
Rationale and Objectives
To determine the recommended iodine dose of contrast material (CM) for hepatic arterial–dominant phase (HAP) and hepatic parenchymal phase (HPP) imaging to assess hypervascular hepatocellular carcinoma (HCC).
Materials and Methods
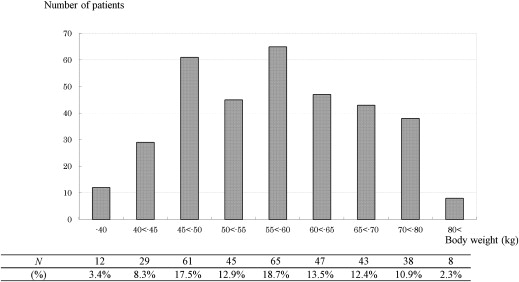
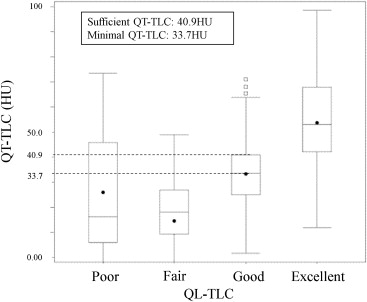
This was a prospective study including 348 patients with hypervascular HCC in 77 hospitals as a postmarketing surveillance to investigate the effects of body weight–tailored dose of CM (300 mgI/mL of iohexol) for hepatic multiphasic contrast-enhanced multidetector-row computed tomography imaging. Informed consent was obtained from all patients who were enrolled. The tumor-to-liver contrast (TLC) of HAP images was assessed qualitatively (QL-TLC) and quantitatively (QT-TLC [HU]; computed tomography [CT] value of tumor–CT value of hepatic parenchyma). Minimal and sufficient QT-TLC were defined as CT values corresponding to the median and 75% of QL-TLC assigned with “good,” respectively. The recommended iodine dose was estimated by the relationship between iodine dose (mgI/kg) and QT-TLC.
Results
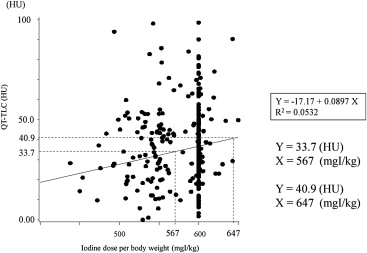
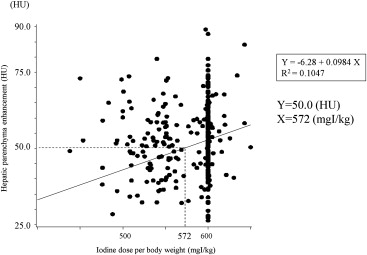
There was a good correlation between QL-TLC and QT-TLC. The recommended iodine dose of CM for HAP imaging was considered to be in the range of 567–647 mgI/kg based on minimal (33.7 HU) and sufficient QT-TLC (40.9 HU). Meanwhile, the recommended dose of CM for HPP imaging was 572 mgI/kg as a dose that gives hepatic enhancement more than 50 HU during HPP imaging.
Conclusions
The recommended iodine dose of CM for HAP and HPP imaging may be different, being 567–647 mgI/kg and 572 mgI/kg, respectively, in assessing hypervascular HCC.
There has been a recent trend for the dose of contrast material used in multiphasic contrast-enhanced computed tomography (CT) imaging of the liver that the dose of contrast material should be tailored according to the patients’ body weight to achieve adequate contrast enhancement. By introducing such a concept of body weight–tailored dose of contrast material, variation among patients with different body weights in the degree of contrast enhancement in the aorta and liver can be canceled .
Some investigators have attempted to determine the optimal dose of contrast material for multiphasic contrast-enhanced CT of the liver. In their studies, the optimal dose of contrast material has been determined based on a definition of the dose that can give adequate hepatic enhancement (>50 HU increase from unenhanced baseline HU of the liver) during hepatic parenchymal phase (HPP; identical to portal venous phase) . Summing up their reports, the optimal dose of contrast material for HPP imaging remains unclear because it ranges widely from 1.7 mL/kg to 2.5 mL/kg with 300 mgI/mL (520–750 mgI/kg). Such considerable discrepancy between their conclusions in the optimal dose might depend on the outdated methods including prolonged scan time throughout the entire liver with single-detector helical CT scanners and the limited, self-approving hepatic CT protocols.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Patients
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Patients’ Characteristics
Overall ( n = 348) Gender Male 255 (73.3 ∗ ) Female 93 (26.7) Age 72.6 ± 8.78 † Body weight 58.3 ± 11.25 Iodine dose per weight (mgI/kg) 584.5 ± 61.93 Injection flow rate (mL/s) 3.65 ± 0.65 Injection duration (s) 31.0 ± 3.23
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CT Imaging
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Imaging evaluation: Qualitative analysis
Get Radiology Tree app to read full this article<
Imaging evaluation: Quantitative analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Estimation of recommended iodine dose
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Relationship between QL-TLC and QT-TLC for HAP Imaging
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Estimation of the Recommended Iodine Dose for HAP Imaging
Get Radiology Tree app to read full this article<
Y(HU)=−17.17+0.0897X(mgI/kg) Y
(
HU
)
=
−
17.17
+
0.0897
X
(
mgI
/
kg
)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Estimation of the Recommended Iodine Dose for HPP Imaging
Get Radiology Tree app to read full this article<
Y(HU)=−6.28+0.0984X(mgI/kg) Y
(
HU
)
=
−
6.28
+
0.0984
X
(
mgI
/
kg
)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
A Quick Reference Table Showing Relationship between Recommended Volume of Contrast Material with 300 mgI/mL and Patient’s Body Weight
40 kg 45 kg 50 kg 55 kg 60 kg 65 kg 70 kg 80 kg 570 mgI/kg † 76 ∗ 86 95 105 114 124 133 152 600 mgI/kg 80 90 100 110 120 130 140 160 650 mgI/kg 87 98 108 119 130 141 152 173
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Awai K., Hori S.: Effect of contrast injection protocol with dose tailored to patient weight and fixed injection duration on aortic and hepatic enhancement at multidetector-row helical CT. Eur Radiol 2003; 13: pp. 2155-2160.
2. Awai K., Hiraishi K., Hori S.: Effect of contrast material injection duration and rate on aortic peak time and peak enhancement at dynamic CT involving injection protocol with dose tailored to patient weight. Radiology 2004; 230: pp. 142-150.
3. Ichikawa T., Erturk S.M., Araki T.: Multiphasic contrast-enhanced multidetector-row CT of liver: contrast-enhancement theory and practical scan protocol with a combination of fixed injection duration and patients’ body-weight-tailored dose of contrast material. Eur J Radiol 2006; 58: pp. 165-176.
4. Megibow A.J., Jacob G., Heiken J.P., et. al.: Quantitative and qualitative evaluation of volume of low osmolality contrast medium needed for routine helical abdominal CT. AJR Am J Roentgenol 2001; 176: pp. 583-589.
5. Heiken J.P., Brink J.A., McClennan B.L., et. al.: Dynamic incremental CT: effect of volume and concentration of contrast material and patient weight on hepatic enhancement. Radiology 1995; 195: pp. 353-357.
6. Yamashita Y., Komohara Y., Takahashi M., et. al.: Abdominal helical CT: evaluation of optimal doses of intravenous contrast material-a prospective randomized study. Radiology 2000; 216: pp. 718-723.
7. Ohashi I., Hanafusa K., Yoshida T.: Small hepatocellular carcinomas: two-phase dynamic incremental CT in detection and evaluation. Radiology 1993; 189: pp. 851-855.
8. Hollett M.D., Jeffrey R.B., Nino-Murcia M., et. al.: Dual-phase helical CT of the liver: value of arterial phase scans in the detection of small (< or = 1.5 cm) malignant hepatic neoplasms. AJR Am J Roentgenol 1995; 164: pp. 879-884.
9. Baron R.L., Oliver J.H., Dodd G.D., et. al.: Hepatocellular carcinoma: evaluation with biphasic, contrast-enhanced, helical CT. Radiology 1996; 199: pp. 505-511.
10. Mitsuzaki K., Yamashita Y., Ogata I., et. al.: Multiple-phase helical CT of the liver for detecting small hepatomas in patients with liver cirrhosis: contrast-injection protocol and optimal timing. AJR Am J Roentgenol 1996; 167: pp. 753-757.
11. Hwang G.J., Kim M.J., Yoo H.S., et. al.: Nodular hepatocellular carcinomas: detection with arterial-, portal-, and delayed-phase images at spiral CT. Radiology 1997; 202: pp. 383-388.
12. Yanaga Y., Awai K., Nakaura K., et. al.: Optimal contrast dose for depiction of hypervascular hepatocellular carcinoma at dynamic CT using 64-MDCT. AJR Am J Roentgenol 2008; 190: pp. 1003-1009.
13. Erturk S.M., Ichikawa T., Sou H., et. al.: Effect of duration of contrast material injection on peak enhancement times and values of the aorta, main portal vein, and liver at dynamic MDCT with the dose of contrast medium tailored to patient weight. Clin Radiol 2008; 63: pp. 263-271.
14. Bae K.T., Heiken J.P., Brink J.A.: Aortic and hepatic contrast medium enhancement at CT. Part I. Prediction with a computer model. Radiology 1998; 207: pp. 647-655.
15. Bae K.T.: Intravenous contrast medium administration and scan timing at CT: considerations and approaches. Radiology 2010; 256: pp. 32-61.
16. Leggett R.W., Williams L.R.: A proposed blood circulation model for Reference Man. Health Phys 1995; 69: pp. 187-201.
17. Ho L.M., Nelson R.C., Delong D.M.: Determining contrast medium dose and rate on basis of lean body weight: does this strategy improve patient-to-patient uniformity of hepatic enhancement during multi-detector row CT?. Radiology 2007; 243: pp. 431-437.
18. Kondo H., Kanematsu M., Goshima S., et. al.: Abdominal multidetector CT in patients with varying body fat percentages: estimation of optimal contrast material dose. Radiology 2008; 249: pp. 872-877.
19. Marin D., Nelson R.C., Samei E., et. al.: Hypervascular Liver tumors: low tube voltage, high tube current multidetector CT during late hepatic arterial phase for detection—initial clinical experience. Radiology 2009; 251: pp. 771-779.
20. Altenbernd J., Heusner T.A., Ringelstein A., et. al.: Dual-energy-CT of hypervascular liver lesions in patients with HCC: investigation of image quality and sensitivity. Eur Radiol 2011; 21: pp. 738-743.