
Rationale and Objectives
To explore the morphological characteristics of ablated lesions and find which combination of duration, temperature, and power was preferable to create largest lesion size with monopolar perfusion electrodes.
Materials and Methods
Using monopolar perfusion electrodes to create 72 lesions in 30 excised porcine livers with radiofrequency radiation at different durations (5, 10, 15, and 20 minutes), temperatures (83°C, 93°C, 103°C, and 113°C), and powers (20, 30, and 40 W). Lesion volumes were calculated from longitudinal diameters and transverse diameters. Morphological characteristics were assessed microscopically from slides stained with hematoxylin and eosin.
Results
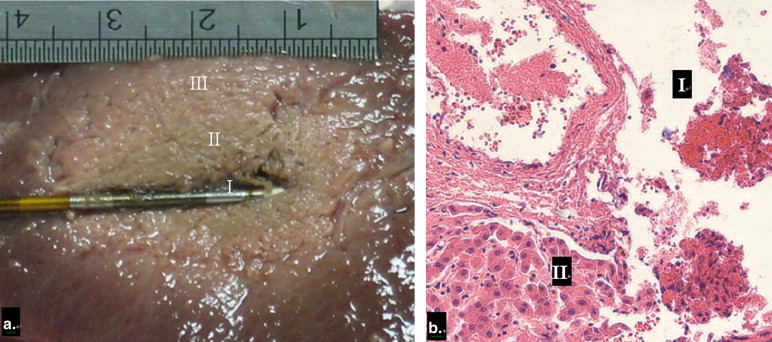
Positive correlations were found between duration and longitudinal diameter ( r = 0.66; P < .001), transverse diameter ( r = 0.66; P < .001), distance of ablation beyond the electrode tip ( r = 0.56; P < .001), and volume of lesions ( r = 0.66; P < .001). Temperature was also positively correlated with longitudinal diameter ( r = 0.70; P < .001), transverse diameter ( r = 0.72; P < .001), distance of ablation beyond the electrode tip ( r = 0.61; P < .001), and lesion volume ( r = 0.711; P < .001). Lesion size did not increase when duration was longer than 15 minutes and temperature was higher than 103°C. Power was not correlated with lesion size. Lesion size did not increase with increasing power. Macroscopically, all lesions were elliptical in cross section and appeared three zones: a central zone (I), a coagulated necrotic zone (II), and a hemorrhagic and edematous zone (III) from inside to outside. Microscopically, cells morphology and the nucleus were irregular or even disappeared in zone I. In zone II and III, cells did not appear deformation.
Conclusion
Duration and temperature, not power, affected lesion size. The largest lesion size was about 3.5 cm × 2.5 cm × 2.5 cm as temperature and duration was 15 minutes/103°C.
In the last two decades, percutaneous radiofrequency ablation (RFA) has been designed to destroy tumors by means of heat and has become increasingly popular as an alternative form of minimally invasive therapy for controlling primary and secondary hepatic malignancies because it is safe, effective, simple, and has fewer postoperative complications and higher survival rates than other ablative techniques when surgery is not indicated . However, a major limitation of RFA is its inability to create an large enough lesion size of coagulation necrosis produced by a monopolar radiofrequency electrode, which does not encompass the entire tumors and the required safety margin of 0.5–1.0 cm . Initially, radiofrequency electrodes available produced small volumes of necrosis with destruction of liver limited to less than 1.6 cm in diameter after a single insertion because of carbonization, desiccation, and tissue boiling, which increase impedance around electrodes . Proposed approaches to solve this lesion size limitation have been studied. Irrigating the electrode with cooling liquid (cool-tip electrode) maintains the electrode low temperature and prevents the impedance rise . Another approach is to infuse saline through the holes at the end of perfusion electrode tip to improve the ablated tissues conductivity and enhance radiofrequency energy distribution outward .
We produced ablation lesions in excised porcine livers with RITA UniBlate, a type of monopolar perfusion electrode. The purpose of this study was to evaluate the morphological characteristics of these lesions. We varied the duration, temperature, and power to find which combination is preferable to create the largest lesion size.
Materials and methods
RFA System
Get Radiology Tree app to read full this article<
Experimental Design
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Characteristics of Lesions Created by Radiofrequency Ablation in Excised Porcine livers
Group Subgroup Combination ∗ (minutes/°C/W) Longitudinal Diameter (cm) Transverse Diameters (cm) Distance of Ablation Beyond the Electrode Tip (cm) Volume (cm 3 ) A 1 5/103/30 2.58 ± 0.05 1.57 ± 0.09 0.07 ± 0.04 3.34 ± 0.42 2 10/103/30 3.01 ± 0.07 1.97 ± 0.03 0.44 ± 0.04 6.13 ± 0.30 3 15/103/30 3.50 ± 0.09 2.46 ± 0.13 0.75 ± 0.12 11.12 ± 1.15 4 20/103/30 3.48 ± 0.13 2.47 ± 0.04 0.64 ± 0.24 11.13 ± 0.72 B 5 15/83/30 2.53 ± 0.03 1.51 ± 0.06 0.01 ± 0.01 3.02 ± 0.23 6 15/93/30 3.05 ± 0.09 1.95 ± 0.05 0.49 ± 0.03 6.08 ± 0.42 3 15/103/30 3.50 ± 0.09 2.46 ± 0.13 0.75 ± 0.12 11.12 ± 1.15 7 15/113/30 3.56 ± 0.05 2.50 ± 0.14 0.71 ± 0.17 11.67 ± 1.32 C 8 15/103/20 3.49 ± 0.06 2.44 ± 0.04 0.78 ± 0.13 10.84 ± 0.50 3 15/103/30 3.50 ± 0.09 2.46 ± 0.13 0.75 ± 0.12 11.12 ± 1.15 9 15/103/40 3.50 ± 0.14 2.46 ± 0.04 0.85 ± 0.12 11.04 ± 0.68
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Measurements and Calculations
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Diameters and Volumes of Ablated Lesions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Morphologic and Pathologic Features of Ablated Lesions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. McGahan J.P., Browning P.D., Brock J.M., et. al.: Hepatic ablation using radiofrequency electrocautery. Invest Radiol 1990; 25: pp. 267-270.
2. Mertyna P., Goldberg W., Yang W., et. al.: Thermal ablation a comparison of thermal dose required for radiofrequency-, microwave-, and laser-induced coagulation in an ex vivo bovine liver model. Acad Radiol 2009; 16: pp. 1539-1548.
3. Lee W.S., Yun S.H., Chun H.K., et. al.: Clinical outcomes of hepatic resection and radiofrequency ablation in patients with solitary colorectal liver metastasis. J Clin Gastroenterol 2008; 42: pp. 945-949.
4. Hur H., Ko Y.T., Min B.S., et. al.: Comparative study of resection and radiofrequency ablation in the treatment of solitary colorectal liver metastases. Am J Surg 2009; 197: pp. 728-736.
5. Nikfarjam M., Shereef S., Kimchi E.T., et. al.: Survival outcomes of patients with colorectal liver metastases following hepatic resection or ablation in the era of effective chemotherapy. Ann Surg Oncol 2009; 16: pp. 1860-1867.
6. Reuter N.P., Woodall C.E., Scoggins C.R., et. al.: Radiofrequency ablation vs. resection for hepatic colorectal metastasis: therapeutically equivalent?. J Gastrointest Surg 2009; 13: pp. 486-491.
7. McGahan J.P., Dodd G.D.: Radiofrequency ablation of the liver: current status. Am J Roentgenol 2001; 176: pp. 3-16.
8. Dodd G.D., Soulen M.C., Kane R.A., et. al.: Minimally invasive treatment of malignant hepatic tumors: at the threshold of a major breakthrough. Radiographics 2000; 20: pp. 9-27.
9. Sartori S., Tombesi P., Macario F., et. al.: Subcapsular liver tumors treated with percutaneous radiofrequency ablation: a prospective comparison with nonsubcapsular liver tumors for safety and effectiveness. Radiology 2008; 248: pp. 670-679.
10. Tateishi R., Shiina S., Ohki T., et. al.: Treatment strategy for hepatocellular carcinoma: expanding the indications for radiofrequency ablation. J Gastroenterol 2009; 44: pp. 142-146.
11. Chen M.H., Yang W., Yan K., et. al.: Treatment efficacy of radiofrequency ablation of 338 patients with hepatic malignant tumor and the relevant complications. World J Gastroenterol 2005; 11: pp. 6395-6401.
12. Decadt B., Siriwardena A.K.: Radiofrequency ablation of liver tumours: systematic review. Lancet Oncol 2004; 5: pp. 550-560.
13. Ni Y., Mulier S., Miao Y., et. al.: A review of the general aspects of radiofrequency ablation. Abdom Imaging 2005; 30: pp. 381-400.
14. Lorentzen T.: A cooled needle electrode for radiofrequency tissue ablation: thermodynamic aspects of improved performance compared with conventional needle design. Acad Radiol 1996; 3: pp. 556-563.
15. Solbiati L., Livraghi T., Goldberg S.N., et. al.: Percutaneous radiofrequency ablation of hepatic metastases from colorectal cancer: long-term results in117 patients. Radiology 2001; 221: pp. 159-166.
16. de Baere T., Elias D., Dromain C., et. al.: Radiofrequency ablation of 100 hepatic metastases with a mean follow-up of more than 1 year. Am J Roentgenol 2000; 175: pp. 1619-1625.
17. Livraghi T., Goldberg S.N., Lazzaroni S., et. al.: Hepatocellular carcinoma: radio-frequency ablation of medium and large lesions. Radiology 2000; 214: pp. 761-768.
18. Goldberg S.N., Gazelle GS., Halpern E.F., et. al.: Radiofrequency tissue ablation: importance of local temperature along the electrode tip exposure in determining lesion shape and size. Acad Radiol 1996; 3: pp. 212-318.
19. Goldberg S.N., Gazelle S., Dawson S., et. al.: Tissue ablation with radiofrequency: effect of probe size, gauge, duration and temperature on lesion volume. Acad Radiol 1995; 2: pp. 399-404.
20. Lee J.M., Jin G.Y., Li C.A., et. al.: Percutaneous radiofrequency thermal ablation of lung VX2 tumors in a rabbit model using a cooled tip-electrode: feasibility, safety, and effectiveness. Invest Radiol 2003; 38: pp. 129-139.
21. Mulier S., Ni Y., Miao Y., et. al.: Size and geometry of hepatic radiofrequency lesions. EJSO 2003; 29: pp. 867-878.
22. Lee J.M., Han J.K., Kim S.H., et. al.: Bipolar radiofrequency ablation in ex vivo bovine liver with the open-perfused system versus the cooled-wet system. Eur Radiol 2005; 15: pp. 759-764.
23. Kim Y.K., Lee J.M., Kim S.W., et. al.: Combined radiofrequency ablation and hot saline injection in rabbit liver. Invest Radiol 2003; 38: pp. 725-732.
24. Lee J.M., Kim S.H., Han J.K., et. al.: Ex vivo experiment of saline-enhanced hepatic bipolar radiofrequency ablation with a perfused needle electrode: comparison with conventional monopolar and simultaneous monopolar modes. Cardiovasc Intervent Radiol 2005; 28: pp. 338-345.
25. Lee J.M., Han J.K., Kim H.C., et. al.: Switching monopolar radiofrequency ablation technique using multiple, internally cooled electrodes and a multichannel generator: ex vivo and in vivo pilot study. Invest Radiol 2007; 42: pp. 163-171.
26. Simon C.J., Dupuy D.E., Iannitti D.A., et. al.: Intraoperative triple antenna hepatic microwave ablation. Am J Roentgenol 2006; 187: pp. W333-W340.
27. Burdío F., Navarro A., Berjano E.J., et. al.: Radiofrequency hepatic ablation with internally cooled electrodes and hybrid applicators with distant saline infusion using an in vivo porcine model. EJSO 2008; 34: pp. 822-830.
28. Rhim H., Choi D., Kim Y.S., et. al.: Ultrasonography-guided percutaneous radiofrequency ablation of hepatocellular carcinomas: a feasibility scoring system for planning sonography. Eur J Radiol 2009; [Epub ahead of print]
29. Gillams A.R.: Radiofrequency ablation in the management of liver tumors. Eur J Surg Oncol 2003; 29: pp. 9-16.
30. Buscarini E., Savoia A., Brambilla G., et. al.: Radiofrequency thermal ablation of liver tumors. Eur Radiol 2005; 15: pp. 884-894.
31. Hong K., Georgiades C.S., Geschwind J.F.: Technology insight: image-guided therapies for hepatocellular carcinoma—intra-arterial and ablative techniques. Nat Clin Pract Oncol 2006; 3: pp. 315-324.
32. Poon R.T., Fan S.T., Tsang F.H., et. al.: Locoregional therapies for hepatocellular carcinoma: a critical review from the surgeon’s perspective. Ann Surg 2002; 235: pp. 466-486.
33. Patterson E.J., Scudamore C.H., Owen D.A., et. al.: Radiofrequency ablation of porcine liver in vivo: effects of blood flow and treatment time on lesion size. Ann Surg 1998; 227: pp. 559-565.
34. Curley S.A.: Radiofrequency ablation of malignant liver tumors. Oncologist 2001; 6: pp. 14-23.
35. Goldberg N.S., Dupuy D.E.: Image-guided radiofrequency tumor ablation: challenges and opportunities–part 1. J Vasc Interv Radiol 2001; 12: 102l-1032
36. de Baere T., Denys A., Denys W.B., et. al.: Radiofrequency liver ablation: experimental comparative study of water-cooled versus expandable systems. Am J Roentgenol 2001; 176: pp. 187-192.
37. Shibata T., Shibata T., Maetani Y., et. al.: Radiofrequency ablation for small hepatocellular carcinoma: prospective comparison of internally cooled electrode and expandable electrode. Radiology 2006; 238: pp. 346-353.
38. Goldberg S.N., Ahmed M., Gazelle G.S., et. al.: Radio-frequency thermal ablation with NaCl solution injection: effect of electrical conductivity on tissue heating and coagulation-phantom and porcine liver study. Radiology 2001; 219: pp. 157-165.
39. Lobo S.M., Afzal K.S., Ahmed M., et. al.: Radiofrequency ablation: modeling the enhanced temperature response to adjuvant NaCl pretreatment. Radiology 2004; 230: pp. 175-182.
40. Lee J.M., Han J.K., Chang J.M., et. al.: Radiofrequency ablation of the porcine liver in vivo: increased coagulation with an internally cooled perfusion electrode. Acad Radiol 2006; 13: pp. 343-352.
41. Ni Y., Miao Y., Mulier S., et. al.: A novel “cooled-wet” electrode for radiofrequency ablation. Eur Radiol 2000; 10: pp. 852-854.
42. Miao Y., Ni Y., Yu J., et. al.: A comparative study on validation of a novel cooled-wet electrode for radiofrequency liver ablation. Invest Radiol 2000; 35: pp. 438-444.
43. Lorentzen T., Christensen N.E., Nolste C.P., et. al.: Radiofrequency tissue ablation with a cooled needle in vitro: ultrasonography, dose response, and lesion temperature. Acad Radiol 1997; 4: pp. 292-297.
44. Miao Y., Ni Y., Bosmans H., et. al.: Radiofrequency ablation for eradication of pulmonary tumor in rabbits. J Surg Res 2001; 99: pp. 265-271.
45. Miao Y., Ni Y., Bosmans H., et. al.: Radiofrequency ablation for eradication of renal tumor in a rabbit model by using a cooled-tip electrode technique. Ann Surg Oncol 2001; 8: pp. 651-657.
46. Miao Y., Ni Y., Mulier S., et. al.: Treatment of VX2 liver tumor in rabbits with “wet” electrode mediated radio-frequency ablation. Eur Radiol 2000; 10: pp. 188-194.
47. Shen P., Geisinger K.R., Zagoria R., et. al.: Pathologic correlation study of microwave coagulation therapy for hepatic malignancies using a three-ring probe. J Gastrointest Surg 2007; 11: pp. 603-611.
48. Ng K.K., Lam C.M., Poon R.T., et. al.: Porcine liver: morphologic characteristics and cell viability at experimental radiofrequency ablation with internally cooled electrodes. Radiology 2005; 235: pp. 478-486.