
Rationale and Objectives
To investigate residents’ knowledge of adverse effects of ionizing radiation, frequency of their education on radiation safety, and their use of radioprotective equipment.
Materials and Methods
Residents from 15/16 residency programs at Emory University were asked to complete a resident radiation safety survey through SurveyMonkey ® . The associations between the residents’ knowledge and use of radioprotective equipment with residents’ specialty and year of training were investigated.
Results
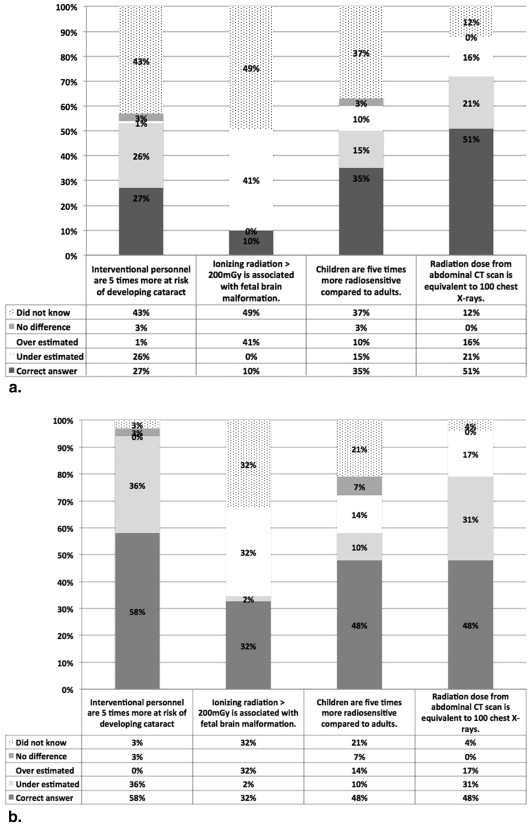
Response rate was 32.5% (173/532 residents). Thirty-nine percent residents reported radiation safety is discussed in their residency curriculum at least every 6 months. Ninety-five percent believed in a link between radiation exposure and development of cancer. Overall and Radiology residents’ knowledge about specific estimated dose effects (correct responses) was limited: radiation dose associated with fetus brain malformation in pregnancy (10% vs. 26%), risk of developing cataract in interventional personnel (27% vs. 47%), lifetime risk of cancer mortality from a single abdominal computed tomography (CT) in children (22% vs. 29%), greater radiosensitivity of children compared to adults (35% vs. 50%), and relative radiation dose from an abdominal CT compared to a chest x-ray (51% vs. 48%). Radiology residents had modestly higher knowledge. There was no significant difference in residents’ knowledge across their postgraduate training years. Use of lead thyroid shields was reported by 86% (97% radiology vs. 80% nonradiology; P = .03) and radiation-monitoring badges in 39% (68% radiology vs. 15% nonradiology; P < .001) of the residents.
Conclusions
Although radiology residents scored higher, knowledge of radiation safety for patients and healthcare workers is limited among residents regardless of medical specialty. These findings emphasize the need for educational initiatives.
The National Council for Radiation Protection and Measurement (NCRP) performs periodic surveys of radiation exposure from all sources to the American population. Their most recent survey reported that there is a rapid increase in average exposure to the American population from medical imaging, particularly computed tomography (CT) and cardiac nuclear medicine testing, from 15% in the early 1980s to 48% in 2006 . Effective dose is a risk estimate for a patient population from radiation exposure and is expressed in Sieverts (Sv) . The risk that a radiation dose will induce a cancer in a specific organ changes with age, gender, and individual patients’ variations of intrinsic radiation sensitivity. The population baseline lifetime cancer risk is 25%. For every 100 mSv of radiation dose to an average population, lifetime cancer mortality risk increases from 25% to 25.5% . The relationship between radiation dose and cancer risk is highly controversial; however, the scientific community generally assumes that there is no safe threshold at low dose (the linear no-threshold model) . There is growing public concern that low-dose (<100 mSv) ionizing radiation from diagnostic imaging may be associated with increased cancer risk depending on radiation dose and duration of exposure. Extrapolating from data of the Life Span Study of Japanese atomic bomb survivors, Brenner and Hall estimated that up to 2% of future cancers may be attributable to CT scanning.
The potential for cancer induction associated with medical radiation is even more important in children and pregnant women. The younger a patient, the more radiosensitive they are for certain tumors . They also have a greater postradiation exposure life expectancy compared to adults in which to manifest radiation-induced tumors .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Methods
Study Population
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Survey
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Analyses
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Study Population
Get Radiology Tree app to read full this article<
Table 1
Demographic Characteristics of Respondents
All Respondents, n (%) Response Rate, n (%) Gender Male 104/173 (60) — Female 69/173 (40) — Specialty 173/532 (33) Emergency medicine 22/162 (14) 22/59 (37) Family medicine 1/162 (1) 1/21 (5) General surgery 16/162 (10) 16/58 (28) Internal medicine 41/162 (25) 41/173 (24) Neurosurgery 2/162 (1) 2/18 (11) Nuclear medicine 3/162 (2) 3/4 (75) Obstetric/Gynecology 10/162 (6) 10/36 (28) Orthopedic surgery 6/162 (4) 6/25 (24) Plastic surgery 0/162 (0) 0/9 (0) Diagnostic radiology 36/162 (22) 36/61 (59) Radiation oncology 9/162 (6) 9/19 (47) Thoracic surgery 4/162 (3) 4/10 (40) Transitional year 9/162 (6) 9/22 (41) Urology 3/162 (2) 3/15 (20) Postgraduate year 1 50/174 (29) — 2 38/174 (22) — 3 46/174 (26) — 4 26/174 (15) — 5 or more 14/174 (8) —
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Radiation Safety as Part of the Residency Curriculum
Get Radiology Tree app to read full this article<
Table 2
Discussion Frequency and Comfort Level with Radiation Safety in Residency Programs
All Specialties, n (%) Specialties, n (%)P Value ¶ Medicine ∗ Surgery † Obstetric/Gynecology Radiology ‡ Discussion over radiation safety at least once in 6 months in residency. 64/164 (39) 13/68 (19) 5/30 (17) 3/10 (30) 38/45 (84)<.001 Discussion over radiation safety in pregnant women at least once in 6 months in residency § 66/145 (46) 13/51 (25) 7/28 (25) 6/10 (60) 37/45 (82)<.001 Discussion over radiation safety in children at least once in 6 months in residency ‖ 56/120 (47) 11/35 (31) 8/28 (28) 1/4 (25) 34/44 (77)<.001 Feeling comfortable making decisions for imaging in pregnancy § 87/143 (61) 17/50 (34) 18/28 (64) 8/10 (80) 38/44 (86)<.001 Feeling comfortable making decisions for imaging in children ‖ 79/106 (75) 17/28 (61) 19/26 (73) 2/3 (67) 37/41 (90).04
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Residents’ Perceptions and Knowledge about Radiation Safety across Postgraduate Year and by Gender
Postgraduate Year, n (%) Gender, n (%) 1 2 3 4 5P Value ‡ Male Female_P_ Value § Feeling comfortable making decisions for imaging in pregnancy ∗ 14/38 (37) 21/32 (65) 23/35 (66) 19/24 (79) 10/14 (71) .008 51/85 (60) 35/57 (61) .87 Feeling comfortable making decisions for imaging in children † 11/21 (52) 22/27 (81) 22/27 (81) 15/20 (75) 9/11 (82) .13 48/68 (70) 30/37 (81) .24 Knowledge There is a link between ionizing radiation and future development of cancer 40/42 (95) 35/36 (97) 39/41 (95) 23/25 (92) 13/13 (100) .81 95/97 (98) 54/59 (92).06 Ionizing radiation > 200 mGy is associated with fetal brain malformation. 2/42 (5) 2/36 (6) 6/41 (15) 4/25 (16) 2/13 (15) .36 9/97 (9) 6/59 (10) .85 There is a risk of developing cancer in patients or interventional personnel who are frequently exposed to ionizing radiation, but is uncommon 30/42 (71) 24/36 (67) 32/41 (78) 16/25 (64) 9/13 (69) .75 69/97 (71) 41/59 (69) .83 Patients undergoing fluoroscopy are at risk of developing skin burns depending on the dose of radiation they are exposed to 23/42 (55) 20/36 (56) 24/41 (59) 17/25 (68) 10/13 (77) .55 71/97 (73) 22/59 (37)<.001 Interventional personnel are five times more at risk of developing cataract 8/42 (19) 10/34 (29) 9/41 (22) 10/25 (40) 6/13 (46) .17 40/97 (41) 3/57 (5)<.001 Radiation dose from abdominal computed tomography (CT) scan is equivalent to 100 chest x-rays 17/40 (43) 18/33 (54) 27/40 (68) 10/25 (40) 6/13 (46) .14 52/96 (54) 26/55 (47) .41 Children are five times more radiosensitive compared to adults 12/41 (29) 10/33 (30) 17/40 (43) 9/25 (36) 5/13 (39) .74 36/96 (38) 17/56 (30) .37 Estimated risk of lifetime fatal cancer from a single abdominal CT is 1:1500 in children 4/41 (10) 11/33 (33) 12/41 (29) 2/25 (8) 6/13 (46) .007 22/96 (23) 13/57 (23) .99 Risk of lifetime fetal cancer is 20% in the American population. 7/41 (17) 6/33 (46) 13/39 (33) 6/25 (24) 5/13 (39) .29 26/96 (27) 11/55 (20) .33
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Residents’ Knowledge about Radiation Safety
Get Radiology Tree app to read full this article<
Table 4
Resident Knowledge and Perceptions about Radiation Safety across Specialties
All Specialties, n (%) Specialties, n (%)P Value § Medicine ∗ Surgery † Obstetric/Gynecology Radiology ‡ There is a link between ionizing radiation and future development of cancer 151/159 (95) 60/66 (91) 28/29 (96) 10/10 (100) 41/42 (98) .36 Ionizing radiation > 200 mGy is associated with fetal brain malformation 16/160 (10) 3/66 (5) 0/29 (0) 2/10 (20) 11/42 (26).04 There is a risk of developing cancer in patients or interventional personnel who are frequently exposed to ionizing radiation, but is uncommon 112/160 (70) 43/66 (65) 19/29 (65) 8/10 (80) 33/42 (79) .06 Patients undergoing fluoroscopy are at risk of developing skin burns depending on the dose of radiation they are exposed to 96/160 (60) 30/66 (45) 18/29 (62) 2/10 (20) 36/42 (86)<.001 Interventional personnel are five times more at risk of developing cataract 43/158 (27) 7/66 (11) 12/29 (41) 1/9 (11) 20/42 (47)<.001 Radiation dose from abdominal computed tomography (CT) scan is equivalent to 100 chest x-rays 79/154 (51) 36/62 (58) 16/29 (55) 4/10 (40) 19/40 (48) .09 Children are five times more radiosensitive compared to adults 54/155 (35) 18/63 (28) 9/29 (31) 3/10 (30) 20/40 (50) .09 Risk of lifetime fetal cancer from abdominal CT (performed based on adult protocol) is 1:1500 35/156 (22) 10/63 (16) 10/29 (34) 1/10 (10) 12/41 (29) .51 Risk of lifetime fatal cancer is 20% in the American population 38/154 (25) 14/63 (22) 5/29 (17) 0/9 (0) 16/40 (40).03
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Radiology Specialty Residents
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 5
Relative Knowledge of Radiation Safety and Use of Radioprotective Equipment among Diagnostic Radiology Residents Compared to Other Specialties (Percent Correct Responses)
Diagnostic Radiology, n (%) Nuclear Medicine and Radiation Oncology, n (%) All Other Specialties, n (%)P Value † Ionizing radiation > 200 mGy is associated with fetal brain malformation. 11/31 (35) 0/11 (0) 5/105 (5).001 Patients undergoing fluoroscopy are at risk of developing skin burns depending on the dose of radiation they are exposed to. 30/31 (97) 6/11 (54) 50/105 (48)<.001 Interventional personnel are five times more at risk of developing cataract. 18/31 (58) 2/11 (18) 20/104 (19)<.001 Radiation dose from abdominal computed tomography (CT) scan is equivalent to 100 chest x-rays. 14/29 (48) 5/11 (45) 56/101 (55) .26 Children are five times more radiosensitive compared to adults. 14/29 (48) 6/11 (54) 30/102 (30) .09 Risk of lifetime fatal cancer from abdominal CT (performed based on adult protocol) is 1:1500. 8/30 (27) 4/11 (36) 21/102 (20) .96 Reported frequency of wearing radiation-monitoring badges everyday or most of the time ∗ 18/28 (64) 3/3 (100) 6/40 (15)<.001 Reported frequency of wearing lead thyroid shield ∗ 28/28 (100) 2/3 (67) 32/40 (80).03 Image Gently/Image Wisely use 13/33 (39) 1/12 (8) 3/105 (3)<.001
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Use of Radiation-monitoring Badges and Lead Thyroid Shields
Get Radiology Tree app to read full this article<
Table 6
Importance of Wearing Radiation Safety Badges and Lead Apron across Specialties
All Specialties Radiology ∗ Nonradiology † P Value Importance of wearing radiation-monitoring badges, mean ± standard deviation (SD) 4.3 ± 0.9 4.2 ± 0.2 4.5 ± 0.1 .12 ‡ Reported frequency of wearing radiation-monitoring badges everyday or most of the time, n (%) 30/78 (39) 21/31 (68) 6/40 (15)<.001 § Importance of wearing lead thyroid shield, mean ± SD 4.8 ± 0.5 4.8 ± 0.07 4.8 ± 0.1 .52 ‡ Reported frequency of wearing lead thyroid shield, N (%) 67/78 (86) 30/31 (97) 32/40 (80).03 § Reported preference of two-piece lead aprons, n (%) 52/79 (66) 25/31 (80) 23/40 (57).04 § Reported availability of two-piece lead aprons, n (%) 40/79 (51) 19/31 (61) 17/40 (42) .12 §
Only residents who are exposed to ionizing radiation were queried.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Limitations
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
References
1. National Council for Radiation Protection and Measurement. Available at: http://www.ncrponline.org . Accessed May 20, 2013.
2. NCRP Report No. 160, Ionizing radiation exposure of the population of the United States. Recommendation of National Council on Radiation Protection and Measurement. 2009. Avaialble at: http://www.ncrponline.org/Publications/Press_Releases/160press.html .
3. International Atomic Energy Agency. Radiation protection of patients. Available at: https://rpop.iaea.org/RPOP/RPoP/Content/InformationFor/HealthProfessionals/1_Radiology/QuantitiesUnits.htm . Accessed May 30, 2013.
4. Brenner D.J., Hall E.J.: Computed tomography—an increasing source of radiation exposure. N Engl J Med 2007; 357: pp. 2277-2284.
5. Balter S., Zanzonico P., Reiss G.R., et. al.: Radiation is not the only risk. AJR Am J Roentgenol 2011; 196: pp. 762-767.
6. Understanding radiation. United Kingdom: Health Protection Agency. Updated 10 December 2008. Health Protection Agency. Available at: http://www.hpa.org.uk/ . Accessed May 20, 2013.
7. Little M.P., Wakeford R., Tawn E.J., et. al.: Risks associated with low doses and low dose rates of ionizing radiation: why linearity may be (almost) the best we can do. Radiology 2009; 251: pp. 6-12.
8. Bogdanich W. “Radiation Boom” series. The New York Times. 2010–2011. Available at: http://topics.nytimes.com/top/news/us/series/radiation_boom/index.html . Accessed May 20, 2013.
9. Mathews J.D., Forsythe A.V., Brady Z., et. al.: Cancer risk in 680 000 people exposed to computed tomography scans in childhood or adolescence: data linkage study of 11 million Australians. BMJ 2013; 346: pp. f2360.
10. Pearce M.S., Salotti J.A., Little M.P., et. al.: Radiation exposure from CT scans in childhood and subsequent risk of leukaemia and brain tumours: a retrospective cohort study. Lancet 2012; 380: pp. 499-505.
11. Berrington de Gonzalez A., Mahesh M., Kim K.P., et. al.: Projected cancer risks from computed tomographic scans performed in the United States in 2007. Arch Intern Med 2009; 169: pp. 2071-2077.
12. United Nations Scientific Committee on the Effect of Atomic Radiation (UNSCEAR). No immediate health risks from Fukushima nuclear accident says UN Expert Science Panel. Press Release, 2013. Available at: http://www.unis.unvienna.org/unis/en/pressrels/2013/unisinf475.html . Accessed June 12, 2013.
13. Lee C., Lee C., Staton R.J., et. al.: Organ and effective doses in pediatric patients undergoing helical multislice computed tomography examination. Med Phys 2007; 34: pp. 1858-1873.
14. Brenner D.J.: Estimating cancer risks from pediatric CT: going from the qualitative to the quantitative. Pediatr Radiol 2002; 32: 228–3; discussion 42–4
15. Wong C.S., Huang B., Sin H.K., et. al.: A questionnaire study assessing local physicians, radiologists and interns’ knowledge and practice pertaining to radiation exposure related to radiological imaging. Eur J Radiol 2012; 81: pp. e264-e268.
16. Zhou G.Z., Wong D.D., Nguyen L.K., et. al.: Student and intern awareness of ionising radiation exposure from common diagnostic imaging procedures. J Med Imaging Radiat Oncol 2010; 54: pp. 17-23.
17. Thomas K.E., Parnell-Parmley J.E., Haidar S., et. al.: Assessment of radiation dose awareness among pediatricians. Pediatr Radiol 2006; 36: pp. 823-832.
18. Huda W.: Effective doses to adult and pediatric patients. Pediatr Radiol 2002; 32: pp. 272-279.
19. Merzenich H., Krille L., Hammer G., et. al.: Paediatric CT scan usage and referrals of children to computed tomography in Germany—a cross-sectional survey of medical practice and awareness of radiation related health risks among physicians. BMC Health Serv Res 2012; 12: pp. 47.
20. Krille L., Hammer G.P., Merzenich H., et. al.: Systematic review on physician’s knowledge about radiation doses and radiation risks of computed tomography. Eur J Radiol 2010; 76: pp. 36-41.
21. Rice H.E., Frush D.P., Harker M.J., et. al.: Peer assessment of pediatric surgeons for potential risks of radiation exposure from computed tomography scans. J Pediatr Surg 2007; 42: pp. 1157-1164.
22. Berrington de Gonzalez A., Darby S.: Risk of cancer from diagnostic X-rays: estimates for the UK and 14 other countries. Lancet 2004; 363: pp. 345-351.
23. Lee C.I., Haims A.H., Monico E.P., et. al.: Diagnostic CT scans: assessment of patient, physician, and radiologist awareness of radiation dose and possible risks. Radiology 2004; 231: pp. 393-398.
24. McBride J.F., Wardrop R.M., Paxton B.E., et. al.: Effect on examination ordering by physician attitude, common knowledge, and practice behavior regarding CT radiation exposure. Clin Imaging 2012; 36: pp. 455-461 e1.
25. Brink J.A., Amis E.S.: Image Wisely: a campaign to increase awareness about adult radiation protection. Radiology 2010; 257: pp. 601-602.
26. Yucel A., Alyesil C., Sim S.: Physicians’ knowledge about ionizing radiation and radiological imaging techniques: a cross-sectional survey. Acta Radiol 2011; 52: pp. 537-539.
27. Strauss K.J., Goske M.J., Kaste S.C., et. al.: Image gently: ten steps you can take to optimize image quality and lower CT dose for pediatric patients. AJR Am J Roentgenol 2010; 194: pp. 868-873.
28. Brenner D., Elliston C., Hall E., et. al.: Estimated risks of radiation-induced fatal cancer from pediatric CT. AJR Am J roentgenol 2001; 176: pp. 289-296.
29. Picano E.: Sustainability of medical imaging. BMJ 2004; 328: pp. 578-580.
30. The International Commission on Radiological Protection. Available at http://www.icrp.info . Accessed May 31, 2013.
31. American College of Radiology. ACR technical standard for management of the use of radiation in fluoroscopic procedures. 2008. Available at: http://www.acr.org/∼/media/F22C9D1FF46F43AAB001F9ED0466B7E9.pdf . Accessed May 31, 2013.
32. Goergen S.: They don’t know what they don’t know. J Med Imaging Radiat Oncol 2010; 54: pp. 1-2.
33. Hassan M., Patil A., Channel J., et. al.: Do we glow? Evaluation of trauma team work habits and radiation exposure. J Trauma Acute Care Surg 2012; 73: pp. 605-611.
34. Son B.K., Lee K.T., Kim J.S., et. al.: Lack of radiation protection for endoscopists performing endoscopic retrograde cholangiopancreatography. Korean J Gastroenterol 2011; 58: pp. 93-99.
35. Amis E.S., Butler P.F., Applegate K.E., et. al.: American College of Radiology white paper on radiation dose in medicine. J Am Coll Radiol 2007; 4: pp. 272-284.
36. Miller D.L., Society for Interventional Radiology: Interventional fluoroscopy: reducing radiation risks for patients and staff. J Vasc Interv Radiol 2009; 20: pp. S274.
37. Balter S., Miller D.L.: The new Joint Commission sentinel event pertaining to prolonged fluoroscopy. J Am Coll Radiol 2007; 4: pp. 497-500.
38. American College of Radiology: ACR appropriateness criteria.2010.American College of RadiologyReston, VA
39. Image Gently. Available at http://www.imagegently.com . Accessed December 25, 2012.
40. Hendee W.R.: Teaching physics to radiology residents. AJR Am J Roentgenol 2009; 192: pp. 855-858.