
Rationale and Objectives
Despite ongoing technical refinements, coronary computed tomography angiography (cCTA) remains challenging in its diagnostic value by electrocardiographic (ECG) misregistration and motion artifacts, which commonly occur in patients with atrial fibrillation and high or irregular heart rates. The aim of this study was to evaluate the radiation dose and the number of inconclusive coronary segments at cCTA using retrospective ECG gating at 100 and 70 kV.
Materials and Methods
With institutional review board approval, 154 patients (median age 54 years, 98 men) with high or irregular heart rate prospectively underwent retrospectively ECG-gated cCTA without tube current modulation on a third-generation dual-source computed tomography (DSCT) system at 70 kV ( n = 103) or on a second-generation DSCT system at 100 kV ( n = 51). Images were reconstructed in best diastolic phase (BDP), best systolic phase (BSP), and in all phases (APs) at 10% intervals across the R-R cycle. Objective and subjective image qualities were evaluated as well as the presence of motion artifacts with the three different reconstruction approaches.
Results
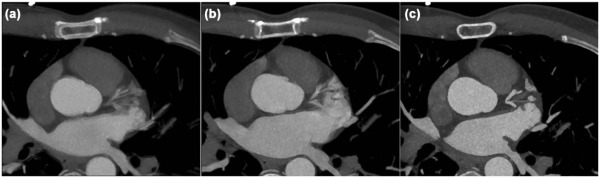
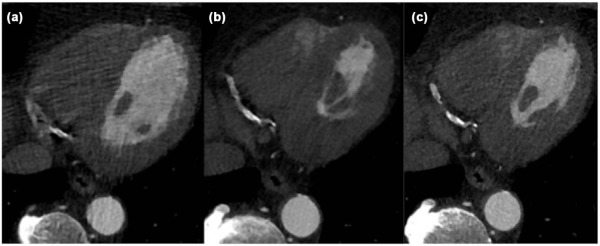
The mean heart rate was 93 ± 16 bpm. The mean effective radiation dose was 4.5 mSv for 70 kV compared to 8.4 mSv for 100 kV ( P < 0.05). At BDP reconstruction, 71% ( n = 110) of the patients showed motion artifacts in one or more coronary segments. At BSP reconstruction, the number of patients with motion artifacts decreased to 37% ( n = 57). In contrast, if images were reconstructed with the AP approach, all vessels and coronary segments were evaluable with both cCTA protocols.
Conclusions
Retrospectively ECG-gated cCTA at 70 kV results in 52% decreased radiation dose. Further using the AP algorithm allowed for diagnostic evaluation of all coronary segments for stenosis, in contrast to BDP or BSP phase alone.
Introduction
Despite ongoing technical refinements, coronary computed tomography angiography (cCTA) remains limited in its diagnostic value by electrocardiographic (ECG) misregistration and motion artifacts, which most commonly occur in patients with atrial fibrillation and high and irregular heart rates. Accordingly, a substantial share of currently available studies investigating the diagnostic accuracy of this test exclude nonevaluable coronary segments from their data analysis . Thus, in real life , diagnostic accuracy of cCTA may be significantly lower compared to the results of clinical trials. From a statistical viewpoint, when gauging cCTA’s true diagnostic performance, it may be more appropriate to apply 3 × 2 tables that include nonevaluable coronary segments as a separate cell compared to including them in the “false negative” or the “false positive” cell of a 2 × 2 table, as is common in clinical trials .
Generally, greater robustness of this test is desirable, especially when atherosclerosis is present, to minimize downstream investigations due to inconclusive cCTA studies. Retrospectively ECG-gated cCTA without ECG-controlled tube current modulation is the most robust cCTA imaging technique . This technique allows reconstruction of images at any desired phase of the heart cycle and the removal of image data acquired during irregular heartbeats, which can lead to ECG misregistration and motion artifacts. Moreover, this technique allows accurate assessment of cardiac function facilitating prediction of mortality as recently shown by an analysis from the multinational CONFIRM registry .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Patients
Get Radiology Tree app to read full this article<
CT Technique
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Assessment of Image Quality and Image Evaluation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Assessment of Radiation Dose
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Patients’ Characteristics and Heart Rate During Scanning
Get Radiology Tree app to read full this article<
TABLE 1
Demographic Patient Data and Radiation Dose Parameters
70-kV cCTA 100-kV cCTA_P_ Value_n_ 103 51 <0.0001 Age (range) 53(24–87) 57(26–89) >0.6325 Male gender 64%(65) 61%(31) >0.8831 Heart rate (bpm) 95 ± 16 91 ± 15 >0.5752 Arrhythmia 67%(69) 71%(36) >0.6953 Body mass index (kg/m 2 ) 27 ± 6 26 ± 5 >0.9649 Median Agatston score 117(0–1653) 130(0–1432) >0.2136 LV ejection fraction 58 ± 21 62 ± 25 >0.3196 Stroke volume (mL) 55 ± 26 59 ± 23 >0.3651 ED volume (mL) 145 ± 67 151 ± 56 >0.4274 ES volume (mL) 43 ± 15 48 ± 13 >0.2867 Coronary artery stenosis (>50%) 25%(26) 26%(13) >0.8993 CTDI vol (mGy) 18 ± 4 33 ± 5 <0.0001 Dose length product (mGy⋅cm) 324 ± 114 601 ± 117 <0.0001 Effective dose (mSv) 4.5 ± 1.6 8.4 ± 1.6
bpm, beat per minute; cCTA, coronary computed tomography angiography; CTDI vol , volume CT dose index; ED, end diastolic; ES, end systolic; LV, left ventricle.
Values in parentheses represent data range.
Get Radiology Tree app to read full this article<
Radiation Dose
Get Radiology Tree app to read full this article<
Subjective and Objective Image Qualities
Get Radiology Tree app to read full this article<
TABLE 2
Subjective and Objective Image Qualities of 70- and 100-kV Retrospectively ECG-Gated cCTA
70-kV cCTA 100-kV cCTA_P_ value Objective image quality Attenuation (mean HU) Aortic root 623 ± 124 471 ± 117 <0.0001 Left ventricle 605 ± 122 474 ± 118 <0.0001 Epicardial muscle 102 ± 12 100 ± 12 <0.0001 Contrast-to-noise ratio (mean) Aortic root 13 ± 4 9 ± 3 <0.0001 Left ventricle 13 ± 4 10 ± 3 <0.0001 Subjective image quality (median) Overall image quality 5 (5–5) 5 (5–5) >0.3358 Overall image noise 5 (4–5) 5 (4–5) >0.3118 Overall vessel attenuation 5 (5–5) 5 (5–5) >0.2574
cCTA, coronary computed tomography angiography.
TABLE 3
Diagnostic Findings of a 3 × 2 Table Including Nonevaluable Results
cCTA Protocol (kV) Dataset True Positive True Negative False Positive False Negative Nonevaluable (Positive) Nonevaluable (Negative) 70 BSP 27 37 39 0 11 39 100 13 18 20 0 7 20 70 BDP 27 20 56 0 15 56 100 13 8 30 0 9 30
BDP, best diastolic phase; BSP, best systolic phase; cCTA, coronary computed tomography angiography.
Nonevaluable segments were rated as positive.
Get Radiology Tree app to read full this article<
Motion Artifacts
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Accuracy of Visibility
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 4
Accuracy of Visibility of the BSPs and BDPs, with the Reconstruction of All Phases as the Reference on a Per-Patient Level (Positive Finding >70% Stenosis)
cCTA Protocol (kV) Dataset Sensitivity (%) CI (%) Specificity (%) CI (%) PPV (%) CI (%) NPV (%) CI (%) 70 BDP 100 87–100 27 17–38 33 23–44 100 83–100 100 100 75–100 21 10–38 30 17–46 100 63–100 70 BSP 100 87–100 49 37–60 41 29–54 100 90–100 100 100 75–100 47 31–64 39 23–57 100 81–100
BDP, best diastolic phase; BSP, best systolic phase; cCTA, coronary computed tomography angiography; CI, confidence intervals; NPV, negative predictive value; PPV, positive predictive value.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgment
Get Radiology Tree app to read full this article<
References
1. Schuetz G.M., Schlattmann P., Dewey M.: Use of 3x2 tables with an intention to diagnose approach to assess clinical performance of diagnostic tests: meta-analytical evaluation of coronary CT angiography studies. BMJ 2012; 345: pp. e6717.
2. Jakobs T.F., Becker C.R., Ohnesorge B., et. al.: Multislice helical CT of the heart with retrospective ECG gating: reduction of radiation exposure by ECG-controlled tube current modulation. Eur Radiol 2002; 12: pp. 1081-1086.
3. Ohnesorge B., Flohr T., Becker C., et. al.: Cardiac imaging by means of electrocardiographically gated multisection spiral CT: initial experience. Radiology 2000; 217: pp. 564-571.
4. Arsanjani R., Berman D.S., Gransar H., et. al.: Left ventricular function and volume with coronary CT angiography improves risk stratification and identification of patients at risk for incident mortality: results from 7758 patients in the prospective multinational CONFIRM observational cohort study. Radiology 2014; 273: pp. 70-77.
5. Hausleiter J., Meyer T., Hermann F., et. al.: Estimated radiation dose associated with cardiac CT angiography. JAMA 2009; 301: pp. 500-507.
6. Meyer M., Haubenreisser H., Schoepf U.J., et. al.: Closing in on the K edge: coronary CT angiography at 100, 80, and 70 kV-initial comparison of a second- versus a third-generation dual-source CT system. Radiology 2014; 273: pp. 373-382.
7. Gruettner J., Henzler T., Sueselbeck T., et. al.: Clinical assessment of chest pain and guidelines for imaging. Eur J Radiol 2012; 81: pp. 3663-3668.
8. Agatston A.S., Janowitz W.R., Hildner F.J., et. al.: Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol 1990; 15: pp. 827-832.
9. Ruzsics B., Gebregziabher M., Lee H., et. al.: Coronary CT angiography: automatic cardiac-phase selection for image reconstruction. Eur Radiol 2009; 19: pp. 1906-1913.
10. Scanlon P.J., Faxon D.P., Audet A.M., et. al.: ACC/AHA guidelines for coronary angiography. A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines (Committee on Coronary Angiography). Developed in collaboration with the Society for Cardiac Angiography and Interventions. J Am Coll Cardiol 1999; 33: pp. 1756-1824.
11. Achenbach S., Goroll T., Seltmann M., et. al.: Detection of coronary artery stenoses by low-dose, prospectively ECG-triggered, high-pitch spiral coronary CT angiography. JACC Cardiovasc Imaging 2011; 4: pp. 328-337.
12. The 2007 Recommendations of the International Commission on Radiological Protection. ICRP publication 103. Ann ICRP 2007; 37: pp. 1-332.
13. Vorre M.M., Abdulla J.: Diagnostic accuracy and radiation dose of CT coronary angiography in atrial fibrillation: systematic review and meta-analysis. Radiology 2013; 267: pp. 376-386.
14. Di Cesare E., Gennarelli A., Di Sibio A., et. al.: Image quality and radiation dose of single heartbeat 640-slice coronary CT angiography: a comparison between patients with chronic atrial fibrillation and subjects in normal sinus rhythm by propensity analysis. Eur J Radiol 2015; 84: pp. 631-636.
15. Kondo T., Matsutani H., Groarke J., et. al.: Technical note: electrocardiogram electrode repositioning for 320-row coronary CT angiography in patients with regular and recurrent premature ventricular contractions. J Cardiovasc Comput Tomogr 2014; 8: pp. 13-18.
16. Wang Q., Qin J., He B., et. al.: Computed tomography coronary angiography with a consistent dose below 2 mSv using double prospectively ECG-triggered high-pitch spiral acquisition in patients with atrial fibrillation: initial experience. Int J Cardiovasc Imaging 2013; 29: pp. 1341-1349.
17. Huda W., Scalzetti E.M., Levin G.: Technique factors and image quality as functions of patient weight at abdominal CT. Radiology 2000; 217: pp. 430-435.
18. Takx R.A., Moscariello A., Schoepf U.J., et. al.: Quantification of left and right ventricular function and myocardial mass: comparison of low-radiation dose 2nd generation dual-source CT and cardiac MRI. Eur J Radiol 2012; 81: pp. e598-e604.