
Rationale and Objectives
This work aimed to study the effects of scanner model and study protocol on radiation dose received by breast tissues from 64-slice computed tomography (CT) studies.
Materials and Methods
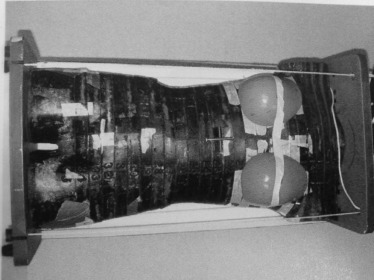
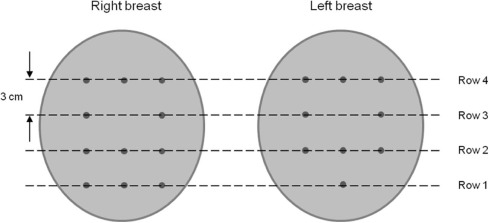
Four scanner models and three study protocols were used in scanning an anthropomorphic phantom with breast modules. Each protocol follows recommendations or guidelines from the American Association of Physicists in Medicine and the American College of Radiology. Twenty thermoluminescent dosimeters were placed inside the breast modules to measure breast tissue doses. Both the absolute and the normalized breast tissue doses were analyzed.
Results
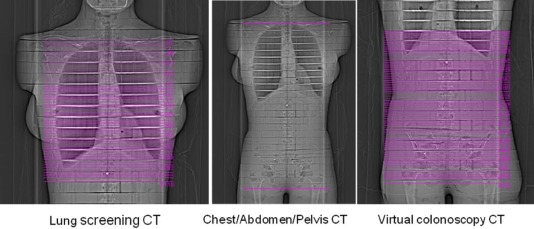
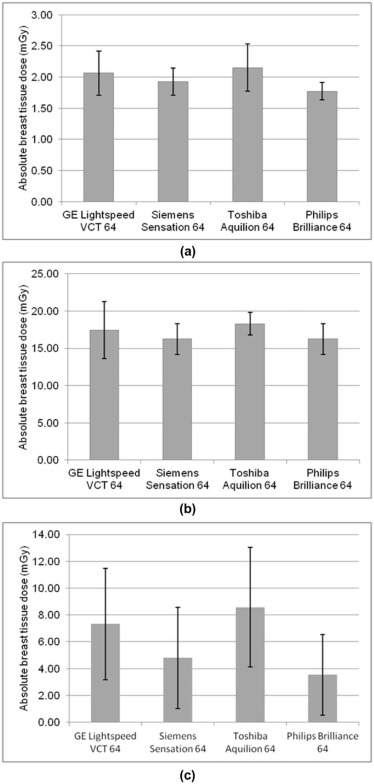
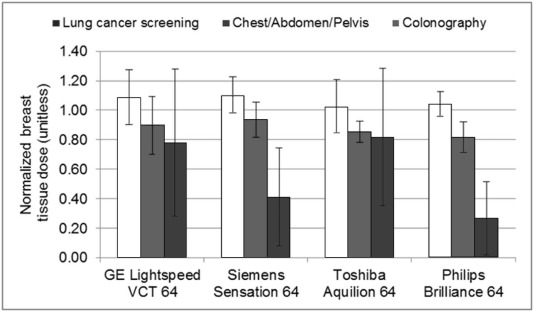
The mean glandular doses of a lung cancer screening CT, a chest/abdomen/pelvis CT, and a virtual colonoscopy CT are equivalent to less than 1, 5–7, and 1–3 two-view digital mammograms, respectively, for a standard-sized patient. The normalized breast dose differs significantly ( P < 0.01) between lung cancer screening CT and chest/abdomen/pelvis CT; however, it shows less than ±10% variation among scanner models for the same protocol. In virtual colonoscopy CT, breast tissue dose decreases with the distance between local tissues to the edge of the x-ray field, although the decreasing trend varies for different scanner models and protocol settings.
Conclusions
When breasts are entirely included in the primary x-ray field, breast dose by 64-slice CT is mainly protocol dependent, with the normalized breast dose about 15% lower for protocols with modulated mA than for those with constant mA; when breasts are only partially included in the primary beam field, breast dose by 64-slice CT is dependent on both the scanner model and the protocol settings.
Introduction
In recent years, public concerns over computed tomography (CT) radiation dose and its associated risks have spurred efforts to understand, manage, and optimize patient dose from CT studies . Among these efforts, the recording and reporting of patient dose play an important role for patient management in clinical practice. Although CT dose index (CTDI), a metric directly available from scanners, has long been used in reporting scanner radiation output, its practical value is limited because of its inability to account for patient variation. Organ dose has been considered a more valuable and suitable metric to meet clinical needs; it gives physical characterization of patient-specific radiation dose and forms the basis for risk estimates.
The determination of organ dose is a challenging task. The organ is affected not only by the scanner radiation output level, usually characterized by CTDI, but also by various other factors, such as patient size, study protocol, scanner model, and x-ray energy spectrum. A number of studies have been conducted with the aim of developing a robust yet simple method with acceptable accuracy for organ dose estimation . These studies employed either experimental methods using physical phantoms or numerical methods using validated Monte Carlo programs, although the majority of them were based on the latter because of the flexibility of simulation.
Get Radiology Tree app to read full this article<
Materials and Methods
Phantom and CT Scan Protocols
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 1
Acquisition Parameters for the Lung Screening CT Protocols Used on Different Systems
GE LightSpeed VCT Siemens SOMATOM Sensation 64 Philips Brilliance 64 Toshiba Aquilion 64 kVp 120 120 120 120 mAs 20 25 18 15 Rotation time (s) 0.5 0.5 0.75 0.5 Pitch 0.969 1.0 0.673 0.828 Detector configuration 32 × 0.625 mm 64 × 0.6 mm \* 64 × 0.625 mm 64 × 0.5 mm Bow-tie filter Large body Body Body Large CTDI vol (mGy) 1.9 1.8 1.7 2.1
CT, computed tomography; CTDI vol , volume CT dose index.
Get Radiology Tree app to read full this article<
TABLE 2
Acquisition Parameters for the Chest/Abdomen/Pelvis CT Protocols Used on Different Systems
GE LightSpeed VCT Siemens SOMATOM Sensation 64 Philips Brilliance 64 Toshiba Aquilion 64 kVp 120 120 120 120 Tube current modulation technique Auto mA and Smart mA Care Dose 4D D-DOM and Z-DOM Sure Exposure Rotation time (s) 0.4 0.5 0.75 0.5 Pitch 0.984 0.9 0.891 0.828 Detector configuration 64 × 0.625 mm 64 × 0.6 mm \* 64 × 0.625 mm 64 × 0.5 mm Bow-tie filter Large body Body Body Large CTDIvol (mGy) 20.0 20.0 20.0 20.0
CT, computed tomography; CTDI vol , volume CT dose index.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Breast Dose Measurements by Thermoluminescent Dosimeter (TLD)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Analysis
Get Radiology Tree app to read full this article<
Normalizedbreastdose=AbsolutebreastdoseRegionalCTDIvol, Normalized
breast
dose
=
Absolute
breast
dose
Regional
CTDI
vol
,
which characterizes the resulting breast tissue dose per unit radiation output to the breasts, and allows comparison among protocols with different radiation output levels. The regional CTDI vol is defined as follows:
CTDIvol,regional=CTDIvol,global×meanmAforimageslicesscontainingbreasttissuesmeanmAforallimageslices, CTDI
vol
,
regional
=
CTDI
vol
,
global
×
mean
mA
for
image
slicess
containing
breast
tissues
mean
mA
for
all
image
slices
,
where CTDI vol,global is the displayed CTDI vol from the scanner, representative of the dose index averaged over the entire scanner anatomy. For protocols using tube current modulation, CTDI vol,regional is more accurate than CTDI vol,global in characterizing the radiation output used on breast tissues. For protocols using constant mA, CTDI vol,regional becomes equal to CTDI vol,global .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
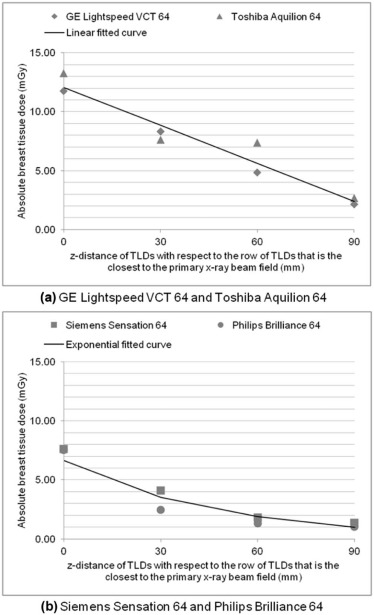
TABLE 3
Acquisition Parameters for the Virtual Colonoscopy CT Protocols Used on Different Systems
GE LightSpeed VCT Siemens SOMATOM Sensation 64 Philips Brilliance 64 Toshiba Aquilion 64 kVp 120 120 120 120 mAs (supine position) 100 150 100 75 mAs (prone position) 100 25 100 75 Rotation time (s) 0.5 0.5 0.75 0.5 Pitch 1.375 1.4 0.891 1.48 Detector configuration 64 × 0.625 mm 32 × 0.6 mm \* 64 × 0.625 mm 64 × 0.5 mm Bow-tie filter Large body Body Body Large CTDI vol (mGy) 10.0 10.0 10.0 10.0
CT, computed tomography; CTDI vol , volume CT dose index.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Acknowledgment
Get Radiology Tree app to read full this article<
References
1. Goske M.J., Applegate K.E., Boylan J., et. al.: Image gently: a national education and communication campaign in radiology using the science of social marketing. J Am Coll Radiol 2008; 5: pp. 1200-1205.
2. Brink J.A., Amis E.S.: Image wisely: a campaign to increase awareness about adult radiation protection. Radiology 2010; 257: pp. 601-602.
3. Boone J.M., Hendee W.R., McNitt-Gray M.F., et. al.: Radiation exposure from CT scans: how to close our knowledge gaps, monitor and safeguard exposure. Radiology 2012; 265: pp. 544-554.
4. McCollough C.H., Chen G.H., Kalender W., et. al.: Achieving routine submillisievert CT scanning: report from the summit on management of radiation dose in CT. Radiology 2012; 264: pp. 567-580.
5. Fujii K., Aoyama T., Yamauchi-Kawaura C., et. al.: Radiation dose evaluation in 64-slice CT examinations with adult and paediatric anthropomorphic phantoms. Br J Radiol 2009; 82: pp. 1010-1018.
6. DeMarco J.J., Cagnon C.H., Cody D.D., et. al.: Estimating radiation doses from multidetector CT using Monte Carlo simulations: effects of different size voxelized patient models on magnitudes of organ and effective dose. Phys Med Biol 2007; 52: pp. 2583-2597.
7. Angel E., Yaghmai N., Jude C.M., et. al.: Dose to radiosensitive organs during routine chest CT: effects of tube current modulation. AJR Am J Roentgenol 2009; 193: pp. 1340-1345.
8. Huda W., Sterzik A., Tipnis S., et. al.: Organ doses to adult patients for chest CT. Med Phys 2010; 37: pp. 842-847.
9. Turner A.C., Zhang D., Khatonabadi M., et. al.: The feasibility of a scanner-independent technique to estimate organ dose from MDCT scans: using CTDI vol to account for differences between scanners. Med Phys 2010; 37: pp. 1816-1825.
10. Li X., Samei E., Segars W.P., et. al.: Patient-specific radiation dose and cancer risk estimation in CT: part II. Application to patients. Med Phys 2011; 38: pp. 408-419.
11. Turner A.C., Zhang D., Khatonabadi M., et. al.: The feasibility of patient size-corrected, scanner-independent organ dose estimates for abdominal CT exams. Med Phys 2011; 38: pp. 820-829.
12. Lee C., Kim K.P., Long D.J., et. al.: Organ doses for reference pediatric and adolescent patients undergoing computed tomography estimated by Monte Carlo simulation. Med Phys 2012; 39: pp. 2129-2146.
13. Li X., Samei E., Williams C.H., et. al.: Effects of protocol and obesity on dose conversion factors in adult body CT. Med Phys 2012; 39: pp. 6550-6571.
14. Khatonabadi M., Kim H.J., Lu P., et. al.: The feasibility of a regional CTDI vol to estimate organ dose from tube current modulated CT exams. Med Phys 2013; 40: pp. 051903.
15. Tian X., Li X., Segars W.P., et. al.: Dose coefficients in pediatric and adult abdominopelvic CT based on 100 patient models. Phys Med Biol 2013; 58: pp. 8755-8768.
16. Li X., Segars W.P., Samei E.: The impact on CT dose of the variability in tube current modulation technology: a theoretical investigation. Phys Med Biol 2014; 59: pp. 4525-4548.
17. Sahbaee P., Segars W.P., Samei E.: Patient-based estimation of organ dose for a population of 58 adult patients across 13 protocol categories. Med Phys 2014; 41: pp. 072104.
18. Angel E., Yaghmai N., Jude C.M., et. al.: Monte Carlo simulations to assess the effects of tube current modulation on breast dose for multidetector CT. Phys Med Biol 2009; 54: pp. 497-511.
19. The 2007 Recommendations of the International Commission on Radiological Protection. ICRP Publication 103. Ann ICRP 2007; 37: pp. 2-4.
20. AAPM : CT scan protocols. Available at: http://www.aapm.org/pubs/CTProtocols/default.asp
21. ACR-SAR-SCBT-MR practice parameter for the performance of computed tomography colonoscopy in adults. 2014; Available at: http://www.acr.org
22. Hendrick R.E.: Radiation doses and cancer risks from breast imaging studies. Radiology 2010; 257: pp. 246-253.
23. Schilham A., van der Molen A.J., Prokop M., et. al.: Overranging at multisection CT: an underestimated source of excess radiation exposure. Radiographics 2010; 30: pp. 1057-1067.
24. Tian X., Li X., Segars W.P., et. al.: Pediatric chest and abdominopelvic CT: organ dose estimation based on 42 patient models. Radiology 2014; 270: pp. 535-547.