
Rationale and Objectives
The current paradigm of cancer diagnosis involves uncoordinated communication of findings from radiology and pathology to downstream physicians. Discordance between these findings can require additional time from downstream users to resolve, or given incorrect resolution, may adversely impact treatment decisions. To mitigate this problem, we developed a web-based system, called RadPath, for correlating and integrating radiology and pathology reporting.
Materials and Methods
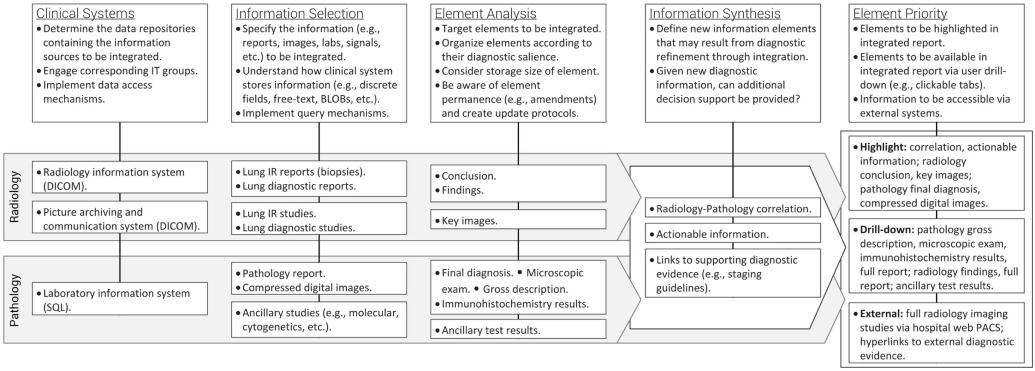
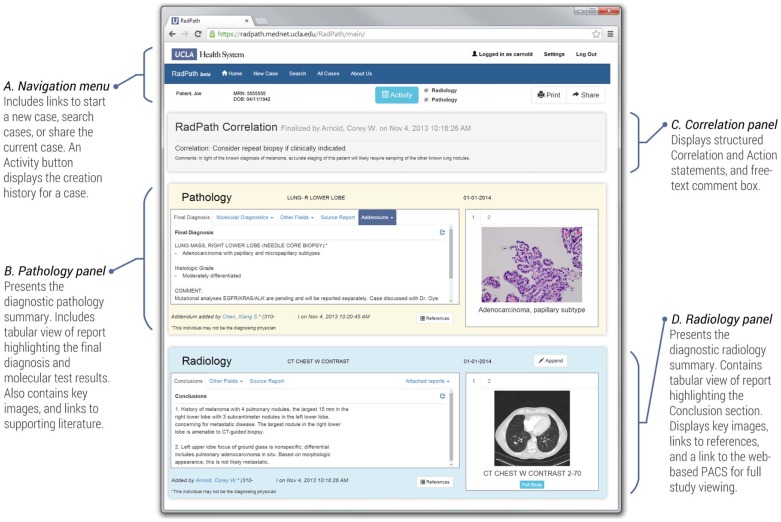
RadPath includes interfaces to our institution’s clinical information systems, which are used to retrieve reports, images, and test results that are structured into an interactive compendium for a diagnostic patient case. The system includes an editing interface for physicians, allowing for the inclusion of additional clinical data, as well as the ability to retrospectively correlate and contextualize imaging findings following pathology diagnosis.
Results
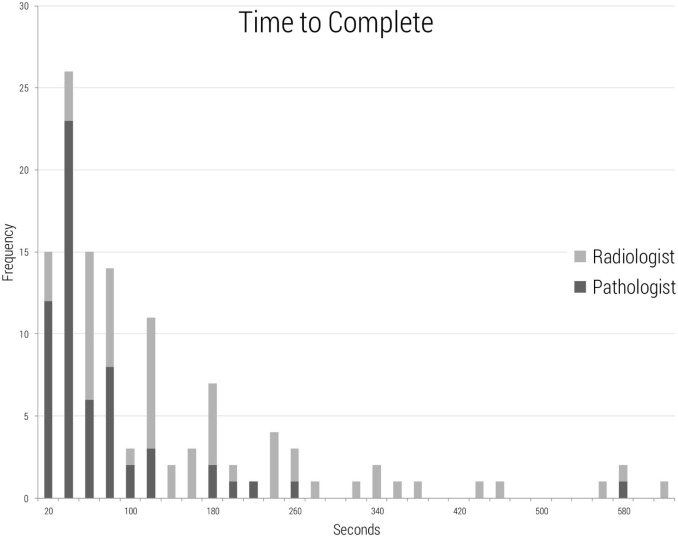
During pilot deployment and testing over the course of 1 year, physicians at our institution have completed 60 RadPath cases, requiring an average of 128 seconds from a radiologist and an average of 93 seconds from a pathologist per case. Several technical and workflow challenges were encountered during development, including interfacing with diverse clinical information systems, automatically structuring report contents, and determining the appropriate physicians to create RadPath summaries. Reaction to RadPath has been positive, with users valuing the system’s ability to consolidate diagnostic information.
Conclusions
With the increasing complexity of medicine and the movement toward team-based disease management, there is a need for improved clinical communication and information exchange. RadPath provides a platform for generating coherent and correlated diagnostic summaries in cancer diagnosis with minimal additional effort from physicians.
Introduction
Cancer is one of the leading causes of death in the United States . Pathology and radiology form the basis of cancer diagnosis, yet the specialties remain isolated, reporting findings independently and often having only minimal communication. The combination of these factors may result in radiologic-pathologic discordance, defined as a discrepancy between imaging and histologic findings . Radiologic-pathologic correlation is utilized in various imaging specialties as a tool to assess the utility of new imaging modalities, to gauge interpretive performance, and to identify radiographic features corresponding to histologic findings . However, correlation in these instances takes place for research or quality assurance purposes, and is generally not a normal part of radiologist or pathologist workflow.
Radiologic-pathologic discordance can be problematic for the ordering clinician, who is left with the task of reconciling the diagnostic conflict . The process of resolution may encompass a spectrum of actions depending on the specific findings, but examples include (1) contacting both the radiologist and the pathologist for clarification of findings; (2) concluding that the computed tomography (CT)-guided biopsy retrieved tissue was not representative of the lesion of concern; or (3) accepting the histologic findings as the final diagnosis and mistakenly interpreting an inadequately sampled lesion as benign. Such actions may lead to a false-negative conclusion in which cases of high radiographic suspicion of malignancy are misdiagnosed as benign, leading to delay in diagnosis with subsequent higher treatment costs and worse clinical outcomes . A recent study found a nearly 20% discordancy rate in mammography biopsies, with over 1.2% resulting in delayed diagnosis of a carcinoma . Extrapolated nationally, this type of discordancy was projected to result in 9969 missed diagnoses of malignant disease. Other studies have found similar results in breast imaging with false-negative rates of image-directed core biopsies estimated to be between 1% and 9% .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
System Architecture
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Report Overview
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Workflow
Get Radiology Tree app to read full this article<
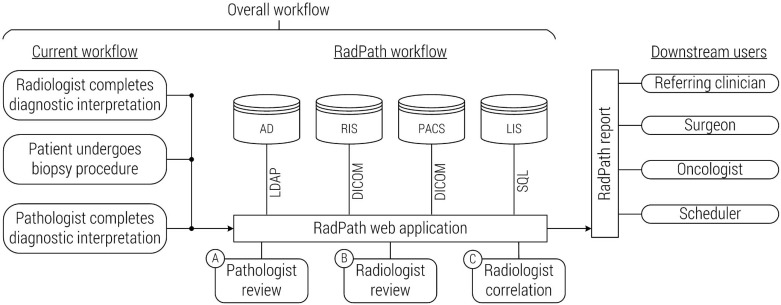
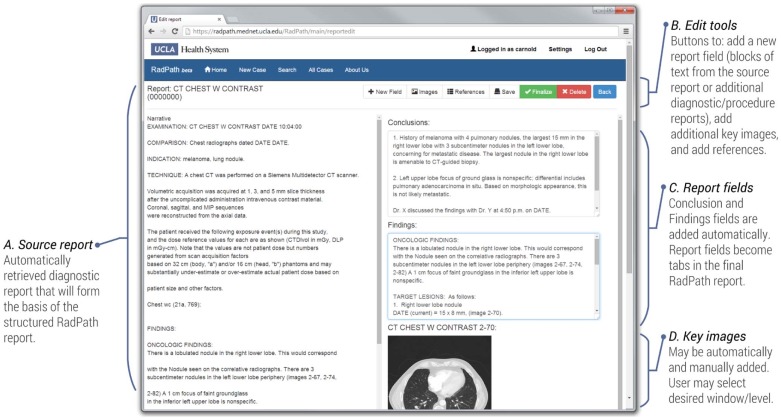
Table 1
Correlation and Action Options, and an Example Correlated Case
Drop-down Text Options Correlation Radiology and pathology correlate.
Defer to pathology diagnosis.
Combined findings suggest sampling error.
Findings are an incomplete representation of disease state. Action No further action needed from radiology and pathology.
Consider repeat biopsy if clinically indicated.
Other: see comments.
Field Example Radiology diagnosis History of melanoma with four pulmonary nodules, the largest 15 mm in the right lower lobe with three subcentimeter nodules in the left lower lobe, concerning for metastatic disease. The largest nodule in the right lower lobe is amenable to CT-guided biopsy. Pathology diagnosis LUNG MASS, RIGHT LOWER LOBE (NEEDLE CORE BIOPSY):
– Adenocarcinoma with papillary and micropapillary subtypes. Correlation Defer to pathology diagnosis. Action Consider repeat biopsy if clinically indicated. Comment In light of the known diagnosis of melanoma, accurate staging of this patient may require sampling of the other known lung nodules.
CT, computed tomography.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Clinician Survey
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 2
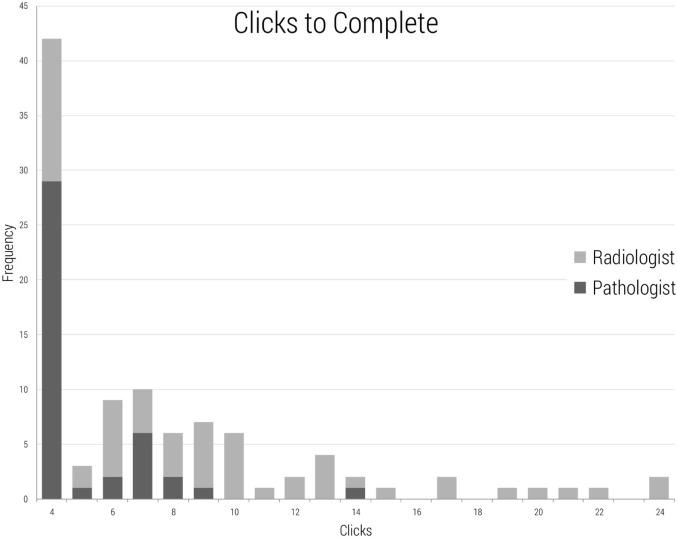
Data Describing RadPath System Usage by Radiologists and Pathologists During Summary Creation
User Average Time (seconds) Median Time (seconds) Average Clicks Radiologist 196 120 9.4 Pathologist 63 35 2.7
Data cover a 12-month period and 60 cases.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Responses to Survey on the Perceived Utility of the RadPath Report ( n = 5)
Question Strongly Disagree Disagree Neutral Agree Strongly Agree There are problems with my current workflow for interpreting diagnostic results from Radiology and Pathology. — — 4 1 — RadPath will be an improvement to my current patient preparation workflow. — — — 2 3 RadPath will reduce my need to search for information in the electronic medical record. — — — 4 1 RadPath will be a valuable educational tool for my patients. — — — 4 1 RadPath will help me stage a disease. — — 2 3 — I will feel comfortable using RadPath as my primary source for diagnostic results for radiology-guided needle biopsy results. — — 1 3 1 I will use the Share function to send a case to a colleague for discussion. — — 1 3 1 The References button will be useful. — — — 2 3 The features are self-explanatory and easy to use. — — — 2 3 The key images from Pathology will be useful. — — 1 2 2 The key images from Radiology will be useful. — — — 2 3 The link to the complete Radiology study will be useful. — — — 2 3 The Correlation statement will be useful. — — — 3 2 The Action statement will be useful. — — — 4 1 The Correlation and Action features will change my practice. — — 1 4 —
Table 4
Free-text Responses to General Questions Regarding the RadPath System ( n = 5)
Question Response What are the problems, if any, with your current workflow for interpreting diagnostic results from Radiology and Pathology? “The direct links on RadPath are helpful as typically one would have to pull up three separate files: the pathology report, the images of the CT biopsy, and the original CT images. This format provided with the correlate is very helpful.”
“The biggest issue is getting the results of molecular analysis.” Could the RadPath display be confusing or cause diagnostic misinterpretation? “I am concerned that if the statement at the top isn’t repeated in the appropriate panel, there is a risk that people will miss it.” Are there other features you would like RadPath to have? “…it would be helpful if we knew which nodule was biopsied (i.e., CT showing needle into target).”
“Anticipated date of any outstanding studies.”
CT, computed tomography.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions and Future Work
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Miniño A.M., Murphy S.L., Xu J., et. al.: Deaths: final data for 2008. Nat Vital Stat Rep 2011; 59:
2. Liberman L., Drotman M., Morris E.A., et. al.: Imaging-histologic discordance at percutaneous breast biopsy. Cancer 2000; 89: pp. 2538-2546.
3. Takao M., Fukuda T., Iwanaga S., et. al.: Gastric cancer: evaluation of triphasic spiral CT and radiologic-pathologic correlation. J Comput Assist Tomogr 1998; 22: pp. 288-294.
4. Maetani Y., Itoh K., Egawa H., et. al.: Benign hepatic nodules in Budd-Chiari syndrome: radiologic–pathologic correlation with emphasis on the central scar. Am J Roentgenol 2002; 178: pp. 869-875.
5. Kuriyama K., Tateishi R., Doi O., et. al.: CT-pathologic correlation in small peripheral lung cancers. Am J Roentgenol 1987; 149: pp. 1139-1143.
6. Koo H.J., Choi H.J., Kim M.-H., et. al.: Radiologic–pathologic correlation of renal cell carcinoma associated with Xp11. 2 translocation. Acta Radiol 2013; 54: pp. 827-834.
7. Varma D., Ayala A., Carrasco C., et. al.: Chondrosarcoma: MR imaging with pathologic correlation. Radiographics 1992; 12: pp. 687-704.
8. Khurana B., Mortelé K.J., Glickman J., et. al.: Macrocystic serous adenoma of the pancreas: radiologic–pathologic correlation. Am J Roentgenol 2003; 181: pp. 119-123.
9. Sorace J., Aberle D.R., Elimam D., et. al.: Integrating pathology and radiology disciplines: an emerging opportunity?. BMC Med 2012; 10: pp. 100.
10. Shah V.I., Raju U., Chitale D., et. al.: False-negative core needle biopsies of the breast. Cancer 2003; 97: pp. 1824-1831.
11. Kim M.J., Kim E.-K., Park S.Y., et. al.: Imaging-histologic discordance at sonographically guided percutaneous biopsy of breast lesions. Eur J Radiol 2008; 65: pp. 163-169.
12. Office of the Assistant Secretary for Planning and Evaluation : The importance of radiology and pathology communication in the diagnosis and staging of cancer: mammography as a case study.2010.US Department of Health and Human ServicesWashington, DC
13. Crowe J.P., Patrick R.J., Rybicki L.A., et. al.: Does ultrasound core breast biopsy predict histologic finding on excisional biopsy?. Am J Surg 2003; 186: pp. 397-399.
14. Jackman R.J., Marzoni F.A., Rosenberg J.: False-negative diagnoses at stereotactic vacuum-assisted needle breast biopsy: long-term follow-up of 1,280 lesions and review of the literature. Am J Roentgenol 2009; 192: pp. 341-351.
15. Dillon M.F., Hill A.D., Quinn C.M., et. al.: The accuracy of ultrasound, stereotactic, and clinical core biopsies in the diagnosis of breast cancer, with an analysis of false-negative cases. Ann Surg 2005; 242: pp. 701.
16. Pfarl G., Helbich T.H., Riedl C.C., et. al.: Stereotactic 11-gauge vacuum-assisted breast biopsy: a validation study. Am J Roentgenol 2002; 179: pp. 1503-1507.
17. Schueller G., Jaromi S., Ponhold L., et. al.: US-guided 14-gauge core-needle breast biopsy: results of a validation study in 1352 cases. Radiology 2008; 248: pp. 406-413.
18. Mariotto A.B., Robin Yabroff K., Shao Y., et. al.: Projections of the cost of cancer care in the United States: 2010–2020. J Natl Cancer Inst 2011; 103: pp. 117-128.
19. Mihalik J.E., Krupka L., Davenport R., et. al.: The rate of imaging-histologic discordance of benign breast disease: a multidisciplinary approach to the management of discordance at a large university-based hospital. Am J Surg 2010; 199: pp. 319-323.
20. Fader D.J., Wise C.G., Normolle D.P., et. al.: The multidisciplinary melanoma clinic: a cost outcomes analysis of specialty care. J Am Acad Dermatol 1998; 38: pp. 742-751.
21. IOM (Institute of Medicine) : Best care at lower cost: the path to continuously learning health care in America.2012.National Academies PressWashington, DC
22. National Research Council : Toward precision medicine: building a knowledge network for biomedical research and a new taxonomy of disease.2011.National Academies PressWashington, DC
23. Tawfik O., Redick M.: Joint radiologist-pathologist review of diagnostic findings improves care of patients being screened for breast cancer. AHRQ Service Delivery Innovation Profile2010.
24. Oh A.S., Arnold C.W., Vangala S., et. al.: Imaging-histologic discordance at percutaneous biopsy of the lung. Acad Radiol 2015; 22: pp. 481-487.
25. Sutton C., McCallum A.: An introduction to conditional random fields for relational learning. Introd Stat Relat Learn 2006; pp. 93-128.