) was applied to determine whether changes in normalized lung volume were statistically significant. The normalized change of the ipsilateral lung volume 1 month after surgery as a proportion of the presurgical ipsilateral lung volume was also calculated:
ΔVre1=(Vtz,ipsVtz,contra)−(Vt1,ipsVt1,contra)Vt1,ipsVt1,contra Δ
V
re
1
=
(
V
t
z
,
ips
V
t
z
,
contra
)
−
(
V
t
1
,
ips
V
t
1
,
contra
)
V
t
1
,
ips
V
t
1
,
contra
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
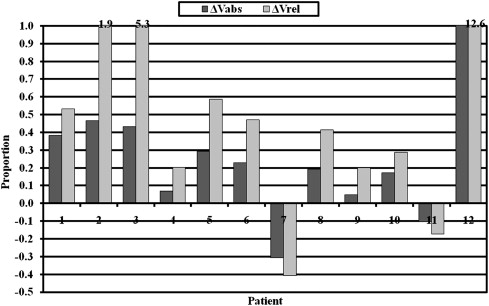
Table 2
Summary of Lung Volume Measurements
Median Range_P_ Value Ratio of presurgical ipsilateral lung volume to contralateral lung volume 0.478 0.081 to 0.754 — Lung expansion at 1 month relative to the presurgical ipsilateral volume (ΔV rel ) 44.3% −40.8% to 1262.7% .007 Lung expansion at 1 month relative to contralateral volume (ΔV abs ) 21.2% −30.8% to 120.7% .027 Lung volume change between 1 month and 4 months after surgery relative to 1‑month volume (ΔV rel ) 7.5% −30.5% to 36.9% .232 Lung volume change between 1 month and 4 months after surgery relative to the contralateral volume (ΔV abs ) 4.4% −33.8% to 18.9% .322
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Kent M., Rice D., Flores R.: Diagnosis, staging, and surgical treatment of malignant pleural mesothelioma. Curr Treat Options Oncol 2008; 9: pp. 158-170.
2. Nakas A., Trousse D.S., Martin-Ucar A.E., et. al.: Open lung-sparing surgery for malignant pleural mesothelioma: the benefits of a radical approach within multimodality therapy. Eur J Cardiothorac Surg 2008; 34: pp. 886-891.
3. van Ruth S., Baas P., Zoetmulder F.A.N.: Surgical treatment of malignant pleural mesothelioma. Chest 2003; 123: pp. 551-561.
4. Flores R.M., Pass H.I., Seshan V.E., et. al.: Extrapleural pneumonectomy versus pleurectomy/decortication in the surgical management of malignant pleural mesothelioma: results in 663 patients. J Thorac Cardiovasc Surg 2008; 135: pp. 620-626.
5. Rusch V.W.: Pleurectomy/decortication in the setting of multimodality treatment for diffuse malignant pleural mesothelioma. Semin Thorac Cardiovasc Surg 1997; 9: pp. 367-372.
6. Hilaris B.S., Nori D., Kwong E., et. al.: Pleurectomy and intraoperative brachytherapy and postoperative radiation in the treatment of malignant pleural mesothelioma. Int J Radiat Oncol Biol Phys 1984; 10: pp. 325-331.
7. Soysal O., Karaoglanoglu N., Demiracan S., et. al.: Pleurectomy/decortication for palliation in malignant pleural mesothelioma: results of surgery. Eur J Cardiothorac Surg 1997; 11: pp. 210-213.
8. Rzyman W., Skokowski J., Romanowicz G., et. al.: Decortication in chronic pleural empyema—effect on lung function. Eur J Cardiothorac Surg 2002; 21: pp. 502-507.
9. Chun E.M., Suh S.W., Modi H.N., et. al.: The change in ratio of convex and concave lung volume in adolescent idiopathic scoliosis: a 3D CT scan based cross sectional study of effect of severity of curve on convex and concave lung volumes in 99 cases. Eur Spine J 2008; 17: pp. 224-229.