
Rationale and Objectives
We compared the radiation dose and diagnostic accuracy on 120- and 100-kVp coronary computed tomography angiography (CCTA) scans whose contrast-to-noise ratio (CNR) was the same.
Materials and Methods
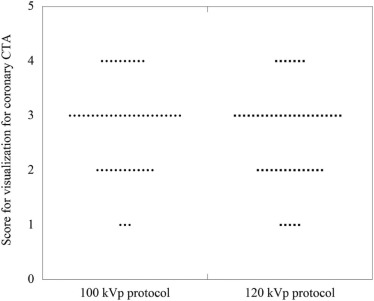
We studied 1311 coronary artery segments from 100 patients. For 120-kVp scans, the targeted image level was set at 25 Hounsfield units (HU). For 100-kVp scans, the targeted noise level was set at 30 HU to obtain the same CNR as at 120 kVp. We compared the CNR and the radiation dose on scans acquired at 120 and 100 kVp. Invasive coronary angiography (ICA) images were evaluated by an interventional coronary angiography specialist, and CCTA images were evaluated by a radiologist. Coronary artery disease was defined as a luminal narrowing ≧50% for ICA and CCTA. With ICA considered the gold standard, the diagnostic accuracy (sensitivity, specificity, positive predictive value, and negative predictive value) was analyzed on both 120- and 100-kVp CCTA images. We also compared the diagnostic accuracy for area under the receiver operating characteristic curve of the ICA and CCTA performed at 120 and 100 kVp. Two blinded observers visually evaluated the septal branch.
Results
The mean dose-length product was 48% lower at 100 kVp than at 120 kVp ( P < .01). Under the 120-kVp CCTA protocol, the area under the curve, 95% confidence interval, sensitivity, specificity, positive predictive value, and negative predictive value were 0.94%, 0.91%–0.96%, 94.0%, 93.0%, 82.3%, and 98.1%, respectively; at 100 kVp these values were 0.94%, 0.92%–0.97%, 96.1%, 92.0%, 85.2%, and 98.0%, respectively. Area under the receiver operating characteristic curve analysis revealed no significant difference in diagnostic accuracy between the two protocols ( P = .87).
Conclusions
At the same CNR, the 100-kVp CCTA protocol may help to reduce the radiation dose by approximately 50% compared to the 120-kVp protocol without degradation of diagnostic accuracy.
Introduction
Coronary computed tomography angiography (CCTA) is an alternative to invasive coronary angiography (ICA) , although its delivery of a higher radiation dose is of concern . To reduce the radiation dose, prospective electrocardiogram triggering with block-wise , high-pitch spiral scanning , automatic tube current modulation , a combination of automatic tube current modulation and automatic tube voltage selection , and lower tube voltage techniques have been introduced.
Application of the contrast-to-noise ratio (CNR) index of the image noise to low tube voltage scans reduced the radiation dose delivered at computed tomography angiography . However, the diagnostic accuracy of CCTA scans obtained at 100 and 120 kVp with the same CNR remained to be compared.
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
Patients
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 1
Patient Characteristics
100-kVp Protocol 120-kVp Protocol_P_ Value Number of patients 50 50 Segment number of coronary 639 672 Sex (male/female) 35/15 34/16 .50 Age (y) 73.0 (43–93) 73.0 (41–91) .90 Height (cm) 161.3 (134–180) 160.1 (138–175) .51 Weight (kg) 59.0 (47–75) 60.0 (43–82) .49 BMI (kg/m 2 ) 23.2 (19.3–31.6) 24.1 (17.4–33.3) .13 Heart rate (bpm) 58.0 (51–70) 59.0 (53–74) .41
BMI, body mass index.
Get Radiology Tree app to read full this article<
Computed Tomography (CT)
Get Radiology Tree app to read full this article<
Image Quality Setting
Get Radiology Tree app to read full this article<
CT number of SD∝1/mAs1/2 CT number of SD
∝
1
/
mAs
1
/
2
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
tube current=250×(BMI/25)and tube current
=
250
×
(
BMI
/
25
)
and
mA=10×BW(kg)/[body height(m)]2 mA
=
10
×
BW
(
kg
)
/
[
body height
(
m
)
]
2
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Contrast Injection Protocols
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Radiation Dose and Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
ICA
Get Radiology Tree app to read full this article<
CCTA Data Analysis
Comparison of the Diagnostic Accuracy of ICA and CCTA
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Comparison of the Visible Smallest Vessel Between 120- and 100-kVp Images
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
TABLE 2
Radiation Dose and Quantitative Image Analysis
Parameter 100-kVp Protocol 120-kVp Protocol_P_ Value CT number (ascending aorta in HU) 542.4 ± 75.3 445.1 ± 60.1 <.01 CT number (muscle in HU) 53.9 ± 7.6 42.1 ± 7.1 <.01 Mean image noise (muscle in HU) 30.1 ± 1.6 26.1 ± 0.9 <.01 Contrast to noise ratio 16.3 ± 2.8 15.4 ± 2.3 .11 Dose length product (mGy-cm) 603.4 ± 120.9 897.0 ± 212.7 <.01
CT, computed tomography; HU, Hounsfield units.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
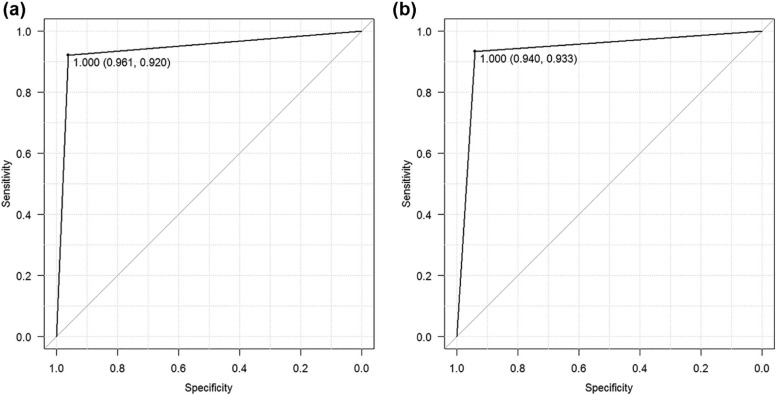
TABLE 3
Diagnostic Accuracy
100-kVp Protocol 120-kVp Protocol Mean 95% CI Mean 95% CI Sensitivity 92.0 86–96 93.7 89–97 Specificity 96.1 94–98 94.1 92–96 Negative predictive value 98.0 96–99 98.1 97–99 Positive predictive value 85.2 78–91 82.3 76–88
CI, confidence interval.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Douglas P.S., Pontone G., Hlatky M.A., et. al.: Clinical outcomes of fractional flow reserve by computed tomographic angiography-guided diagnostic strategies vs. usual care in patients with suspected coronary artery disease: the prospective longitudinal trial of FFR (CT): outcome and resource impacts study. Eur Heart J 2015; 36: pp. 3359-3367.
2. Hausleiter J., Meyer T., Hermann F., et. al.: Estimated radiation dose associated with cardiac CT angiography. JAMA 2009; 301: pp. 500-507.
3. Husmann L., Valenta I., Gaemperli O., et. al.: Feasibility of low-dose coronary CT angiography: first experience with prospective ECG-gating. Eur Heart J 2008; 29: pp. 191-197.
4. Herzog B.A., Husmann L., Burkhard N., et. al.: Accuracy of low-dose computed tomography coronary angiography using prospective electrocardiogram-triggering: first clinical experience. Eur Heart J 2008; 29: pp. 3037-3042.
5. Herzog B.A., Wyss C.A., Husmann L., et. al.: First head-to-head comparison of effective radiation dose from low-dose 64-slice CT with prospective ECG-triggering versus invasive coronary angiography. Heart 2009; 95: pp. 1656-1661.
6. Buechel R.R., Husmann L., Herzog B.A., et. al.: Low-dose computed tomography coronary angiography with prospective electrocardiogram triggering: feasibility in a large population. J Am Coll Cardiol 2011; 57: pp. 332-336.
7. Achenbach S., Marwan M., Ropers D., et. al.: Coronary computed tomography angiography with a consistent dose below 1 mSv using prospectively electrocardiogram-triggered high-pitch spiral acquisition. Eur Heart J 2010; 31: pp. 340-346.
8. He G., Liu X., Liu Y., et. al.: Dose study of electrocardiogram automatic tube current modulation technology in prospective coronary computed tomography angiography scans of overweight patients. Exp Ther Med 2015; 9: pp. 2384-2388.
9. Lee K.H., Lee J.M., Moon S.K., et. al.: Attenuation-based automatic tube voltage selection and tube current modulation for dose reduction at contrast-enhanced liver CT. Radiology 2012; 265: pp. 437-447.
10. Mayer C., Meyer M., Fink C., et. al.: Potential for radiation dose savings in abdominal and chest CT using automatic tube voltage selection in combination with automatic tube current modulation. AJR Am J Roentgenol 2014; 203: pp. 292-299.
11. Schueller-Weidekamm C., Schaefer-Prokop C.M., Weber M., et. al.: CT angiography of pulmonary arteries to detect pulmonary embolism: improvement of vascular enhancement with low kilovoltage settings. Radiology 2006; 241: pp. 899-907.
12. Hausleiter J., Martinoff S., Hadamitzky M., et. al.: Image quality and radiation exposure with a low tube voltage protocol for coronary CT angiography: results of the PROTECTION II Trial. JACC Cardiovasc Imaging 2010; 3: pp. 1113-1123.
13. Masuda T., Funama Y., Kiguchi M., et. al.: Radiation dose reduction based on CNR index with low-tube voltage scan for pediatric CT scan: experimental study using anthropomorphic phantoms. Springerplus 2016; 5: pp. 2064.
14. Imai E., Horio M., Nitta K., et. al.: Modification of the Modification of Diet in Renal Disease (MDRD) Study equation for Japan. Am J Kidney Dis 2007; 50: pp. 927-937.
15. Matsuo S., Imai E., Horio M., et. al.: Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis 2009; 53: pp. 982-992.
16. Hendel R.C., Patel M.R., Kramer C.M., et. al.: ACCF/ACR/SCCT/SCMR/ASNC/NASCI/SCAI/SIR 2006 appropriateness criteria for cardiac computed tomography and cardiac magnetic resonance imaging: a report of the American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group, American College of Radiology, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, American Society of Nuclear Cardiology, North American Society for Cardiac Imaging, Society for Cardiovascular Angiography and Interventions, and Society of Interventional Radiology. J Am Coll Cardiol 2006; 48: pp. 1475-1497.
17. Masuda T., Funama Y., Nakaura T., et. al.: CT angiography of suspected peripheral artery disease: comparison of contrast enhancement in the lower extremities of patients undergoing and those not undergoing hemodialysis. AJR Am J Roentgenol 2017; 208: pp. 1127-1133.
18. Mahnken A.H., Wildberger J.E., Simon J., et. al.: Detection of coronary calcifications: feasibility of dose reduction with a body weight-adapted examination protocol. AJR Am J Roentgenol 2003; 181: pp. 533-538.
19. Jung B., Mahnken A.H., Stargardt A., et. al.: Individually weight-adapted examination protocol in retrospectively ECG-gated MSCT of the heart. Eur Radiol 2003; 13: pp. 2560-2566.
20. Horiguchi J., Yamamoto H., Hirai N., et. al.: Variability of repeated coronary artery calcium measurements on low-dose ECG-gated 16-MDCT. AJR Am J Roentgenol 2006; 187: pp. W1-W6.
21. Sevrukov A., Pratap A., Doss C., et. al.: Electron beam tomography imaging of coronary calcium: the effect of body mass index on radiologic noise. J Comput Assist Tomogr 2002; 26: pp. 592-597.
22. Horiguchi J., Matsuura N., Yamamoto H., et. al.: Coronary artery calcium scoring on low-dose prospective electrocardiographically-triggered 64-slice CT. Acad Radiol 2009; 16: pp. 187-193.
23. Horiguchi J., Matsuura N., Yamamoto H., et. al.: Evaluation of attenuation-based tube current control in coronary artery calcium scoring on prospective ECG-triggered 64-detector CT. Acad Radiol 2009; 16: pp. 1231-1240.
24. Austen W.G., Edwards J.E., Frye R.L., et. al.: A reporting system on patients evaluated for coronary artery disease. Report of the Ad Hoc Committee for Grading of Coronary Artery Disease, Council on Cardiovascular Surgery, American Heart Association. Circulation 1975; 51: pp. 5-40.
25. Budoff M.J., Dowe D., Jollis J.G., et. al.: Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial. J Am Coll Cardiol 2008; 52: pp. 1724-1732.
26. Gaemperli O., Schepis T., Valenta I., et. al.: Functionally relevant coronary artery disease: comparison of 64-section CT angiography with myocardial perfusion SPECT. Radiology 2008; 248: pp. 414-423.
27. Abbara S., Blanke P., Maroules C.D., et. al.: SCCT guidelines for the performance and acquisition of coronary computed tomographic angiography: a report of the society of Cardiovascular Computed Tomography Guidelines Committee endorsed by the North American Society for Cardiovascular Imaging (NASCI). J Cardiovasc Comput Tomogr 2016; 10: pp. 435-449.
28. Huda W., Scalzetti E.M., Levin G.: Technique factors and image quality as functions of patient weight at abdominal CT. Radiology 2000; 217: pp. 430-435.
29. Sigal-Cinqualbre A.B., Hennequin R., Abada H.T., et. al.: Low-kilovoltage multi-detector row chest CT in adults: feasibility and effect on image quality and iodine dose. Radiology 2004; 231: pp. 169-174.
30. Krissak R., Henzler T., Prechel A., et. al.: Triple-rule-out dual-source CT angiography of patients with acute chest pain: dose reduction potential of 100 kV scanning. Eur J Radiol 2012; 81: pp. 3691-3696.
31. Waaijer A., Prokop M., Velthuis B.K., et. al.: Circle of Willis at CT angiography: dose reduction and image quality—reducing tube voltage and increasing tube current settings. Radiology 2007; 242: pp. 832-839.
32. Sahani D.V., Kalva S.P., Hahn P.F., et. al.: 16-MDCT angiography in living kidney donors at various tube potentials: impact on image quality and radiation dose. AJR Am J Roentgenol 2007; 188: pp. 115-120.
33. Nakayama Y., Awai K., Funama Y., et. al.: Abdominal CT with low tube voltage: preliminary observations about radiation dose, contrast enhancement, image quality, and noise. Radiology 2005; 237: pp. 945-951.
34. Schindera S.T., Nelson R.C., Mukundan S., et. al.: Hypervascular liver tumors: low tube voltage, high tube current multi-detector row CT for enhanced detection—phantom study. Radiology 2008; 246: pp. 125-132.
35. Fei X., Du X., Yang Q., et. al.: 64-MDCT coronary angiography: phantom study of effects of vascular attenuation on detection of coronary stenosis. AJR Am J Roentgenol 2008; 191: pp. 43-49.
36. Layritz C., Muschiol G., Flohr T., et. al.: Automated attenuation-based selection of tube voltage and tube current for coronary CT angiography: Reduction of radiation exposure versus a BMI-based strategy with an expert investigator. J Cardiovasc Comput Tomogr 2013; 7: pp. 303-310.
37. Park E.A., Lee W., Kang J.H., et. al.: The image quality and radiation dose of 100-kVp versus 120-kVp ECG-gated 16-slice CT coronary angiography. Korean J Radiol 2009; 10: pp. 235-243.
38. Takx R.A.P., Krissak R., Fink C., et. al.: Low-tube-voltage selection for triple-rule-out CTA: relation to patient size. Eur Radiol 2017; 27: pp. 2292-2297.
39. Health Quality Ontario : Non-invasive cardiac imaging technologies for the diagnosis of coronary artery disease: a summary of evidence-based analyses. Ont Health Technol Assess Ser 2010; 10: pp. 1-40.
40. Guimaraes L.S., Fletcher J.G., Harmsen W.S., et. al.: Appropriate patient selection at abdominal dual-energy CT using 80 kV: relationship between patient size, image noise, and image quality. Radiology 2010; 257: pp. 732-742.
41. Yu L., Li H., Fletcher J.G., et. al.: Automatic selection of tube potential for radiation dose reduction in CT: a general strategy. Med Phys 2010; 37: pp. 234-243.