
Rationale and Objectives
Breast arterial calcification (BAC) detected on mammography is frequently not included in final reports. However, previous studies have indicated that BAC may be evidence of general atherosclerotic vascular disease, and it can potentially be a useful marker of coronary artery disease. In addition, there are currently no available techniques for the quantification of calcium mass using mammography. The purpose of this study was to evaluate the reproducibility and inter-reader agreement of a technique for the quantification of BAC using standard digital mammography.
Materials and Methods
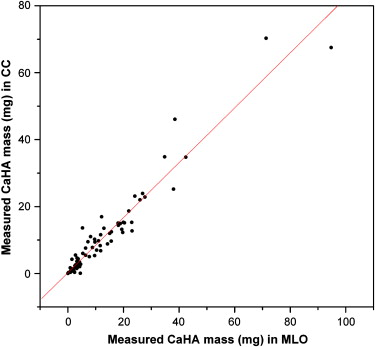
BAC mass was measured in a convenient, consecutive sample of 39 women aged 49 to 82 years attending routine mammographic examinations. BAC mass measurements were performed in standard mediolateral oblique (MLO) and craniocaudal (CC) views. To assess reproducibility, the BAC measurements obtained in MLO and CC views were compared.
Results
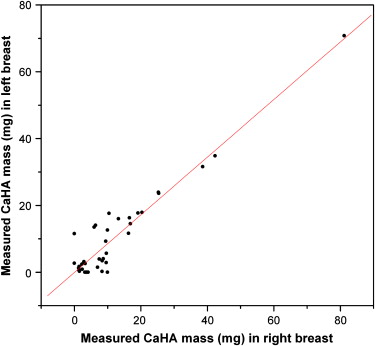
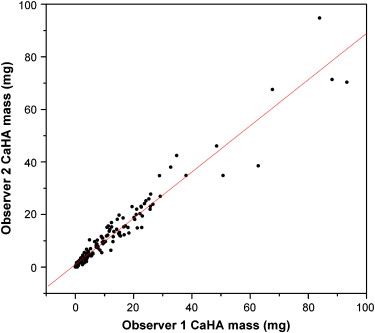
The measured BAC masses in CC ( M CC ) and MLO ( M MLO ) projections were related by M CC = 0.82( M MLO ) + 0.27 mg ( r = 0.97; standard error of estimation [SEE], 3.44 mg). The measured BAC masses in the left ( M L ) and right ( M R ) breasts were related by M L = 0.86( M R ) − 0.06 mg ( r = 0.95; SEE, 4.30 mg). The intraclass correlation coefficients for the measurement of calcium mass ranged from 0.94 in the left CC view to 0.99 in the right CC view.
Conclusion
A densitometry technique for the quantification of BAC mass was evaluated in patients using standard full-field digital mammography. The results demonstrated that this densitometric technique for the quantification of BAC mass is highly reproducible and has excellent inter-reader agreement. This technique may provide a quantitative metric for future studies relating the severity of BAC and cardiovascular risk.
Coronary artery disease (CAD) is the leading cause of death in women. Mammography is a common, inexpensive, and widely accepted test that is recommended to all middle-aged women to screen for breast cancer. Breast arterial calcification (BAC) detected on mammography is frequently not included in final reports, because it is considered a benign finding that is not relevant to the diagnosis of breast cancer. The preponderance of studies on this topic, including large cohorts in Europe and the United States, indicate that the detection and grading of BAC on mammography may be a useful marker of atherosclerosis and therefore may have value for cardiovascular risk stratification . The only exception is a smaller case-control study that reported no significant association between BAC and CAD detected on angiography .
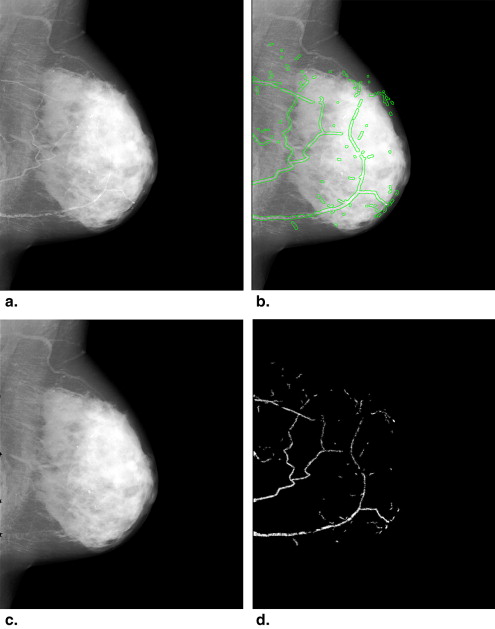
BAC assessment could be performed during regular rounds of screening mammography with minimal added burden to radiologists. However, additional evidence from large-scale prospective studies is needed to guide recommendations for routine BAC reporting in clinical practice. Previous studies on BAC have reported only the presence or absence of calcification on mammography. The currently available full-field digital mammographic systems provide the capability to quantify BAC. We recently developed a technique for the quantification of BAC using standard full-field digital mammography and performed an anthropomorphic breast phantom study that demonstrated the feasibility of quantifying vascular calcium mass using densitometry after taking into account the effects of scatter correction, breast thickness, breast density, anatomic background, and magnification error on calcium mass .
Get Radiology Tree app to read full this article<
Materials and methods
Patient Population
Get Radiology Tree app to read full this article<
Image Acquisition and Processing
Get Radiology Tree app to read full this article<
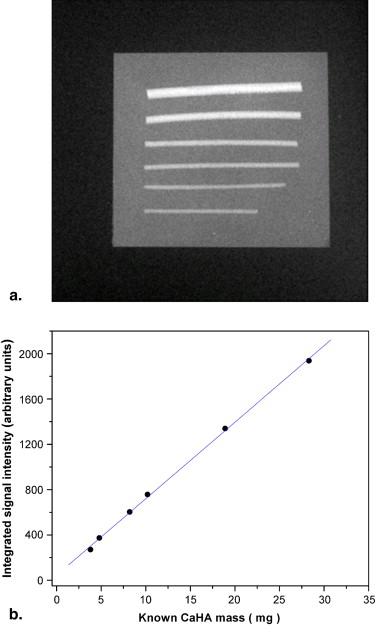
Calcium Calibration
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
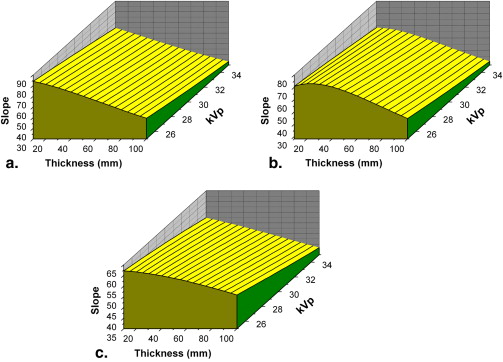
S(K,T)=(a1K+a2T)e(b1K+b2T), S
(
K
,
T
)
=
(
a
1
K
+
a
2
T
)
e
(
b
1
K
+
b
2
T
)
,
where K and T are the peak kilovoltage and thickness, respectively; S is the calcium calibration slope; and a 1 , a 2 , b 1 , and b 2 are fitting parameters. The fit was performed for both molybdenum and rhodium x-ray tube anodes. The relative root-mean-square error quantified by calculating the residuals was 0.84% of the mean calibration slope for the molybdenum anode and 1.05% of the mean calibration slope for the rhodium anode. The fitting of the calibration data to this two-dimensional surface permitted the calculation of calcium calibration slopes for points not explicitly sampled during the calibration process. The slope of the calibration curve was used to estimate CaHA mass from integrated signal intensity.
Get Radiology Tree app to read full this article<
Calcium Measurement
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Calcium Calibration
Get Radiology Tree app to read full this article<
![Figure 4, Measured calibration slope (integrated signal intensity/calcium hydroxyapatite mass [mg]) compared to predicted slope from phantom studies ( n = 17). The predicted ( S p ) and measured ( S m ) calibration slopes were related by S p = 1.114( S m ) + 0.984 ( r = 0.998; standard error of estimation, 0.613).](https://storage.googleapis.com/dl.dentistrykey.com/clinical/ReproducibilityofBreastArterialCalciumMassQuantificationUsingDigitalMammography/3_1s20S107663320800528X.jpg)
Get Radiology Tree app to read full this article<
Calcium Measurements
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Interpretation of Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Limitations
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Clinical Implications
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
References
1. van Noord P.A., Beijerinck D., Kemmeren J.M., van der Graaf Y.: Mammograms may convey more than breast cancer risk: breast arterial calcification and arterio-sclerotic related diseases in women of the DOM cohort. Eur J Cancer Prev 1996; 5: pp. 483-487.
2. Kemmeren J.M., Beijerinck D., van Noord P.A., et. al.: Breast arterial calcifications: association with diabetes mellitus and cardiovascular mortality. Work in progress. Radiology 1996; 201: pp. 75-78.
3. Iribarren C., Go A.S., Tolstykh I., Sidney S., Johnston S.C., Spring D.B.: Breast vascular calcification and risk of coronary heart disease, stroke, and heart failure. J Womens Health (Larchmt) 2004; 13: pp. 381-389.
4. Kataoka M., Warren R., Luben R., et. al.: How predictive is breast arterial calcification of cardiovascular disease and risk factors when found at screening mammography?. AJR Am J Roentgenol 2006; 187: pp. 73-80.
5. Doerger K., Whaley D., Berger P., Rowland C., Britain M.: Breast arterial calcification detected on mammography is a risk factor for coronary artery disease. Radiology 2002; 225: pp. 553.
6. Moshyedi A.C., Puthawala A.H., Kurland R.J., O’Leary D.H.: Breast arterial calcification: association with coronary artery disease. Work in progress. Radiology 1995; 194: pp. 181-183.
7. Pecchi A., Rossi R., Coppi F., Ligabue G., Modena M.G., Romagnoli R.: Association of breast arterial calcifications detected by mammography and coronary artery calcifications quantified by multislice CT in a population of post-menopausal women. Radiol Med (Torino) 2003; 106: pp. 305-312.
8. Dale P.S., Graham J., Nichols K.W., Catchings T., Richards M.: Mammography as a screening tool for peripheral vascular disease. Am J Surg 2006; 192: pp. 488-491.
9. Dale P.S., Mascarhenas C., Richards M., Mackie G.: Mammography as a screening tool for coronary artery disease. J Surg Res 2008; 148: pp. 1-6.
10. Henkin Y., Abu-Ful A., Shai I., Crystal P.: Lack of association between breast artery calcification seen on mammography and coronary artery disease on angiography. J Med Screen 2003; 10: pp. 139-142.
11. Molloi S., Xu T., Ducote J.L.: Quantification of breast arterial calcification using full field digital mammography. Med Phys 2008; 35: pp. 1428-1439.
12. White D.R.: The formulation of tissue substitute materials using basic interaction data. Phys Med Biol 1977; 22: pp. 889-899.
13. Wong J.T., Kamyar F., Molloi S.: Quantitative coronary angiography using image recovery techniques for background estimation in unsubtracted images. Med Phys 2007; 34: pp. 4003-4015.
14. Shrout P.E., Fleiss J.L.: Intraclass correlations: uses in assessing rater reliability. Psychol Bull 1979; 2: pp. 420-428.
15. American Cancer Society : Cancer facts & figures 2007.2007.American Cancer SocietyAtlanta, GA
16. Molloi S., Detrano R., Ersahin A., Roeck W., Morcos C.: Quantification of coronary arterial calcium by dual energy digital subtraction fluoroscopy. Med Phys 1991; 18: pp. 295-298.
17. Xu T., Ducote J.L., Wong J.T., Molloi S.: Feasibility of real time dual-energy imaging based on a flat panel detector for coronary artery calcium quantification. Med Phys 2006; 33: pp. 1612-1622.