
Rationale and Objectives
Conventional mammographic image contrast is derived from x-ray absorption, resulting in breast structure visualization due to density gradients that attenuate radiation without distinction between transmitted, scattered, or refracted x-rays. Diffraction-enhanced imaging (DEI) allows for increased contrast with decreased radiation dose compared to conventional mammographic imaging because of monochromatic x-rays, its unique refraction-based contrast mechanism, and excellent scatter rejection. However, a lingering drawback to the clinical translation of DEI has been the requirement for synchrotron radiation.
Materials and Methods
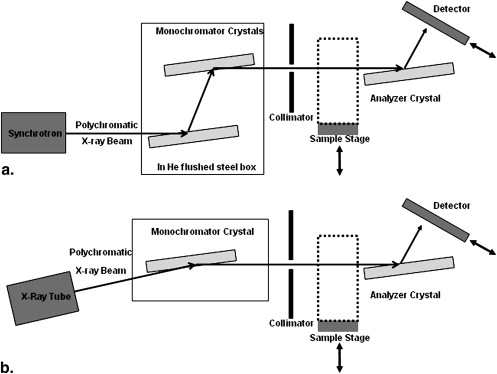
The authors’ laboratory developed a DEI prototype (DEI-PR) using a readily available tungsten x-ray tube source and traditional DEI crystal optics, providing soft tissue images at 60 keV. Images of full-thickness human breast tissue specimens were acquired on synchrotron-based DEI (DEI-SR), DEI-PR, and digital mammographic systems. A panel of expert radiologists evaluated lesion feature visibility and correlation with pathology after receiving training on the interpretation of refraction contrast mammographic images.
Results
For mammographic features (mass, calcification), no significant differences were detected between the DEI-SR and DEI-PR systems. Benign lesions were perceived as better seen by radiologists using the DEI-SR system than the DEI-PR system at the [111] reflectivity, with generalizations limited by small sample size. No significant differences between DEI-SR and DEI-PR were detected for any other lesion type (atypical, cancer) at either crystal reflectivity.
Conclusions
Thus, except for benign lesion characterizations, the DEI-PR system’s performance was roughly equivalent to that of the traditional DEI system, demonstrating a significant step toward clinical translation of this modality for breast cancer applications.
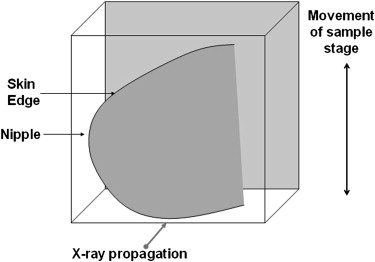
Cancer imparts distinct and measurable changes in breast tissue at the cellular level. In conventional, attenuation-based radiography, variations in the density of the breast tissue lead to varied x-ray attenuation and thus varied intensity in the image. Contrast based on the spatial distribution of x-ray attenuation is not always sufficient to distinguish between normal and cancerous tissues. However, additional contrast can be gained from the refraction of x-rays. Microscopic and macroscopic alterations in the breast tissue may cause x-ray refraction, a minute change in the direction of x-ray propagation, which is exploited by phase-contrast imaging. X-ray refraction contrast is not yet widely used in medical imaging, although several phase-contrast imaging devices are in various stages of research and development .
Diffraction-enhanced imaging (DEI) is a specific type of analyzer-based phase-contrast imaging. Traditionally, DEI has used intense, highly collimated synchrotron radiation (SR) to produce images on the basis of absorption, refraction, and extinction contrast . The application of DEI to breast imaging has consistently provided a superior signal-to-noise ratio (contrast) compared to conventional radiographic images .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Specimen Selection
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
DEI
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Full-field Digital Mammography
Get Radiology Tree app to read full this article<
Pathologic Correlation
Get Radiology Tree app to read full this article<
Flux, Dose, and Signal Measured at the Detector
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Specimen Radiographic Density
Specimen Percentage Density Glandular Thickness (cm) Adipose Thickness (cm) 1 20% 1.35 5.40 2 30% 2.55 5.95 3 20% 1.70 6.80 4 50% 2.25 2.25 5 30% 2.55 5.95 6 30% 2.55 5.95
Get Radiology Tree app to read full this article<
Reader Study
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Methods
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
![Figure 3, Comparison of benign lesion characteristic visibility. This specimen (12.5 × 17.5 cm) contains a circled region of interest, which represents dense stromal sclerosis, a biopsy cavity, fibrocystic change, and focal atypical ductal hyperplasia with associated calcifications. (a) Digital mammographic standard, acquired at 22 keV. Diffraction-enhanced images (b–e) were acquired at 60 keV using the [333] reflectivity. Synchrotron-based diffraction-enhanced images are displayed in the first column , and prototype diffraction-enhanced images are shown in the second column . The top row in (b) and (c) displays the +0.5 Darwin width ( W D ) rocking-curve position, and the bottom row in (d) and (e) displays the −0.5 W D rocking-curve position.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/RadiologistEvaluationofanXrayTubeBasedDiffractionEnhancedImagingPrototypeUsingFullThicknessBreastSpecimens/2_1s20S1076633209003031.jpg)
![Figure 4, Comparison of malignant lesion characteristic visibility. The magnified views of this region of interest (approximately 6.5 × 5 cm) represent apocrine-type ductal carcinoma in situ (nuclear grade 2–3 with necrosis without associated calcifications), proliferative fibrocystic change, and duct ectasia. (a) Digital mammographic standard, acquired at 29 keV. Diffraction-enhanced images (b–e) were acquired at 60 keV using the [333] reflectivity. The first column (b,c) was acquired using synchrotron-based diffraction-enhanced imaging (DEI), and the second column (e,d) was acquired using prototype DEI. The top row in (b) and (e) displays the +0.5 Darwin width ( W D ) rocking-curve position, and the bottom row in (c) and (d) displays the −0.5 W D rocking-curve position.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/RadiologistEvaluationofanXrayTubeBasedDiffractionEnhancedImagingPrototypeUsingFullThicknessBreastSpecimens/3_1s20S1076633209003031.jpg)
![Figure 5, Effect of crystal reflectivity on lesion feature visibility. This magnified region of interest (approximately 3.5 × 4.5 cm) contains duct ectasia, proliferative fibrocystic change, stromal sclerosis, and calcifications at pathologic analysis. The digital mammographic image is displayed in (a) , and (b) through (d) show the region of interest acquired on the synchrotron-based diffraction-enhanced imaging (DEI-SR) system at the [333] reflectivity at the +0.5 Darwin width ( W D ), −0.5 W D , and peak rocking-curve positions, respectively. (e–g) Same region of interest and rocking-curve positions acquired using the DEI-SR system at the [111] reflectivity.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/RadiologistEvaluationofanXrayTubeBasedDiffractionEnhancedImagingPrototypeUsingFullThicknessBreastSpecimens/4_1s20S1076633209003031.jpg)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
![Figure 6, Reader study analysis of radiographic feature visibility. Three expert radiologists ranked radiographic feature visibility on a scale ranging from 1 (not easily appreciated) to 5 (easily appreciated). These scores were averaged for all masslike and calcification regions of interest as perceived on the synchrotron-based diffraction-enhanced imaging (DEI-SR), prototype DEI (DEI-PR), and digital mammographic (DM) systems. Average scores obtained for images acquired at the [333] reflectivity (left) and the [111] reflectivity (right) are shown.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/RadiologistEvaluationofanXrayTubeBasedDiffractionEnhancedImagingPrototypeUsingFullThicknessBreastSpecimens/5_1s20S1076633209003031.jpg)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Reader Study Analysis of DEI Correlation with Pathologic Findings
DEI-SR DEI-PR Reflectivity Pathologic Feature_n_ Mean SD_n_ Mean SD_P_ 333 Benign 17 1.84 0.35 9 1.94 0.74 .8294 Atypical 9 1.87 0.43 6 2.03 0.51 .4367 Malignant 11 1.94 0.47 7 1.88 0.48 .5465 111 Benign 18 2.05 0.38 4 1.46 0.25 .0003 Atypical 6 2.06 0.69 4 2.03 0.37 .9061 Malignant 18 2.92 0.89 — — — —
DEI, Diffraction-enhanced imaging; DEI-PR, prototype DEI; DEI-SR, synchrotron-based DEI; SD, standard deviation.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
References
1. Chapman D., Thomlinson W., Johnston R.E., et. al.: Diffraction-enhanced x-ray imaging. Phys Med Biol 1997; 42: pp. 2015-2025.
2. Cloetens P., Ludwig W., Baruchel J., et. al.: Holotomography: quantitative phase tomography with micrometer resolution using hard synchrotron radiation x rays. Appl Phys Lett 1999; 75: pp. 2912-2914.
3. Ingal V.N., Beliaevskaya E.A.: X-ray plane-wave topography observation of the phase-contrast from a non-crystalline object. J Phys D Appl Phys 1995; 28: pp. 2314-2317.
4. Pagot E., Fiedler S., Cloetens P., et. al.: Quantitative comparison between two phase-contrast techniques: diffraction-enhanced imaging and phase propagation imaging. Phys Med Biol 2005; 50: pp. 709-724.
5. Peele A.G., De Carlo F., McMahon P.J., et. al.: X-ray phase-contrast tomography with a bending magnet source. Rev Sci Instrum 2005; 76: pp. 083707.1-083707.5.
6. Pfeiffer F., Kottler C., Bunk O., David C.: Hard x-ray phase tomography with low-brilliance sources. Phys Rev Lett 2007; 98: pp. 1081051-1081054.
7. Tanaka T., Honda C., Matsuo S., et. al.: The first trial of phase-contrast imaging for digital full-field mammography using a practical molybdenum x-ray tube. Invest Radiol 2005; 40: pp. 385-396.
8. Weitkamp T., Diaz A., David C., et. al.: X-ray phase imaging with a grating interferometer. Opt Express 2005; 12: pp. 6296-6304.
9. Wu X., Liu H.: Clinical implementation of x-ray phase-contrast imaging: theoretical foundations and design considerations. Med Phys 2003; 30: pp. 2169-2179.
10. Chapman D., Thomlinson W., Arfelli F., et. al.: Mammography imaging studies using a Laue crystal analyzer. Rev Sci Instrum 1996; 67: pp. 1-5.
11. Hasnah M.O., Zhong Z., Oltulu O., et. al.: Diffraction-enhanced imaging contrast mechanisms in breast cancer specimens. Med Phys 2002; 29: pp. 2216-2221.
12. Chapman D., Pisano E., Thomlinson W., et. al.: Medical applications of diffraction-enhanced imaging. Breast Dis 1998; 10: pp. 197-207.
13. Fernandez M., Keyriläinen J., Serimaa R., et. al.: Human breast cancer in vitro: matching histo-pathology with small-angle x-ray scattering and diffraction-enhanced x-ray imaging. Phys Med Biol 2005; 50: pp. 2991-3006.
14. Fiedler S., Bravin A., Keyriläinen J., et. al.: Imaging lobular breast carcinoma: comparison of synchrotron radiation DEI-CT technique with clinical CT, mammography and histology. Phys Med Biol 2004; 49: pp. 175-188.
15. Kiss M.Z., Sayers D.E., Zhong Z.: Measurement of image contrast using diffraction-enhanced imaging. Phys Med Biol 2003; 48: pp. 325-340.
16. Kiss M.Z., Sayers D.E., Zhong Z., et. al.: Improved image contrast of calcifications in breast tissue specimens using diffraction-enhanced imaging. Phys Med Biol 2004; 49: pp. 3427-3439.
17. Lewis R.A., Hall C.J., Hufton A.P., et. al.: X-ray refraction effects: applications to the imaging of biological tissues. Br J Radiol 2003; 76: pp. 301-308.
18. Liu C., Yan X., Zhang X., et. al.: Evaluation of x-ray diffraction-enhanced imaging in the diagnosis of breast cancer. Phys Med Biol 2007; 52: pp. 419-427.
19. Pisano E.D., Johnson R.E., Chapman D., et. al.: Human breast cancer specimens: diffraction-enhanced imaging with histologic correlation-improved conspicuity of lesion detail compared to digital radiography. Radiology 2000; 214: pp. 895-901.
20. Bushberg J., Seibert A., Leidholdt M., Boone J.: The essential physics of medical imaging.2nd ed2002.Lippincott, Williams & WilkinsPhiladelphia, PA
21. Donnelly E.F., Price R.R.: Quantification of the effect of kvp on edge-enhancement index in phase-contrast radiography. Med Phys 2002; 29: pp. 999-1002.
22. Forster E., Goetz K., Zaumseil P.: Double crystal diffractometry for the characterization of targets for laser fusion experiments. Krist Tech 1980; 15: pp. 937-945.
23. Ingal V.N., Beliavskaya E.A., Brianskaya A.P., Merkurieva R.D.: Phase mammography—a new technique for breast investigation. Phys Med Biol 1998; 43: pp. 2555-2567.
24. Kim C.H.: A study of monochromatic x-ray area beam for application in diffraction-enhanced imaging. [dissertation]2007.North Carolina State UniversityRaleigh
25. Vine D.J., Paganin D.M., Pavlov K.M., et. al.: Analyzer-based phase-contrast imaging and phase retrieval using a rotating anode x-ray source. Appl Phys Lett 2007; 91: pp. 254110.
26. Wang X.: Line x-ray source for diffraction-enhanced imaging in clinical and industrial applications. [dissertation]2006.North Carolina State UniversityRaleigh
27. Parham C.A.: System parameters and performance specifications for the application of diffraction-enhanced imaging and multiple image radiography to breast imaging. [dissertation]2006.University of North Carolina at Chapel HillChapel Hill
28. Parham C., Connor D.M., Pisano E.D., et. al.: Design and implementation of a compact low-dose diffraction-enhanced medical imaging system. Acad Radiol 2009; 16: pp. 911-917.
29. Zhong Z., Thomlinson W., Chapman D., Sayers D.: Implementation of diffraction-enhanced imaging experiments: at the NSLS and APS. Nucl Instr Meth A 2000; 450: pp. 556-567.
30. Bravin A., Keyriläinen J., Fernández M., et. al.: High-resolution CT by diffraction-enhanced x-ray imaging: mapping of breast tissue samples and comparison with their histo-pathology. Phys Med Biol 2007; 52: pp. 2197-2211.
31. Keyriläinen J., Fernandez M., Fiedler S., et. al.: Visualization of calcifications and thin collagen strands in human breast tumour specimens by diffraction-enhanced imaging technique: a comparison with conventional mammography and histology. Eur J Radiol 2005; 53: pp. 226-237.