
Rationale and Objectives
This study aimed to describe prenatal and postnatal imaging features and outcomes of neonates with neonatal lymphatic disorders (NLDs).
Materials and Methods
An institutional review board-approved search of the radiology database for patients with NLD identified five patients. Inclusion criteria include prenatal imaging (fetal magnetic resonance [MR] imaging and ultrasound) and postnatal three-dimensional T2 Sampling Perfection with Application optimized Contrasts using different flip angle Evolution (SPACE) and dynamic contrast-enhanced MR lymphangiography within 6 months of life. Chart review was undertaken to evaluate morbidity and mortality.
Results
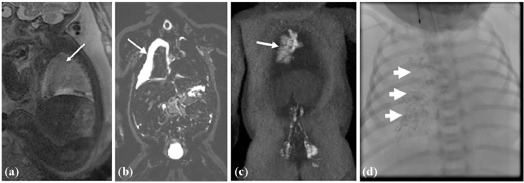
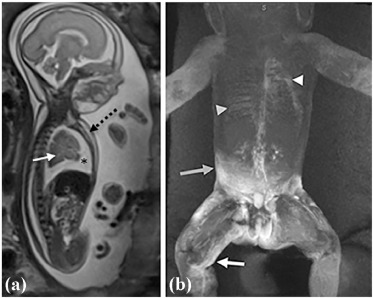
Prenatal finding of “nutmeg lung” or fetal pulmonary lymphatic disorder was identified in all five patients on fetal MR imaging, and in four of five patients on fetal ultrasound. Postnatal dynamic contrast-enhanced MR lymphangiography demonstrated abnormal lymphatic flow to the lungs in four of five patients, but absent in the single patient with coexisting hypoplastic left heart syndrome (HLHS). Dermal backflow was seen in one patient, also the only patient with prenatal body wall edema. Three patients with lymphatic flow to the lungs only were classified as neonatal chylothorax. The patient with dermal backflow and perfusion to the lungs was diagnosed with central lymphatic flow disorder (CLFD). The HLHS patient with normal lymphatic perfusion maintained the HLHS diagnosis. Of the five patients, the patient with CLFD and the one with HLHS expired because of respiratory distress.
Conclusions
NLDs can be recognized on prenatal and postnatal imaging and may be primary, as in neonatal chylothorax or CLFD, or secondary. In this small series, “nutmeg lung” was present in all patients. Prenatal imaging demonstrates that body wall edema may correlate with postnatal dermal backflow, which, in our small cohort, carried a poor prognosis.
Introduction
Neonatal lymphatic disorders (NLD) are a group of rare diseases that clinically manifest as one or a combination of chylous pleural effusion, chylous ascites, and soft tissue edema. Various terms are found in the literature to describe these conditions, including congenital chylothorax , non–immune neonatal hydrops fetalis, congenital lymphatic dysplasia , congenital pulmonary lymphangiectasia , and primary lymphatic dysplasia .
These disease processes are difficult to evaluate in part because of the rarity of these conditions and the lack of an effective minimally invasive lymphatic imaging method. Bellini et al. used lymphoscintigraphy to identify the lymphatic flow patterns in patients with NLD and demonstrated several findings, including congenital aplasia or hypoplasia of the peripheral lymphatics, congenital abnormalities of the abdominal or thoracic lymphatic trunks, and congenital lymphatic valvular incompetence . One of the advantages of lymphoscintigraphy is the ability to demonstrate the dynamics of lymphatic flow; however, its spatial resolution is significantly limited. Dynamic contrast-enhanced magnetic resonance lymphangiography (DCMRL) is a new lymphatic imaging technique that allows imaging of the central lymphatic system through the delivery of a gadolinium-based contrast agent into the inguinal lymph nodes under ultrasound (US) guidance . DCMRL provides both dynamic flow and anatomic information. Using this technique, Dori et al. and Itkin et al. visualized abnormal pulmonary lymphatic flow from the thoracic duct toward lung parenchyma in adult and pediatric patients with plastic bronchitis, a finding they named pulmonary lymphatic perfusion syndrome .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Patient Population
Get Radiology Tree app to read full this article<
TABLE 1
Presence or Absence of Prenatal and Postnatal Imaging Findings of the Five Patients with Neonatal Lymphatic Flow Disorder
Nutmeg Nutmeg Prenatal Postnatal 3D T2 SPACE Postnatal DCMRL Abdominal Cavity (Y/N) Patients Final Dx Lung on Fetal US (Y/N) Lung on Fetal MRI (Y/N) Ascites Body Wall Edema Neck/Supraclavicular (Y/N) Mediastinum/Perihilar (Y/N) Lung Interstitium (Y/N) Periportal (Y/N) RP (Y/N) Pleural Space (Y/N) Dermal Backflow (Y/N) Thoracic Duct Seen (Y/N) 1 NC Y Y N N Y Y Y Y Y Y N Y 2 CLFD Y Y N Y Y Y Y N Y Y Y N 3 NC Y Y N N Y Y Y Y Y Y N N 4 NC Y Y N N N Y Y Y Y Y N Y 5 HLHS N Y Y N Y Y Y Y Y N N Y
3D, three dimensional; CLFD, central lymphatic flow disorder; DCMRL, dynamic contrast-enhanced magnetic resonance lymphangiography; Dx, diagnosis; HLHS, hypoplastic left heart syndrome; MRI, magnetic resonance imaging; N, no; NC, neonatal chylothorax; RP, retroperitoneum; US, ultrasound; Y, yes.
Get Radiology Tree app to read full this article<
Prenatal Findings
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Postnatal Imaging
3D T2 SPACE
Get Radiology Tree app to read full this article<
Contrast Lymphangiography
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Outcome
Get Radiology Tree app to read full this article<
TABLE 2
Lymphatic Intervention Performed Along with Outcomes of Five Patients with Neonatal Lymphatic Disorders
Patients Dx Lymphatic Intervention Number of Days During the First 120 Days of Life Final Outcome Hospital ICU Ventilator ECMO 1 NC Lipiodol injection 113 71 111 0 Stable small pleural effusion without reaccumulation 2 CLFD None 75 75 66 0 Continued chylous effusions until demise due to respiratory distress 3 NC None 5 5 0 0 Resolution of pleural fluid without reaccumulation 4 NC Lipiodol injection 34 34 0 0 Improvement of pleural effusion without reaccumulation 5 HLHS None 120 120 120 5 Improving pleural effusion with refractory hypoxia post-Glenn with eventual demise
CLFD, central lymphatic flow disorder; Dx, diagnosis; ECMO, extracorporeal membrane oxygenation; HLHS, hypoplastic left heart syndrome; ICU, intensive care unit; NC, neonatal chylothorax.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Bialkowski A., Poets C.F., Franz A.R.: Congenital chylothorax: a prospective nationwide epidemiological study in Germany. Arch Dis Child Fetal Neonatal Ed 2015; 100: pp. F169-F172. Available at: http://fn.bmj.com/lookup/doi/10.1136/archdischild-2014-307274
2. Bellini C., Hennekam R.C.: Non-immune hydrops fetalis: a short review of etiology and pathophysiology. Am J Med Genet Part A 2012; 158 A: pp. 597-605.
3. Gray M., Kovatis K.Z., Stuart T., et. al.: Treatment of congenital pulmonary lymphangiectasia using ethiodized oil lymphangiography. J Perinatol 2014; 34: pp. 720-722. Available at: http://dx.doi.org/10.1038/jp.2014.71
4. Smeltzer D., Stickler D., Fleming R.: Primary lymphatic dysplasia in children: chylothorax, chylous ascites, and generalized lymphatic dysplasia. Eur J Pediatr 1986; 145: pp. 286-292.
5. Bellini C., Villa G., Sambuceti G., et. al.: Lymphoscintigraphy patterns in newborns and children with congenital lymphatic dysplasia. Lymphology 2014; 47: pp. 28-39.
6. Dori Y., Keller M.S., Rychik J., et. al.: Successful treatment of plastic bronchitis by selective lymphatic embolization in a Fontan patient. Pediatrics 2014; 134: pp. e590-e595. Available at: http://www.ncbi.nlm.nih.gov/pubmed/25002668
7. Dori Y., Keller M.S., Rome J.J., et. al.: Percutaneous lymphatic embolization of abnormal pulmonary lymphatic flow as treatment of plastic bronchitis in patients with congenital heart disease. Circulation 2016; 133: pp. 1160-1170.
8. Itkin M.G., McCormack F.X., Dori Y.: Diagnosis and treatment of lymphatic plastic bronchitis in adults using advanced lymphatic imaging and percutaneous embolization. Ann Am Thorac Soc 2016; 13: pp. 1689-1696.
9. Savla J.J., Itkin M., Rossano J.W., et. al.: Post-operative chylothorax in patients with congenital heart disease. J Am Coll Cardiol 2017; 69: pp. 2410-2422.
10. Pugash D., Brugger P.C., Bettelheim D., et. al.: Prenatal ultrasound and fetal MRI: the comparative value of each modality in prenatal diagnosis. Eur J Radiol 2008; 68: pp. 214-226.
11. Quinn T.M., Hubbard A.M., Adzick N.S.: Prenatal magnetic resonance imaging enhances fetal diagnosis. J Pediatr Surg 1998; 33: pp. 553-558.
12. Victoria T., Andronikou S.: The fetal MR appearance of “nutmeg lung”: findings in 8 cases linked to pulmonary lymphangiectasia. Pediatr Radiol 2014; 44: pp. 1237-1242.
13. Saul D., Degenhardt K., Iyoob S.D., et. al.: Hypoplastic left heart syndrome and the nutmeg lung pattern in utero: a cause and effect relationship or prognostic indicator?. Pediatr Radiol 2016; 46: pp. 483-489.
14. Seed M., Bradley T., Bourgeois J., et. al.: Antenatal MR imaging of pulmonary lymphangiectasia secondary to hypoplastic left heart syndrome. Pediatr Radiol 2009; 39: pp. 747-749.
15. Faul J.L., Berry G.J., Colby T., et. al.: Thoracic lymphangiomas, lymphangiectasis, lymphangiomatosis, and lymphatic dysplasia syndrome. Am J Respir Crit Care Med 2000; 161: pp. 1037-1046.
16. María V., Marugán D., Lopez-Gutierrez J.C., et. al.: Primary intestinal lymphangiectasia and its association with generalized lymphatic anomaly. J Pediatr Rev 2016; 4: pp. e4790.
17. Noonan J.A., Walters L.R., Reeves J.T.: Congenital pulmonary lymphangiectasis. Am J Dis Child 1970; 120: pp. 314-319.
18. Bellini C., Boccardo F., Toma P., et. al.: Pulmonary lymphangiectasia. Lymphology 2005; 38: pp. 111-121.