
Rationale and Objectives
The aim of this study was to examine radiologists’ use and perceptions of computer-aided detection (CAD) and double reading for screening mammography interpretation.
Materials and Methods
A mailed survey of 257 community radiologists participating in the national Breast Cancer Surveillance Consortium was used to assess perceptions and practices related to CAD and double reading. Latent class analysis was used to classify radiologists’ overall perceptions of CAD and double reading on the basis of their agreement or disagreement with specific statements about CAD and double reading.
Results
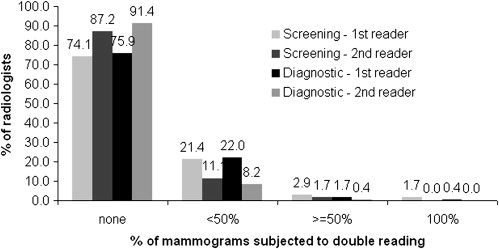
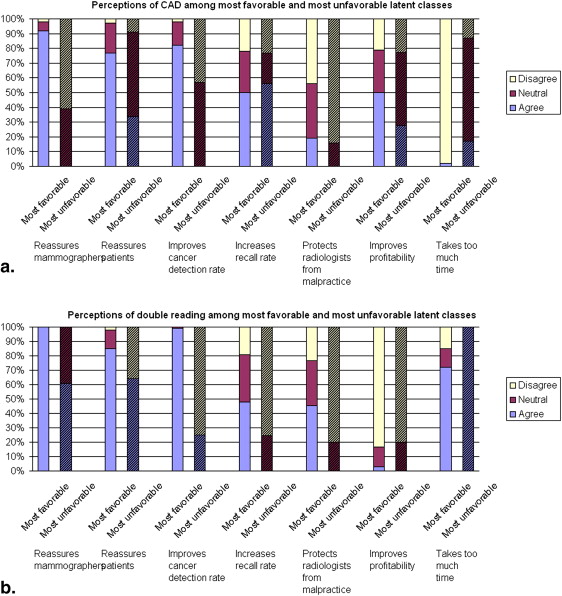
Most radiologists (64%) reported using CAD for more than half the screening mammograms they interpreted, but only <5% reported double reading that much. More radiologists perceived that double reading improved cancer detection rates compared to CAD (74% vs 55% reported), whereas fewer radiologists thought that double reading decreased recall rates compared to CAD (50% vs 65% reported). Radiologists with the most favorable perceptions of CAD were more likely to think that CAD improved cancer detection rates without taking too much time compared to radiologists with the most unfavorable overall perceptions. In latent class analysis, an overall favorable perception of CAD was significantly associated with the use of CAD (81%), a higher percentage of workload in screening mammography (80%), academic affiliation (71%), and fellowship training (58%). Perceptions of double reading that were most favorable were associated with academic affiliation (98%).
Conclusions
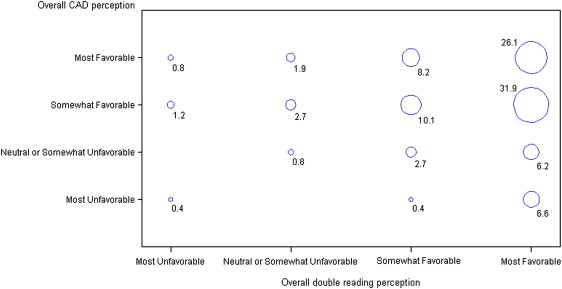
Radiologists’ perceptions were more favorable toward double reading by a second clinician than by a computer, although fewer used double reading in their own practice. The majority of radiologists perceived both CAD and double reading at least somewhat favorably, although for largely different reasons.
We have entered a unique period in medicine in which double reading by a computer may soon replace double reading by a second clinician. This is especially prominent in the field of breast imaging. Computer-aided detection (CAD) has been approved by the US Food and Drug Administration for use in screening mammography interpretation since 1998 with the goal of serving as the equivalent of a “spell checker” to mark potentially abnormal findings and thus lead to improved breast cancer detection . Since that time, the diffusion of CAD in clinical practice has progressed . The use of CAD for screening mammography interpretation has been given some positive anecdotal attention from the commercial media and may have increased patient expectations of accurate cancer detection. However, information on the relative benefits and harms of CAD in mammography is limited and often contradictory. CAD has been shown to increase rates of recall and lower specificity in some studies and to improve sensitivity and cancer detection rates in others .
Double reading is generally accepted as a practice to improve cancer detection in screening mammography, but this is primarily done in Europe and is therefore included in the “European Guidelines for Quality Assurance in Breast Cancer Screening and Diagnosis” . Double reading is not consistently practiced in the United States, possibly because it demands more radiologist time without reimbursement for the second read. Furthermore, the benefits of double reading depend on how the information from the second radiologist is obtained and used (eg, whether the second assessment is independent and blinded to that of the first assessment and whether the final medical decision making requires consensus between the two radiologists for recall).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Data Source and Study Population
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Characteristics of Radiologists Responding to Perception Statements About CAD and Double Reading
Radiologists Who Use CAD for Screening Mammography Radiologists Who Double Read Screening Mammograms Radiologists Who Use CAD for Screening but Not Double Reading All Radiologists Characteristic ( n = 195) ( n = 68) ( n = 121) ( n = 257) Demographics Sex Male 145 (74.4%) 41 (60.3%) 92 (76.0%) 184 (71.6%) Female 50 (24.6%) 27 (39.7%) 29 (24.0%) 73 (28.4%) Age (y) <44 50 (26.0%) 18 (27.3%) 30 (25.2%) 64 (25.4%) 45–54 71 (36.0%) 29 (43.9%) 43 (36.1%) 89 (35.3%) ≥55 71 (36.0%) 19 (28.8%) 46 (38.7%) 99 (39.3%) Practice type Primary affiliation with academic medical center No 158 (82.3%) 54 (79.4%) 100 (84.0%) 208 (81.9%) Adjunct 20 (10.4%) 7 (10.3%) 14 (11.8%) 24 (9.5%) Primary 14 (7.3%) 7 (10.3%) 5 (4.2%) 22 (8.7%) Breast imaging experience Fellowship training No 178 (91.3%) 65 (95.6%) 108 (89.3%) 236 (91.8%) Yes 17 (8.7%) 3 (4.4%) 13 (10.7%) 21 (8.2%) Years of mammography interpretation <10 42 (21.5%) 16 (23.5%) 27 (22.3%) 56 (21.9%) 10–19 73 (37.4%) 24 (35.3%) 44 (36.4%) 91 (35.6%) ≥20 80 (41.0%) 28 (41.2%) 50 (41.3%) 109 (42.6%) Percentage of time spent in breast imaging <20% 49 (25.9%) 13 (19.4%) 32 (27.6%) 66 (26.4%) 20%–39% 45 (23.8%) 18 (26.9%) 29 (25.0%) 66 (26.4%) 40%–79% 26 (13.8%) 16 (23.9%) 9 (7.8%) 38 (15.2%) 80%–100% 69 (36.5%) 20 (29.9%) 46 (39.7%) 80 (32.0%) Volume Self-reported average number of screening mammograms per year over the past 5 years ≤1000 21 (11.4%) 13 (19.4%) 15 (12.7%) 34 (14.0%) 1001–2000 67 (36.4%) 18 (26.9%) 43 (36.4%) 84 (34.6%) ≥2000 96 (52.2%) 36 (53.7%) 60 (50.9%) 125 (51.4%) Percentage of workload that is screening ≤10% 80 (42.3%) 22 (32.4%) 51 (44.0%) 103 (41.0%) 11%–24% 64 (33.9%) 26 (38.2%) 40 (34.5%) 89 (35.5%) ≥25% 45 (23.8%) 20 (29.4%) 25 (21.6%) 59 (23.5%) Interpretative practice CAD use for screening mammography Yes 195 (100.0%) 45 (67.2%) 121 (100.0%) 195 (77.4%) No 0 22 (32.8%) 0 57 (22.6%) CAD use for diagnostic mammography Yes 129 (69.0%) 33 (50.0%) 79 (68.1%) 129 (52.9%) No 58 (31.0%) 33 (50.0%) 37 (31.9%) 115 (47.1%) Double read screening mammograms Yes 45 (24.6%) 68 (100.0%) 0 68 (28.0%) No 138 (75.4%) 0 121 (100.0%) 175 (72.0%) Double read diagnostic mammograms Yes 38 (21.8%) 49 (74.2%) 0 59 (25.4%) No 136 (78.2%) 17 (25.8%) 121 (100.0%) 173 (74.6%)
CAD, computer-aided detection.

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Perceptions of CAD and Double Reading Among 257 Radiologists Surveyed Nationally
Perceptions of CAD Perceptions of Double Reading Perception Statement Agree Neutral Disagree Agree Neutral Disagree Reassures mammographers 163 (64.7%) 65 (25.8%) 24 (9.5%) 191 (80.9%) 35 (14.8%) 10 (4.2%) Reassures patients 185 (74.0%) 60 (24.0%) 5 (2.0%) 172 (73.2%) 53 (22.6%) 10 (4.3%) Improves cancer detection rate 137 (54.6%) 99 (39.4%) 15 (6.0%) 173 (73.9%) 57 (24.4%) 4 (1.7%) Increases recall rate 160 (65.0%) 59 (23.6%) 31 (12.4%) 117 (49.8%) 81 (34.5%) 37 (15.7%) Protects radiologists from malpractice suits 29 (11.6%) 87 (34.7%) 135 (53.8%) 84 (35.6%) 84 (35.6%) 68 (28.8%) Improves profitability of breast imaging 109 (43.8%) 86 (34.5%) 54 (21.7%) 4 (1.7%) 46 (19.6%) 185 (78.7%) Takes too much time 40 (15.9%) 74 (29.5%) 137 (54.6%) 166 (70.6%) 38 (16.2%) 31 (13.2%)
CAD, computer-aided detection.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Prevalence of Latent Class Memberships of Radiologists’ Perceptions of CAD and Double Reading by Radiologist Characteristics
CAD Perception1 (Row %) Double Reading Perception (Row %) Radiologist Characteristic Most Favorable Somewhat Favorable Neutral or Somewhat Unfavorable Most Unfavorable Most Favorable Somewhat Favorable Neutral or Somewhat Unfavorable Most Unfavorable Total 35.8 43.3 12.0 9.0 64.5 28.2 5.1 2.3 Demographics Sex Male 42.9 39.2 9.6 8.3 60.1 31.4 6.0 2.5 Female 24.1 46.5 19.0 10.4 79.2 16.2 2.8 1.8 Age (y) <44 31.2 52.0 14.5 2.3 68.6 21.4 8.2 1.8 45–54 40.4 32.5 14.3 12.8 58.2 34.1 3.6 4.1 ≥55 35.6 47.0 7.2 10.2 69.2 25.1 4.5 1.2 Practice type Primary affiliation with academic medical center No 35.8 ∗ 43.2 ∗ 10.6 ∗ 10.4 ∗ 59.4 ∗ 32.1 ∗ 6.2 ∗ 2.3 ∗ Adjunct 70.0 ∗ 9.5 ∗ 15.5 ∗ 5.0 ∗ 68.7 ∗ 26.5 ∗ 0.2 ∗ 4.6 ∗ Primary 16.7 ∗ 53.9 ∗ 24.2 ∗ 5.2 ∗ 98.0 ∗ 1.7 ∗ 0.2 ∗ 0.1 ∗ Breast imaging experience Fellowship training No 38.1 ∗ 44.1 ∗ 7.7 ∗ 10.1 ∗ 66.0 26.0 5.6 2.4 Yes 18.3 ∗ 39.5 ∗ 41.7 ∗ 0.5 ∗ 60.9 38.8 0.2 0.1 Years of mammography interpretation <10 31.5 44.5 18.9 5.1 69.6 22.8 5.6 2.0 10–19 46.5 33.9 8.0 11.6 60.6 32.0 4.7 2.7 ≥20 32.6 46.3 11.6 9.5 65.5 28.2 4.2 2.1 Percentage of time spent in breast imaging <20% 31.9 39.7 11.7 16.7 61.8 33.3 4.9 0.0 20%–39% 33.7 54.2 7.0 5.1 70.5 21.6 6.3 1.6 40%–79% 45.9 28.8 16.7 8.6 62.1 29.3 2.9 5.7 80%–100% 33.5 41.6 17.9 7.0 65.0 25.7 5.8 3.5 Volume Self-reported average number of mammograms per year over the past 5 years ≤1000 37.7 34.3 17.2 10.8 70.1 23.5 3.1 3.3 1001–2000 39.1 43.8 8.0 9.1 73.6 16.9 8.0 1.5 ≥2000 37.9 40.5 13.9 7.7 65.8 28.1 3.3 2.8 Percentage of workload that is screening ≤10% 36.3 ∗ 37.7 ∗ 8.8 ∗ 17.2 ∗ 63.8 30.9 4.2 1.1 11%–24% 40.8 ∗ 39.8 ∗ 14.4 ∗ 5.0 ∗ 67.7 24.3 3.7 4.3 ≥25% 23.2 ∗ 57.1 ∗ 14.3 ∗ 5.4 ∗ 69.1 19.8 9.1 2.0 Interpretative practice CAD use for Screening: yes 59.9 ∗ 21.5 ∗ 10.0 ∗ 8.6 ∗ 64.4 27.7 5.6 2.3 Screening: no 12.2 ∗ 71.7 ∗ 13.8 ∗ 2.3 ∗ 64.7 31.6 3.7 0.0 Diagnosis: yes 53.3 ∗ 24.8 ∗ 11.3 ∗ 10.6 ∗ 62.1 32.2 4.1 1.6 Diagnosis: no 24.4 ∗ 59.3 ∗ 9.7 ∗ 6.6 ∗ 64.9 27.4 5.6 2.1 Double reader Screening: yes 38.8 39.7 15.1 6.4 82.6 9.8 4.5 3.1 Screening: no 42.1 37.3 6.9 13.7 63.2 29.2 5.6 2.0 Diagnosis: yes 37.9 38.5 17.5 6.1 81.6 11.1 3.6 3.7 Diagnosis: no 38.0 42.7 8.4 10.9 65.3 27.9 4.8 2.0
CAD, computer-aided detection.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Birdwell R.L., Bandodkar P., Ikeda D.M.: Computer-aided detection with screening mammography in a university hospital setting. Radiology 2005; 236: pp. 451-457.
2. National Cancer Institute. Computer-aided interpretation of mammograms: questions and answers. Available at: http://www.cancer.gov/newscenter/pressreleases/CADmammographyQandA . Accessed July 2009.
3. Taylor P., Potts H.W.: Computer aids and human second reading as interventions in screening mammography: two systematic reviews to compare effects on cancer detection and recall rate. Eur J Cancer 2008; 44: pp. 798-807.
4. Freer T.W., Ulissey M.J.: Screening mammography with computer-aided detection: prospective study of 12,860 patients in a community breast center. Radiology 2001; 220: pp. 781-782.
5. Houssami N., Given-Wilson R., Ciatto S.: Early detection of breast cancer: overview of the evidence on computer-aided detection in mammography screening. J Med Imaging Radiat Oncol 2009; 53: pp. 171-172.
6. Morton M.J., Whaley D.H., Brandt K.R., Amrami K.K.: Screening mammograms: interpretation with computer-aided detection—prospective evaluation. Radiology 2006; 239: pp. 375-383.
7. Beam C., Hendrick R.: Proposition: all mammograms should be double-read. Med Phys 1999; 26: pp. 115-118.
8. Anttinen I., Pamilo M., Soiva M., Roiha M.: Double reading of mammography screening films—one radiologist or two?. Clin Radiol 1993; 48: pp. 414-421.
9. Destounis S.V., DiNitto P., Logan-Young W., Bonaccio E., Zuley M.L., Willison K.M.: Can computer-aided detection with double reading of screening mammograms help decrease the false-negative rate? Initial experience. Radiology 2004; 232: pp. 578-584.
10. Harvey S.C., Geller B., Oppenheimer R.G., Pinet M., Riddell L., Garra B.: Increase in cancer detection and recall rates with independent double interpretation of screening mammography. AJR Am J Roentgenol 2003; 180: pp. 1461-1462.
11. Blanks R.G., Wallis M.G., Moss S.M.: A comparison of cancer detection rates achieved by breast cancer screening programmes by number of readers, for one and two view mammography: results from the UK National Health Service breast screening programme. J Med Screen 1998; 5: pp. 195-201.
12. Thurfjell E.L., Lernevall K.A., Taube A.A.S.: Benefit of independent double reading in a population-based mammography screening program. Radiology 1994; 191: pp. 241-244.
13. Brown J., Bryan S., Warren R.: Mammography screening: an incremental cost effectiveness analysis of double versus single reading of mammograms. BMJ 1996; 312: pp. 809-822.
14. Perry N, Broeders M, Wolf CD, et al, eds. European guidelines for quality assurance in breast cancer screening and diagnosis. 4th ed. Available at: http://ec.europa.eu/health/ph_projects/2002/cancer/fp_cancer_2002_ext_guid_01.pdf . Accessed July 2009.
15. Gilbert F.J., Astley S.M., Gillan M.G., et. al.: Single reading with computer-aided detection for screening mammography. N Engl J Med 2008; 359: pp. 1675-1684.
16. Hofvind S., Vacek P.M., Skelly J., Weaver D.L., Geller B.M.: Comparing screening mammography for early breast cancer detection in Vermont and Norway. J Natl Cancer Inst 2008; 100: pp. 1082-1091.
17. Breast Cancer Surveillance Consortium. Home page. Available at: http://breastscreening.cancer.gov . Accessed October 5, 2009.
18. Ballard-Barbarsh R., Taplin S.H., Yankaskas B.C., et. al.: Breast Cancer Surveillance Consortium: a national mammography screening and outcomes database. AJR Am J Roentgenol 1997; 169: pp. 1001-1008.
19. Carney P.A., Geller B.M., Moffett H., et. al.: Current medicolegal and confidentiality issues in large, multicenter research programs. Am J Epidemiol 2000; 152: pp. 371-378.
20. Bandeen-Roche K., Zeger S.L., Rathouz P.J.: Latent variable regression for multiple discrete outcomes. J Am Stat Assoc 1997; 92: pp. 1375-1386.
21. Lazersfeld P.F.: Latent Structure Analysis.1968.Houghton MifflinBoston
22. Ciatto S., Del Turco M.R., Morrone D., et. al.: Independent double reading of screening mammograms. J Med Screen 1995; 2: pp. 99-101.
23. Physician Insurers Association of America: Breast Cancer Study.Third Edition2002.Physician Insurers Association of AmericaRockville, MD
24. Fenton J.J., Taplin S.H., Carney P.A., et. al.: Influence of computer-aided detection on performance of screening mammography. N Engl J Med 2007; 356: pp. 1399-1409.
25. Gilbert F.J., Astely S.M., McGee M.A., et. al.: Single reading with computer-aided detection and double reading of screening mammograms in the United Kingdom National Breast Screening Program. Radiology 2006; 241: pp. 47-53.
26. Hendrick R.E., Cutter G.R., Berns E.A., et. al.: Community-based mammography practice: services, charges, and interpretation methods. AJR Am J Roentgenol 2005; 184: pp. 433-438.