
Rationale and Objectives
Intra-procedural measurement of hepatic perfusion following liver embolization continues to be a challenge. Blood volume imaging before and after interventional procedures would allow identifying the treatment end point or even allow predicting treatment outcome. Recent liver oncology studies showed the feasibility of parenchymal blood volume (PBV) imaging using an angiographic C-arm system. This study was done to evaluate the reproducibility of PBV measurements using cone beam computed tomography (CBCT) before and after embolization of the liver in a swine model.
Materials and Methods
CBCT imaging was performed before and after partial bland embolization of the left lobe of the liver in five adult pigs. Intra-arterial injection of iodinated contrast with a 6-second x-ray delay was used with a two-sweep 8-second rotation imaging protocol. Three acquisitions, each separated by 10 minutes to allow for contrast clearance, were obtained before and after embolization in each animal. Post-processing was carried out using dedicated software to generate three-dimensional (3D) PBV maps. Two region-of-interest measurements were placed on two views within the right and left lobe on each CBCT 3D PBV map. Variation in PBV for scans acquired within each animal was determined by the coefficient of variation and intraclass correlation. A Wilcoxon signed-rank test was used to test post-procedure reduction in PBV.
Results
The CBCT PBV maps showed mean coefficients of variation of 7% (range: 2%–16%) and 25% (range: 13%–34%) for baseline and embolized PBV maps, respectively. The intraclass correlation for PBV measurements was 0.89, demonstrating high reproducibility, with measurable reduction in PBV displayed after embolization ( P = 0.007).
Conclusions
Intra-procedural acquisition of 3D PBV maps before and after liver embolization using CBCT is highly reproducible and shows promising application for obtaining intra-procedural PBV maps during locoregional therapy.
Introduction
Objective measurement of hepatic perfusion during locoregional treatment could aid in the treatment of hepatocellular carcinoma (HCC). Although hepatic blood circulation is approximately 25% arterial and 75% portal venous in the healthy liver , the onset of neoangiogenesis in HCC leads to the domination of arterial supply to the tumor . For patients with underlying cirrhosis, the degree of arterialization reflects the stage , with dysplastic nodules and early HCC demonstrating some portal flow, but as HCC progresses the supply to the tumor rapidly morphs into exclusively arterial supply . In vivo assessment of organ perfusion, including measurement of blood volume contribution from the hepatic arterial and portal flow, is an established and reproducible technique using dynamic contrast-enhanced computed tomography (CT) . Specifically, pathologic changes during neoangiogenesis, the evolution from dysplasia to poorly differentiated HCC, and changes following transarterial chemoembolization have been studied by dynamic contrast-enhanced CT . Assessment of tumor characteristics during locoregional treatments, vis-à-vis quantitative hemodynamic characteristics, may offer a valuable diagnostic or treatment end point biomarker . Intra-procedural dynamic contrast-enhanced CT at the present time is infeasible. In contrast, the use of cone beam CT (CBCT) or C-arm CT as a complementary modality to digital subtraction angiography (DSA) during therapy is widely accepted and continues to become a routine part of the procedure . Moreover, within the past few years, a modified injection and reconstruction protocol designed for CBCT imaging has demonstrated the feasibility of calculating cerebral perfusion in canines and humans . Using a similar approach, it was shown that a modified injection and reconstruction protocol enables the calculation of parenchymal blood volume (PBV) within the liver using CBCT . These first clinical studies show the feasibility of PBV measurements before and after hepatic arterial treatment with its correlation to CT perfusion studies. However, up to now, no study has carefully evaluated the reproducibility of PBV measurements in the liver for one subject. Therefore, the objective of this study was to investigate the reproducibility of obtaining PBV measurements in a swine model using CBCT, before and after partial transarterial (bland) embolization of the liver.
Materials and Methods
Under approval by the Administrative Panel on Laboratory Animal Care, five female adult Yorkshire breed pigs (53 ± 0.9 kg) underwent CBCT imaging of the liver before and after partial particle embolization of the left lobe. During the duration of the experiments, animals were under the attendance of two licensed veterinary technicians. Prior to imaging, the animals were given intramuscular injection of Telazol (Fort Dodge Animal Health, KS) (5–7 mg/kg) combined with atropine (0.5 mg/kg). Following intubation, isoflurane was maintained at 1%–2% by mechanical ventilation. Assessment of vital signs, including heart rate, O 2 saturation, and end tidal CO 2 , was performed every 15 minutes. Primary dosage of 300 IU/kg of heparin was given intra-arterially and supplemented as needed. Directly prior to imaging procedures, a 7Fr sheath (Vanguard; Medrad, Indianola, PA) was placed within the right common femoral artery. Following an aortogram, a standard 5Fr end-hole catheter (AngioDynamics, Latham, NY) was placed in the common hepatic artery under fluoroscopic guidance. All pre-embolization and post-embolization imaging was performed following injection of iodinated contrast into the common hepatic artery using a dual-syringe power injector (MEDTRON Accutron HP-D, Saarbrücken, Germany). CBCT acquisition details are described later. A 2.3Fr microcatheter (Renegade HI-FLO; Boston Scientific, Natick, MA) was advanced through the 5Fr catheter, with the tip positioned in the left hepatic artery, under fluoroscopic guidance. The embolization to near stasis was performed by injecting 150–300 micron diameter microspheres (Embospheres; Merit Medical Systems, Inc, South Jordan, UT) to parts of the left lobe of the liver and was confirmed using DSA.
CBCT Image Acquisition Protocol
Get Radiology Tree app to read full this article<
Post-processing
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
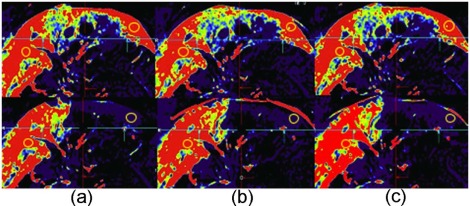
Table 1
Parenchymal Blood Volume Measurements Obtained Within a 2 cm 2 ROI Placed on Identical Regions of the Left and the Right Lobes, Across a Total of Six 3D Maps Corresponding to Three Scans Performed Before and Three Scans Performed After Partial Embolization for Each Study Animal
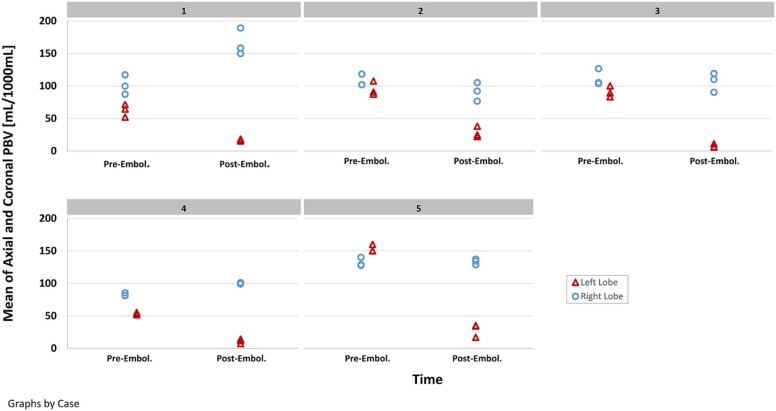
ID Baseline PBV (mL/1000 mL): Left Lobe Post-left Lobe Embolization PBV (mL/1000 mL): Left Lobe Scan 1 Scan 2 Scan 3 Mean Across 3 Scans Scan 1 Scan 2 Scan 3 Mean Across 3 Scans 1 64.40 71.35 52.05 62.60 16.70 15.25 18.30 16.75 2 87.25 107.55 90.80 95.20 38.15 24.90 22.25 28.43 3 100.15 83.25 89.15 90.85 11.20 6.20 5.95 7.78 4 55.20 51.75 52.95 53.30 14.10 7.15 12.00 11.08 5 159.90 150.05 150.05 153.33 35.15 16.95 34.35 28.82
ID Baseline PBV (mL/1000 mL): Right Lobe Post-left Lobe Embolization PBV (mL/1000 mL): Right Lobe Scan 1 Scan 2 Scan 3 Mean Across 3 Scans Scan 1 Scan 2 Scan 3 Mean Across 3 Scans 1 99.65 117.15 87.25 101.35 189.25 149.75 158.35 165.78 2 101.85 101.95 118.35 107.38 105.15 92.15 76.65 91.32 3 126.65 105.25 103.70 111.87 119.20 110.05 90.30 106.52 4 85.40 81.50 81.00 82.63 99.10 100.95 98.90 99.65 5 127.55 139.90 128.45 131.97 137.05 128.60 134.05 133.23
3D, three-dimensional; PBV, parenchymal blood volume; ROI, region-of-interest.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Summary and Conclusions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Miles K.A., Lee T.Y., Goh V., et. al.: Current status and guidelines for the assessment of tumour vascular support with dynamic contrast-enhanced computed tomography. Eur Radiol 2012; 22: pp. 1430-1441.
2. International Consensus Group for Hepatocellular Neoplasia. The International Consensus Group for Hepatocellular Neoplasia: Pathologic diagnosis of early hepatocellular carcinoma: a report of the International Consensus Group for Hepatocellular Neoplasia. Hepatology 2009; 49: pp. 658-664.
3. Park Y.N., Kim M.-J.: Hepatocarcinogenesis: imaging-pathologic correlation. Abdom Imaging 2011; 36: pp. 232-243.
4. Hashimoto K., Murakami T., Dono K., et. al.: Assessment of the severity of liver disease and fibrotic change: the usefulness of hepatic CT perfusion imaging. Oncol Rep 2006; 16: pp. 677-683.
5. Sahani D.V., Holakere N.-S., Mueller P.R., et. al.: Advanced hepatocellular carcinoma: CT perfusion of liver and tumor tissue—initial experience. Radiology 2007; 243: pp. 736-743.
6. Hayano K., Desai G.S., Kambadakone A.R., et. al.: Quantitative characterization of hepatocellular carcinoma and metastatic liver tumor by CT perfusion. Cancer Imaging 2013; 13: pp. 512-519.
7. Ippolito D., Sironi S., Pozzi M., et. al.: Hepatocellular carcinoma in cirrhotic liver disease. Functional computed tomography with perfusion imaging in the assessment of tumor vascularization. Acad Radiol 2008; 15: pp. 919-927.
8. Yang L., Zhang X., Tan B., et. al.: Computed tomographic perfusion imaging for the therapeutic response of chemoembolization for hepatocellular carcinoma. J Comput Assist Tomogr 2012; 36: pp. 226-230.
9. Tognolini A., Louie J.D., Hwang G.L., et. al.: Utility of C-arm CT in Patients with hepatocellular carcinoma undergoing transhepatic arterial chemoembolization. J Vasc Interv Radiol 2010; 21: pp. 339-347.
10. Wallace M.J., Murthy R., Kamat P.P., et. al.: Impact of C-arm CT on hepatic arterial interventions for hepatic malignancies. J Vasc Interv Radiol 2007; 18: pp. 1500-1507.
11. Ahmed A.S., Zellerhoff M., Strother C.M., et. al.: C-arm CT measurement of cerebral blood volume: an experimental study in canines. AJNR Am J Neuroradiol 2009; 30: pp. 917-922.
12. Struffert T., Deuerling-Zheng Y., Engelhorn T., et. al.: Feasibility of cerebral blood volume mapping by flat panel detector CT in the angiography suite: first experience in patients with acute middle cerebral artery occlusions. AJNR Am J Neuroradiol 2012; 33: pp. 618-625.
13. Struffert T., Kloska S., Engelhorn T., et. al.: Dynamic angiography and perfusion imaging using flat detector CT in the angiography suite: a pilot study in patients with acute middle cerebral artery occlusions. AJNR Am J Neuroradiol 2015; 36: pp. 1964-1970.
14. Ganguly A., Fieselmann A., Boese J., et. al.: In vitro evaluation of the imaging accuracy of C-arm conebeam CT in cerebral perfusion imaging. Med Phys 2012; 39: pp. 6652-6659.
15. Zhuang Z.G., Bin Zhang X., Han J.F., et. al.: Hepatic blood volume imaging with the use of flat-detector CT perfusion in the angiography suite: comparison with results of conventional multislice CT perfusion. J Vasc Interv Radiol 2014; 25: pp. 739-746.
16. Syha R., Groezinger G., Grosse U., et. al.: Parenchymal blood volume assessed by C-arm-based computed tomography in immediate posttreatment evaluation of drug-eluting bead transarterial chemoembolization in hepatocellular carcinoma. Invest Radiol 2016; 51: pp. 121-126.
17. Syha R., Grözinger G., Grosse U., et. al.: C-arm computed tomography parenchymal blood volume measurement in evaluation of hepatocellular carcinoma before transarterial chemoembolization with drug eluting beads. Cancer Imaging 2015; 15: pp. 22.
18. Plank C., Wolf F., Langenberger H., et. al.: Adrenal venous sampling using dyna-CT—a practical guide. Eur J Radiol 2012; 81: pp. 2304-2307.
19. Zellerhoff M., Deuerling-Zheng Y., Strother C.M., et. al.: Measurement of cerebral blood volume using angiographic C-arm systems. Proceedings of SPIE Medical Imaging 2009: Biomedical Applications in Molecular, Structural, and Functional Imaging, Vol. 72622009.
20. Struffert T., Deuerling-Zheng Y., Kloska S., et. al.: Flat detector CT in the evaluation of brain parenchyma, intracranial vasculature, and cerebral blood volume: a pilot study in patients with acute symptoms of cerebral ischemia. AJNR Am J Neuroradiol 2010; 31: pp. 1462-1469.
21. Jin B., Wang D., Lewandowski R.J., et. al.: Chemoembolization endpoints: effect on survival among patients with hepatocellular carcinoma. AJR Am J Roentgenol 2011; 196: pp. 919-928.
22. Kim D.Y., Ryu H.J., Choi J.Y., et. al.: Radiological response predicts survival following transarterial chemoembolisation in patients with unresectable hepatocellular carcinoma. Aliment Pharmacol Ther 2012; 35: pp. 1343-1350.
23. Jin B., Wang D., Lewandowski R.J., et. al.: Quantitative 4D transcatheter intraarterial perfusion MRI for standardizing angiographic chemoembolization endpoints. AJR Am J Roentgenol 2011; 197: pp. 1237-1243.
24. Lewandowski R.J., Wang D., Gehl J., et. al.: A comparison of chemoembolization endpoints using angiographic versus transcatheter intraarterial perfusion/MR imaging monitoring. J Vasc Interv Radiol 2007; 18: pp. 1249-1257.
25. Kinugasa H., Nouso K., Takeuchi Y., et. al.: Risk factors for recurrence after transarterial chemoembolization for early-stage hepatocellular carcinoma. J Gastroenterol 2012; 47: pp. 421-426.
26. Suk Oh J., Jong Chun H., Gil Choi B., et. al.: Transarterial chemoembolization with drug-eluting beads in hepatocellular carcinoma: usefulness of contrast saturation features on cone-beam computed tomography imaging for predicting short-term tumor response. J Vasc Interv Radiol 2013; 24: pp. 483-489.
27. Monsky W.L., Kim I., Loh S., et. al.: Semiautomated segmentation for volumetric analysis of intratumoral ethiodol uptake and subsequent tumor necrosis after chemoembolization. AJR Am J Roentgenol 2010; 195: pp. 1220-1230.
28. Wang D., Gaba R.C., Jin B., et. al.: Intra-procedural transcatheter intraarterial perfusion MRI as a predictor of tumor response to chemoembolization for hepatocellular carcinoma. Acad Radiol 2012; 18: pp. 828-836.
29. Struffert T., Deuerling-Zheng Y., Kloska S., et. al.: Cerebral blood volume imaging by flat detector computed tomography in comparison to conventional multislice perfusion CT. Eur Radiol 2011; 21: pp. 882-889.
30. Mordasini P., El-Koussy M., Brekenfeld C., et. al.: Applicability of tableside flat panel detector CT parenchymal cerebral blood volume measurement in neurovascular interventions: preliminary clinical experience. AJNR Am J Neuroradiol 2012; 33: pp. 154-158.
31. Royalty K., Manhart M., Pulfer K., et. al.: C-arm CT measurement of cerebral blood volume and cerebral blood flow using a novel high-speed acquisition and a single intravenous contrast injection. AJNR Am J Neuroradiol 2013; 34: pp. 2131-2138.
32. Peynircioglu B., Hizal M., Cil B., et. al.: Quantitative liver tumor blood volume measurements by a C-arm CT post-processing software before and after hepatic arterial embolization therapy: comparison with MDCT perfusion. Diagn Interv Radiol 2015; 21: pp. 71-77.
33. Kudo K., Sasaki M., Yamada K., et. al.: Differences in CT perfusion maps generated by different commercial software: quantitative analysis by using identical source data of acute stroke patients. Radiology 2010; 254: pp. 200-209.