
Rationale and Objectives
To evaluate the interpretation of computed tomographic pulmonary angiograms performed outside of regular reporting hours, comparing the initial interpretation by the radiology resident to the attending radiologist.
Materials and Methods
Records for 840 consecutive computed tomographic pulmonary angiograms (CTPA) performed outside of regular reporting hours at two tertiary referral centers from January 1, 2004–December 31, 2005 were reviewed. The preliminary interpretation by the on-call radiology resident was compared to the subsequent final report issued by a subspecialty trained chest radiologist. Studies were stratified as positive, negative, or equivocal for pulmonary embolus. Cases with discordant interpretations or negative CTPA were reviewed to determine impact on clinical outcome. Patients were followed up to 12 months after CTPA to document any subsequent thromboembolic event.
Results
Sixteen percent (131/840) of CTPAs were reported positive by the staff radiologist. There was agreement in 90% (752/840) of studies ( P = .76, 95% confidence interval, 0.71–0.81) with 86% (114/133) agreement for studies interpreted as positive by residents, 95% (582/612) for studies interpreted as negative by residents, and 63% (60/95) for studies interpreted as equivocal by residents. Studies of optimal quality had higher interobserver agreement than studies of suboptimal quality ( P < .0001). In-patient studies were more likely to be positive than emergency room patients (20% vs. 13%) ( P = .004). No adverse clinical outcomes were attributed to discordant interpretations.
Conclusions
Radiology residents provide a high level interpretation of on-call CTPA studies, achieving good concordance with the attending radiologists’ assessment.
Acute pulmonary embolism (PE) is estimated to cause 50,000 to 100,000 deaths annually in the United States ( ). It is a potentially treatable condition; therefore, an accurate and early diagnosis is essential. Computed tomographic pulmonary angiography (CTPA) is an important diagnostic tool used to evaluate patients presenting with symptoms suggestive of PE. Given the potential seriousness of a positive diagnosis, these examinations are triaged as high priority scans, and during regular working hours, a staff radiologist will communicate a report to the patient’s physician expeditiously to facilitate appropriate management.
At many academic institutions, CTPA examinations that are performed out of regular clinical hours (“on call”) are initially read by radiology residents, who provide a preliminary interpretation. A staff radiologist subsequently reviews the study. Several studies have demonstrated good concordance between resident and attending interpretations of on-call studies in general ( ), but there have been a limited number of studies examining resident interpretation of CTPA ( ). These studies are limited by a small number of patients and have few resident observers. Moreover, the impact of the initial radiology report on clinical decision-making and patient outcome has not been assessed in these studies. Ginsberg et al. ( ) performed a larger retrospective study with 658 CTPA examinations in which they compared the performance of on-call radiology fellows with that of staff radiologists and reported a good correlation between the two groups. These results cannot easily be extrapolated to most academic institutions in which radiology residents, not fellows, are the primary interpreters of these studies after hours.
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
CT Technique
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Residency Structure and Precall Preparation
Get Radiology Tree app to read full this article<
Interpretation
Get Radiology Tree app to read full this article<
Data Collection and Analysis
Get Radiology Tree app to read full this article<
Table 1
Data Recorded for Each CT Pulmonary Angiogram
Age Sex Date study completed Hospital site (A, B) Patient location (inpatient, emergency department) Time study completed Time resident report entered Rank of resident Resident interpretation Staff interpretation Type of scanner (4-, 8-, 64-row detector)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Agreement
Get Radiology Tree app to read full this article<
Table 2
Summary of Interpretations of 840 CT Pulmonary Angiograms by Radiology Residents and Attending Staff
Resident Interpretation Attending Interpretation Negative (%) Equivocal (%) Positive (%) Negative (%) 582 (69) 19 (2.3) 11 (1.3) Equivocal (%) 29 (3.5) 60 (7) 6 (0.7) Positive (%) 13 (1.5) 6 (0.7) 114 (13.6) Total (%) 624 (74) 85 (10) 131 (15.6)
Get Radiology Tree app to read full this article<
Discordant Results
Get Radiology Tree app to read full this article<
Clinical Outcome for Discordant Cases
Get Radiology Tree app to read full this article<
Table 3
Clinical Outcome in Discordant Interpretations
Type of Discordant Interpretation (Resident/Staff) No. of Patients Anticoagulated/No. of Discordant CT Pulmonary Angiograms Comments Negative/positive 11/11 No complications from delay in AC Positive/negative 2/13 2 short-term AC, discontinued with no complications Negative/equivocal 5/19 2 short-term AC, discontinued with no complications 1 long-term AC as patient clinically high risk for embolism, no complications 2 lifelong AC Positive/equivocal 3/6 1 short-term AC, discontinued with no complications 1 long-term AC as repeat CT 1 day later was positive, no complications 1 lifelong AC Equivocal/positive 6/6 No complications from delay in AC Equivocal/negative 7/29 5 short-term AC, discontinued with no complications 2 lifelong AC
AC, anticoagulation therapy.
Get Radiology Tree app to read full this article<
Clinical Significance of a Negative CTPA Study
Get Radiology Tree app to read full this article<
Follow-up Studies
Get Radiology Tree app to read full this article<
Agreement by Quality
Get Radiology Tree app to read full this article<
Table 4
Factors Limiting the Interpretation of CT Pulmonary Angiograms in 112 Patients
Number of Scans Factor ⁎ N = 112 (%) Poor contrast opacification 54 (48) Respiratory motion 50 (45) Streak artifact 2 (2) Cardiac pulsation artifact 1 (1) Patient motion 1 (1) Atelectasis 1 (1) Not specified 3 (3)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
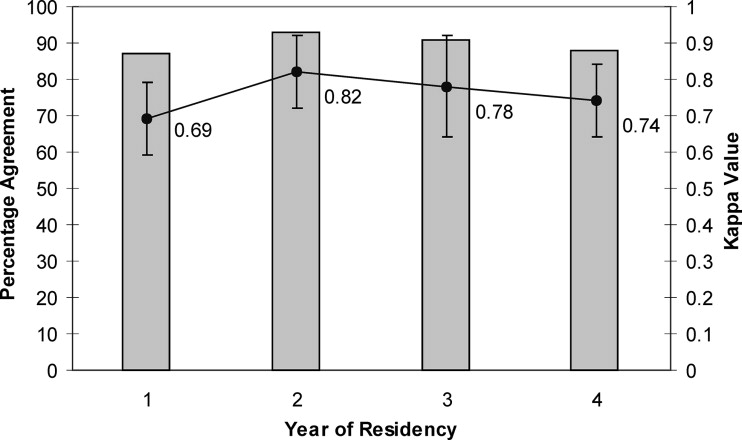
Agreement by Year of Residency
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Agreement by Type of Scanner
Get Radiology Tree app to read full this article<
Likelihood of a Positive Study Based on Patent Location
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Laack T.A., Goyal D.G.: Pulmonary embolism: An unsuspected killer. Emerg Med Clin North Am 2004; 22: pp. 961-983.
2. National Institutes of Health: Prevention of venous thrombosis and pulmonary embolism. JAMA 1986; 256: pp. 744-749.
3. Matsumoto A.H., Tegtmeyer C.J.: Contemporary diagnostic approaches to acute pulmonary emboli. Radiol Clin North Am 1995; 33: pp. 167-183.
4. Albano M.C., Ross G.W., Ditchek J.J., et. al.: Resident interpretation of emergency CT scans in the evaluation of acute appendicitis. Acad Radiol 2001; 8: pp. 915-918.
5. Lal N.R., Murray U.M., Eldevik O.P., et. al.: Clinical consequences of misinterpretations of neuroradiologic CT scans by on-call radiology residents. Am J Neuroradiol 2000; 21: pp. 124-129.
6. Wysoki M.G., Nassar C.J., Koenigsberg R.A., et. al.: Head trauma: CT scan interpretation by radiology residents versus staff radiologists. Radiology 1998; 208: pp. 125-128.
7. Roszler M.H., McCarroll K.A., Rashid T., et. al.: Resident interpretation of emergency computed tomographic scans. Invest Radiol 1991; 26: pp. 374-376.
8. van Rossum A.B., van Erkel A.R., van Persijn van Meerten E.L., et. al.: Accuracy of helical CT for acute pulmonary embolism: ROC analysis of observer performance related to clinical experience. Eur Radiol 1998; 8: pp. 1160-1164.
9. Wechsler R.J., Spettell C.M., Kurtz A.B., et. al.: Effects of training and experience in interpretation of emergency body CT scans. Radiology 1996; 199: pp. 717-720.
10. Eng J., Mysko W.K., Weller G.E., et. al.: Interpretation of emergency department radiographs: A comparison of emergency medicine physicians with radiologists, residents with faculty, and film with digital display. AJR Am J Roentgenol 2000; 175: pp. 1233-1238.
11. Lowe L.H., Draud K.S., Hernanz-Schulman M., et. al.: Nonenhanced limited CT in children suspected of having appendicitis: Prospective comparison of attending and resident interpretations. Radiology 2001; 221: pp. 755-759.
12. Carney E., Kempf J., DeCarvalho V., et. al.: Preliminary interpretations of after-hours CT and sonography by radiology residents versus final interpretations by body imaging radiologists at a level 1 trauma center. AJR Am J Roentgenol 2003; 181: pp. 367-373.
13. Safriel Y., Sclafani S., Gale B., et. al.: Comparing the interpretations of CT pulmonary angiograms by attending and resident radiologists: Can residents identify life-threatening pulmonary emboli in hospitalized patients?. Emerg Radiol 2002; 9: pp. 55-59.
14. Shaham D., Heffez R., Bogot N.R., et. al.: CT pulmonary angiography for the detection of pulmonary embolism: Interobserver agreement between on-call radiology residents and specialists (CTPA interobserver agreement). Clin Imaging 2006; 30: pp. 266-270.
15. Ginsberg M.S., King V., Panicek D.M.: Comparison of interpretations of CT angiograms in the evaluation of suspected pulmonary embolism by on-call radiology fellows and subsequently by radiology faculty. AJR Am J Roentgenol 2004; 182: pp. 61-66.
16. Remy-Jardin M., Remy J.: Spiral CT angiography of the pulmonary circulation. Radiology 1999; 212: pp. 615-636.
17. Altmann D.: Primary Statistics for Medical Research.1992.Chapman & HallLondon, England:pp. 404.
18. Chartrand-Lefebvre C., Howarth N., Lucidarme O., et. al.: Contrast-enhanced helical CT for pulmonary embolism detection: Inter- and intraobserver agreement among radiologists with variable experience. AJR Am J Roentgenol 1999; 172: pp. 107-112.