
Rationale and Objectives
First study to investigate the basic tissue elastic properties of the cervix in pre- and postmenopausal healthy women and to compare these normal findings with the results in a group of patients with focal pathology of the cervix.
Materials and Methods
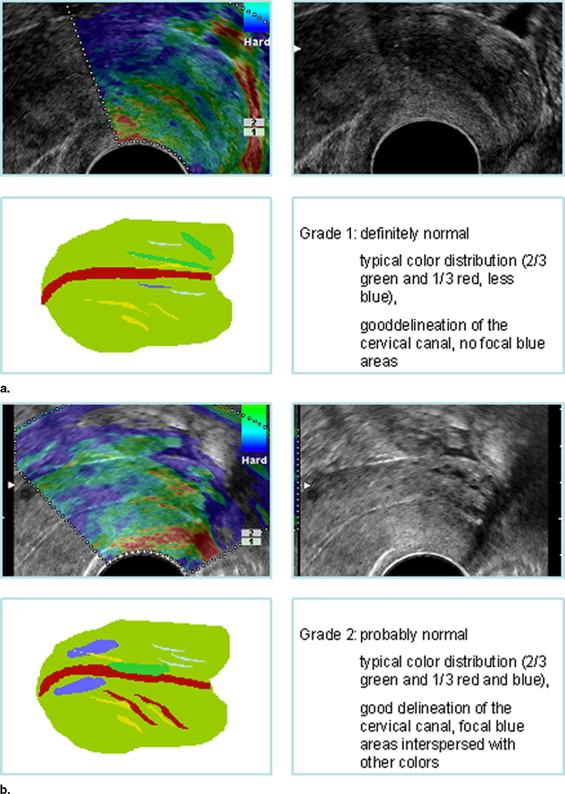
A total of 113 patients underwent transvaginal ultrasound, among them 24 with cervical pathology. The real-time elastography (Hitachi) information was color-coded and superimposed on the B-mode scan. The elastography images were analyzed by means of a software tool to identify thresholds for the colors red (soft), blue (hard), and green (medium hard), and the percentages of the three colors of the total area were determined. The results were correlated with age. In addition, scans were evaluated subjectively on an analogue scale from 1 (definitely normal) to 5 (definitely abnormal). Statistical analysis was performed using Anova, Wilcoxon’s test, and Pearson’s correlation.
Results
Computer-assisted generation of the color spectrum showed green to be predominant in both the normal group (67±13 %) and in the group with cervical pathology (64±15 %) without a significant difference between both groups (p=>0.05). Significant differences (p<0.05) in the blue color spectrum (hard tissue) were found between the 13 cervical tumor patients (34±15 %) and the normal group (26±13 %) but not between the CIN patients and normal women (19±12 %) (p>0.05). Subjective tumor characterization also showed significant differences (p<0.05) among the groups and good correlation with the histologic diagnosis (r2=0.744). There were no significant changes in color distribution with patient age (p>0.05).
Conclusion
Computer-assisted and subjective evaluation of cervical elastography allows differentiation of malignancy from normal findings. CIN cannot be identified with this modality. Elastographically, cervical tissue is of medium hardness and does not change with age.
A biological tissue possesses a specific inherent elasticity that may be altered by pathophysiological processes such as maturation, inflammation, or malignancy. The elasticity of a tissue is defined as the tension (pressure) required to produce relative elongation (stretching) and is a measure of the pressure necessary to achieve elastic ( ). In recent years, many study groups have focused on the development of imaging techniques to visualize such changes in tissue elasticity by determining the shearing modulus ( ). These groups study not only approaches based on magnetic resonance imaging but also state-of-the-art techniques of sonoelastography, which have already been investigated experimentally in different tissues as well as in patients ( ). The most recently introduced ultrasound (US) technique for the evaluation of tissue elasticity is real-time sonoelastography ( ). Using this technique, elasticity information is provided in real time and displayed in color on the B-mode scans similar to color Doppler information. Initial results achieved with real-time sonoelastography in different organs such as the breast and prostate are promising ( ). Tissue compressibility is used as a parameter in the differential diagnosis of breast lesions by ultrasonography, and a tumor that cannot be compressed has a 31% higher risk of malignancy ( ). Initial studies suggest that real-time elastography can be successfully used to assess breast tumors ( ). Because it is possible in principle to derive tissue elasticities from stretching values (which are calculated directly from high-frequency echo signals), the data needed can be obtained with endoprobes. Therefore, studying this new technique for evaluating the cervix, which is rigid when a tumor is present, is an interesting approach. The normal cervix consists mostly of collagen with a small proportion of muscle fibers. During pregnancy, for example, the collagen fibers are initially stabilized by decortin (PGS2) and dissolved by biglycan (PGS1) during the third trimester ( ). Therefore, the elastic properties of the cervix are affected not only by age but also by physiological factors. The standard screening and diagnostic tests for cervical cancer are cytologic smears and bimanual palpation, and transvaginal US has only a supplementary role ( ).
Based on these considerations, we performed a study to investigate whether real-time sonoelastography is able to visualize the normal elastic properties of the cervix in relation to patient age and to differentiate tumorous changes of the cervix in patients with cervical cancer or suspicious cytology findings from the normal appearance. To our knowledge, these questions have not been addressed in a clinical study previously (based on a PubMed search for the period from January 1996 to July 2006). More specifically, the questions to be answered in this first original article are whether cervical elasticity shows typical premenopausal and postmenopausal variations with age and whether these properties can serve to define a normal population. Besides defining the color (elastic) composition of the normal cervix, we examined selected cervical lesions by using real-time sonoelastography.
Materials and methods
Get Radiology Tree app to read full this article<
Table 1
Diagnosis of the 24 Patients With Cervical Pathology
Diagnosis (n = 24) ⁎ FIGO Classification CIN Classification Cervical cancer (n = 13) FIGO 0, 1 patient FIGO Ib, 4 patients FIGO III, 8 patients Cervical intraepithelial neoplasia (CIN) (n = 11) CIN II, 1 patient CIN III,10 patients
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Ultrasound Technique
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Evaluation
Get Radiology Tree app to read full this article<
Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Calculation of Age-Dependent Elasticity
Get Radiology Tree app to read full this article<
TQ=%red/%green TQ
=
%
red
/
%
green
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Computer-Assisted Analysis of Cervical Elasticity
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Subjective Evaluation of Cervical Elasticity
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Age-Dependent Cervical Elasticity
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Krouskop T.A., Wheeler T.M., Kallel F., et. al.: Elastic moduli of breast and prostate tissues under compression. Ultrason Imaging 1998; 20: pp. 260-274.
2. Konofagou E., Ophir J.: A new elastographic method for estimation and imaging of lateral displacements, lateral strains, corrected axial strains and Poisson’s ratios in tissues. Ultrasound Med Biol 1998; 24: pp. 1183-1199.
3. Ophir J., Garra B., Kallel F., et. al.: Elastographic imaging. Ultrasound Med Biol 2000; 26: pp. 23-29.
4. Bilgen M., Srinivasan S., Lachman L.B., Ophir J.: Elastography imaging of small animal oncology models: A feasibility study. Ultrasound Med Biol 2003; 29: pp. 1291-1296.
5. Shah N.S., Kruse S.A., Lager D.J., et. al.: Evaluation of renal parenchymal disease in a rat model with magnetic resonance elastography. Magn Reson Med 2004; 52: pp. 56-64.
6. Srinivasan S., Krouskop T., Ophir J.: A quantitative comparison of modulus images obtained using nanoindentation with strain elastograms. Ultrasound Med Biol 2004; 30: pp. 899-918.
7. Lorenzen J., Sinkus R., Adam G.: Elastographie: Quantitative Bildgebung der elastischen Gewebeeigenschaften. Fortschr Röntgenstr 2003; 175: pp. 623-630.
8. Kemper J., Sinkus R., Lorenzen J., et. al.: MR-Elastographie der Prostata: Erste In-vivo-Anwendung. Fortschr Röntgenstr 2004; 176: pp. 1094-1099.
9. Xydeas T., Siegmann K., Sinkus R., et. al.: Magnetic resonance elastography of the breast: correlation of signal intensity data with viscoelastic properties. Invest Radiol 2005; 40: pp. 412-420.
10. Frey H.: Realtime elastography. Radiologe 2003; 43: pp. 850-854.
11. Thomas A., Fischer T., Frey H., et. al.: An advanced method of ultrasound–real-time elastography: First results in 108 patients with breast lesions. Ultrasound Obstet Gynecol 2006; 28: pp. 335-340.
12. Frauscher F., Gradl J., Pallwein L.: Prostate ultrasound—For urologists only?. Cancer Imaging 2005; 23: pp. 76-82.
13. Lyshchik A., Higashi T., Asato R., et. al.: Thyroid gland tumor diagnosis at US. Radiology 2005; 237: pp. 202-211.
14. Varghese T., Shi H.: Elastographic imaging of thermal lesions in liver in-vivo using diaphragmatic stimuli. Ultrason Imaging 2004; 26: pp. 18-28.
15. Blohmer J.U., Schmalisch G., Hruby B., et. al.: Sonographische Kriterien in der Differentialdiagnose von Herdbefunden der Mamma. Ultraschall 1995; 16: pp. 525.
16. Itoh A., Ueno E., Tohno E., et. al.: Breast disease: Clinical application of US elastography for diagnosis. Radiology 2006; 239: pp. 341-350.
17. Ciatto S., Houssami N., Apruzzese A., et. al.: Categorizing breast mammographic density: Intra- and interobserver reproducibility of BI-RADS density categories. Breast 2005; 14: pp. 269-275.
18. Uldbjerg N., Ekman G., Malstrom A.: Ripening of the human uterine cervix related to changes in collagen, glycosaminoglycans and collagenolytic activity. Am J Obstet Gynecol 1982; 147: pp. 662-666.
19. Osmers R., Blaser J., Kuhn W., Tschesche H.: Interleukin-8 synthesis and the onset of labor. Obstet Gynecol 1995; 86: pp. 223-229.
20. Thomas A., Kümmel S., Sehouli J., Lichtenegger W.: Aktuelle Diagnostik und Therapie des Zervixkarzinoms. Academos Wissenschaftsverlag 2005; 3: pp. 54-62.
21. Michniewicz K., Oellinger J.: Bildgebende Diagnostik beim invasiven Zervixkarzinom: MRT, CT und Ultraschall. Zentralbl Gynakol 2001; 123: pp. 222-228.
22. Nitta N., Yamakawa M., Ueno E., et. al.: Tissue elasticity imaging based on combined autocorrelation method and 3D tissue model. Proc IEEE Ultrasonic 1998; 2: pp. 1447-1450.
23. Rief F.: 2003.Hanser FachbuchverlagMunich
24. Ophir J., Céspedes I., Ponneanti H., et. al.: A quantitative method for imaging the elasticity of biological tissue. Ultrason Imaging 1991; 13: pp. 111-114.
25. Parkin D.M., Bray F.I., Devesa S.S.: Cancer burden in the year 2000. Eur J Cancer 2001; 37: pp. 4-66.
26. Giles M., Garland S.: A study of women’s knowledge regarding human papillomavirus infection, cervical cancer and human papillomavirus vaccines. Aust N Z J Obstet Gynaecol 2006; 46: pp. 311-315.
27. Fiander A.N., Tristram A.J., Davidson E.J., et. al.: Prime-boost vaccination strategy in women with high-grade, noncervical anogenital intraepithelial neoplasia: Clinical results from a multicenter phase II trial. Int J Gynecol Cancer 2006; 16: pp. 1075-1081.
28. Thomas A.: Picture of the month. Ultrasound Obstet Gynecol 2006; 28: pp. 356-357.
29. Obenauer S., Sohns C., Werner C., et. al.: Retrospektive Analyse eines computerassisitierten Detektions-Systems CAD; in der digitalen Vollfeldmammographie in Abhängigkeit von der Histologie. Fortschr Röntgenstr 2005; 177: pp. 1103-1109.
30. Grunert J.H., Khalifa R., Gmelin E.: Computerassistierte Segmentierung und Formanalyse von 2975 mammären Mikroverkalkungen mit Hilfe der 7fachen Vergröβerungspräparateradiographie. Fortschr Röntgenstr 2004; 176: pp. 1759-1765.
31. Thomas A., Kümmel S., Fritzsche F., et. al.: Real-time sonoelastography performed in addition to B-mode ultrasound and mammography: Improved differentiation of breast lesions?. Acad Radiol 2006; 13: pp. 1496-1504.