
Rationale and Objectives
In this article, we review the core principles of bone physiology alongside imaging examples that demonstrate such principles.
Materials and Methods
The core principles of bone physiology are reviewed and further solidified with a corresponding abnormal pathophysiologic example. The key principles of bone physiology to be reviewed include the following: (1) formation and growth, (2) maintenance and repair, (3) metabolism and regulation, and (4) neoplastic disease. Lastly, a collection of secondary bone diseases is presented to demonstrate the skeletal manifestations of numerous systemic diseases. With this integrative method, we hope to emphasize the value of using radiology to teach physiology within a clinical context. This is especially relevant now, as many US medical schools undergo curricular reform with more emphasis on integrative interdisciplinary learning. Ultimately, we intend to provide a paradigm for incorporating radiology into the pre-clinical medical curriculum through a review of basic science physiology that underlies key radiographic findings of the skeletal system.
Results
Radiology is known for its role in helping make diagnoses and clinical decisions. However, radiology is also well suited to enhance medical education by offering the ability to visualize physiology in action. This is especially true in skeletal radiology, where radiographic osseous changes represent a wide range of physiological processes. Therefore, skeletal radiology can be a useful tool for illustrating concepts of physiology that underlie the normal and abnormal radiologic appearances of bone.
Conclusion
Radiology is an important but underutilized tool for demonstrating concepts in bone physiology.
Introduction and Background
One of the greatest underappreciated opportunities in medical education is the use of radiologic images to teach the basic medical sciences. Too often, medical students learn such subjects as anatomy, physiology, and pathology from text, diagrams, cadavers, and animal models rather than from living human subjects. Radiology makes it possible to visualize living human structure, function, disease, and injury in ways that can help learners gain a much deeper understanding of the material, creating indelible images that they carry with them into practice for many years. Nonetheless, radiology is underutilized in this regard.
Despite the explosion of diagnostic imaging utilization in clinical practice, estimated to be nearly twice the rate of laboratory and pharmaceutical usage , the role of radiology in medical education has remained stagnant across allopathic and osteopathic medical schools for decades . If available, a formal radiology clerkship is typically offered to medical students as a fourth-year elective, long after the basic science coursework has ended. This approach isolates radiology fromits foundation in the basic sciences and may put students at a disadvantage in their future clinical practices.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
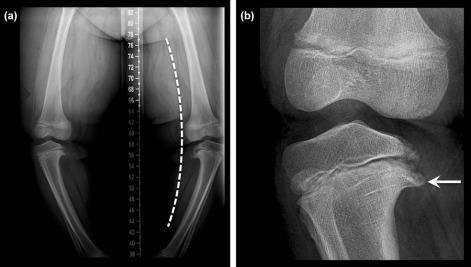
Bone Development and Growth
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
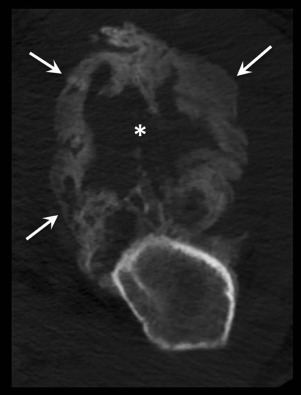
Bone Maintenance and Repair
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
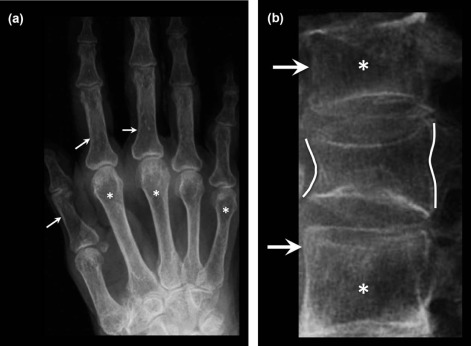
Bone Metabolism and Regulation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Neoplastic Disease
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Secondary Disorders of Bone
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. Hendee W.R., Becker G.J., Borgstede J.P., et. al.: Addressing overutilization in medical imaging. Radiology 2010; 257: pp. 240-245.
2. Poot J.D., Hartman M.S., Daffner R.H.: Understanding the US medical school requirements and medical students’ attitudes about radiology rotations. Acad Radiol 2012; 19: pp. 369-373.
3. Phillips A.W., Smith S.G., Straus C.M.: The role of radiology in preclinical anatomy: a critical review of the past, present, and future. Educ Issue 2013; 20: pp. 297-304. e1
4. Bassett L.W., Squire L.F.: Anatomy instruction by radiologists. Invest Radiol 1985; 20: pp. 1008-1010.
5. Tufts M.A., Higgins-Opitz S.B.: What makes the learning of physiology in a PBL medical curriculum challenging? Student perceptions. Adv Physiol Educ 2009; 33: pp. 187-195.
6. Sefton A.J.: Charting a global future for education in physiology. Adv Physiol Educ 2005; 29: pp. 189-193.
7. Michael J.A., Richardson D., Rovick A., et. al.: Undergraduate students’ misconceptions about respiratory physiology. Am J Physiol 1999; 277: pp. S127-S135.
8. Nay J.W., Aaron V.D., Gunderman R.B.: Using radiology to teach physiology. J Am Coll Radiol 2011; 8: pp. 117-123.
9. Finnerty E.P., Chauvin S., Bonaminio G., et. al.: Flexner revisited: the role and value of the basic sciences in medical education. Acad Med 2010; 85: pp. 349-355.
10. Eisenstein A., Vaisman L., Johnston-Cox H., et. al.: Integration of basic science and clinical medicine: the innovative approach of the cadaver biopsy project at the Boston University School of Medicine. Acad Med 2014; 89: pp. 50-53.
11. Bell F.E., Wilson L.B., Hoppmann R.A.: Using ultrasound to teach medical students cardiac physiology. Adv Physiol Educ 2015; 39: pp. 392-396.
12. Boffano P., Roccia F., Campisi P., et. al.: Review of 43 osteomas of the craniomaxillofacial region. J Oral Maxillofac Surg 2012; 70: pp. 1093-1095.
13. Laor T., Jaramillo D.: MR imaging insights into skeletal maturation: what is normal?. Radiology 2009; 250: pp. 28-38.
14. Marco R.A., Gitelis S., Brebach G.T., et. al.: Cartilage tumors: evaluation and treatment. J Am Acad Orthop Surg 2000; 8: pp. 292-304.
15. Birch J.G.: Blount disease. J Am Acad Orthop Surg 2013; 21: pp. 408-418.
16. Sabharwal S.: Blount disease. J Bone Joint Surg Am 2009; 91: pp. 1758-1776.
17. Walczak B.E., Johnson C.N., Howe B.M.: Myositis ossificans. J Am Acad Orthop Surg 2015; 23: pp. 612-622.
18. Andersen T.L., Sondergaard T.E., Skorzynska K.E., et. al.: A physical mechanism for coupling bone resorption and formation in adult human bone. Am J Pathol 2009; 174: pp. 239-247.
19. Parfitt A.M.: Misconceptions (2): turnover is always higher in cancellous than in cortical bone. Bone 2002; 30: pp. 807-809.
20. Raisz L.G.: Physiology and pathophysiology of bone remodeling. Clin Chem 1999; 45: pp. 1353-1358.
21. Hadjidakis D.J., Androulakis I.I.: Bone remodeling. Ann N Y Acad Sci 2006; 1092: pp. 385-396.
22. Chen J.-H., Liu C., You L., et. al.: Boning up on Wolff’s law: mechanical regulation of the cells that make and maintain bone. J Biomech 2010; 43: pp. 108-118.
23. Del Fattore A., Teti A., Rucci N.: Bone cells and the mechanisms of bone remodelling. Front Biosci (Elite Ed) 2012; 4: pp. 2302-2321.
24. Mee A.P., Dixon J.A., Hoyland J.A., et. al.: Detection of canine distemper virus in 100% of Paget’s disease samples by in situ-reverse transcriptase-polymerase chain reaction. Bone 1998; 23: pp. 171-175.
25. Schindeler A., McDonald M.M., Bokko P., et. al.: Bone remodeling during fracture repair: the cellular picture. Semin Cell Dev Biol 2008; 19: pp. 459-466.
26. Gaston M.S., Simpson A.H.R.W.: Inhibition of fracture healing. J Bone Joint Surg Br 2007; 89-B: pp. 1553-1560.
27. Forslund J.M., Archdeacon M.T.: The pathobiology of diabetes mellitus in bone metabolism, fracture healing, and complications. Am J Orthop (Belle Mead NJ) 2015; 44: pp. 453-457.
28. Gullihorn L., Karpman R., Lippiello L.: Differential effects of nicotine and smoke condensate on bone cell metabolic activity. J Orthop Trauma 2005; 19: pp. 17-22.
29. Raikin S.M., Landsman J.C., Alexander V.A., et. al.: Effect of nicotine on the rate and strength of long bone fracture healing. Clin Orthop 1998; pp. 231-237.
30. Giannoudis P.V., MacDonald D.A., Matthews S.J., et. al.: Nonunion of the femoral diaphysis: The influence of reaming and non-steroidal anti-inflammatory drugs. J Bone Joint Surg Br 2000; 82-B: pp. 655-658.
31. Kumar V., Stanley L.: Robbins basic pathology.8th ed.2007.Saunders/Elsevier.
32. Marx S.J.: Hyperparathyroid and hypoparathyroid disorders. N Engl J Med 2000; 343: pp. 1863-1875.
33. Genant H.K., Heck L.L., Lanzl L.H., et. al.: Primary hyperparathyroidism. A comprehensive study of clinical, biochemical and radiographic manifestations. Radiology 1973; 109: pp. 513-524.
34. Jevtic V.: Imaging of renal osteodystrophy. Eur J Radiol 2003; 46: pp. 85-95.
35. Lips P.: Vitamin D physiology. Prog Biophys Mol Biol 2006; 92: pp. 4-8.
36. Pacifici R.: Cytokines, estrogen, and postmenopausal osteoporosis – the second decade. Endocrinology 1998; 139: pp. 2659-2661.
37. Wodajo F.M., Gannon F., Murphey M.D.: Visual guide to musculoskeletal tumors: a clinical-radiologic-histologic approach.2010.Elsevier Health Sciences
38. Rana R.S., Wu J.S., Eisenberg R.L.: Periosteal reaction. AJR Am J Roentgenol 2009; 193: pp. W259-W272.
39. Clines G.A., Guise T.A.: Hypercalcaemia of malignancy and basic research on mechanisms responsible for osteolytic and osteoblastic metastasis to bone. Endocr Relat Cancer 2005; 12: pp. 549-583.
40. Keller E.T., Brown J.: Prostate cancer bone metastases promote both osteolytic and osteoblastic activity. J Cell Biochem 2004; 91: pp. 718-729.
41. Kondo K.L., Swerdlow M.: Medical student radiology curriculum: what skills do residency program directors believe are essential for medical students to attain?. Educ Issue 2013; 20: pp. 263-271.