
Rationale and Objectives
The aim of this study was to determine whether the diagnostic yield of thyroid fine-needle aspirations (FNAs) changes over the course of residency training.
Materials and Methods
We identified 5418 ultrasound-guided thyroid nodule FNAs performed in our radiology department from 2004 through 2012. For each FNA, we recorded if the FNA was performed by a resident and if so the name of the resident and supervising attending radiologist. For each resident, we determined the level of training based on their graduation year from our residency program and the date of the FNA as well as prior surgical training and if they completed subsequent interventional radiology fellowship. Pathology reports were reviewed, and FNAs were classified as diagnostic or nondiagnostic (ND). Generalized mixed models were used to assess ND rate with postgraduate years, including residents with and without prior surgical training or if they subsequently completed an interventional radiology fellowship.
Results
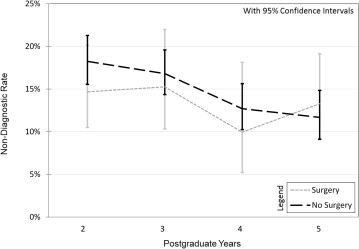
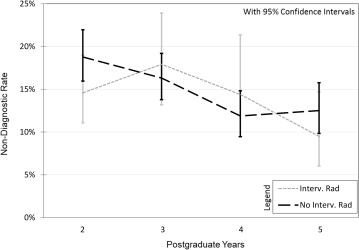
Of the 5418 thyroid FNAs, 3164 (58.4%) were performed by a radiology resident under the direct supervision of an attending physician. There was a significant decrease in ND rate as postgraduate years increased ( P < .05). A significant decrease in ND rate was found as postgraduate years increased for residents without prior surgical training ( P = .0007) or subsequent training in interventional radiology ( P = .0014); however, no significant decrease was found for residents with surgical training ( P = .37) or completing an interventional radiology fellowship ( P = .08). In addition, no significant difference was found for ND rate between postgraduate year 4 (PGY4) and PGY5 ( P > .05).
Conclusions
ND thyroid FNA rates progressively decrease with training level, suggesting that early and continued participation in procedures throughout residency improves outcomes. This is particularly true for residents without prior surgical training or subsequent interventional radiology fellowship.
Thyroid nodules are common and typically benign. Current clinical guidelines recommend fine-needle aspiration (FNA) of nodules > 1–1.5 cm, and of smaller nodules with concerning sonographic features . The reported diagnostic yield of thyroid FNA varies from 80% to 99%, with an average of 85% . Although it is well documented that diagnostic rates can be improved by routine onsite cytopathology evaluation for adequacy, it is expensive and inefficient, particularly at high volume centers . The effect of biopsy technique on nondiagnostic (ND) rates has also been studied. For example, two studies have demonstrated equal efficacy of aspiration versus suction-assisted FNA techniques . Visualization of the needle within the nodule along its long axis has been shown to improve diagnostic rates for deep nodules when compared with visualization along the needle’s short axis . Needle size seems to be relatively unimportant as studies comparing needles from 21 to 27 ga have not shown a diagnostic advantage of the larger bore needles .
One small study showed no difference in ND rates between an experienced attending radiologist and a new attending radiologist . Another study examining attending pathologists’ interpretations of thyroid FNA based on number of years of experience found that less experienced pathologists were more likely to interpret samples as ND or atypical, whereas more experienced pathologists were more likely to interpret samples as benign . To our knowledge, the effect of resident training level on ND thyroid FNA rates is unknown. The aim of this study was to determine whether the diagnostic yield of thyroid FNA changes over the course of residency training.
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
ND FNA Rates by Level of Training, Comparing Residents with and without Prior Surgical Training, and Whether They Completed a Subsequent Interventional Radiology Fellowship
Level of Training ND Rate (%) Surgery (95% CI) No Surgery (95% CI) Interventional Radiology (95% CI) No Interventional Radiology (95% CI) PGY2 14.7 (10.5–20.2) 18.2 (15.6–21.3) 14.6 (11.1–19.0) 18.8 (16.0–22.0) PGY3 15.3 (10.3–22.0) 16.8 (14.4–19.6) 17.9 (13.2–23.9) 16.3 (13.8–19.2) PGY4 9.9 (5.2–18.1) 12.7 (10.2–15.6) 14.4 (9.4–21.3) 11.9 (9.5–14.8) PGY5 13.3 (9.0–19.1) 11.7 (9.1–14.8) 9.5 (6.0–14.7) 12.5 (9.8–15.8)
CI, confidence interval; FNA, fine-needle aspiration; ND, nondiagnostic; PGY, postgraduate year.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Frates M.C., Benson C.B., Charboneau J.W., et. al.: Management of thyroid nodules detected at US: society of radiologists in ultrasound consensus conference statement. Radiology 2005; 237: pp. 794-800.
2. Cibas E.S., Alexander E.K., Benson C.B., et. al.: Indications for thyroid FNA and pre-FNA requirements: a synopsis of the national cancer institute thyroid fine-needle aspiration state of the science conference. Diagn Cytopathol 2008; 36: pp. 390-399.
3. American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer, Cooper D.S., Doherty G.M., Haugen B.R., et. al.: Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 2009; 19: pp. 1167-1214.
4. Ceresini G., Corcione L., Morganti S., et. al.: Ultrasound-guided fine-needle capillary biopsy of thyroid nodules, coupled with on-site cytologic review, improves results. Thyroid 2004; 14: pp. 385-389.
5. Yassa L., Cibas E.S., Benson C.B., et. al.: Long-term assessment of a multidisciplinary approach to thyroid nodule diagnostic evaluation. Cancer 2007; 111: pp. 508-516.
6. Yang J., Schnadig V., Logrono R., et. al.: Fine-needle aspiration of thyroid nodules: a study of 4703 patients with histologic and clinical correlations. Cancer 2007; 111: pp. 306-315.
7. Nayar R., Ivanovic M.: The indeterminate thyroid fine-needle aspiration: experience from an academic center using terminology similar to that proposed in the 2007 national cancer institute thyroid fine needle aspiration state of the science conference. Cancer 2009; 117: pp. 195-202.
8. Gharib H., Goellner J.R.: Fine-needle aspiration biopsy of the thyroid: an appraisal. Ann Intern Med 1993; 118: pp. 282-289.
9. Zhu W., Michael C.W.: How important is on-site adequacy assessment for thyroid FNA? An evaluation of 883 cases. Diagn Cytopathol 2007; 35: pp. 183-186.
10. Gomez-Macias G.S., Garza-Guajardo R., Segura-Luna J., et. al.: Inadequate fine needle aspiration biopsy samples: pathologists versus other specialists. Cytojournal 2009; 6: pp. 9.
11. Poller D.N., Kandaswamy P.: A simplified economic approach to thyroid FNA cytology and surgical intervention in thyroid nodules. J Clin Pathol 2013; 66: pp. 583-588.
12. Redman R., Zalaznick H., Mazzaferri E.L., et. al.: The impact of assessing specimen adequacy and number of needle passes for fine-needle aspiration biopsy of thyroid nodules. Thyroid 2006; 16: pp. 55-60.
13. Abraham T.M., de las Morenas A., Lee S.L., et. al.: In thyroid fine-needle aspiration, use of bedside-prepared slides significantly increased diagnostic adequacy and specimen cellularity relative to solution-based samples. Thyroid 2011; 21: pp. 237-242.
14. O’Malley M.E., Weir M.M., Hahn P.F., et. al.: US-guided fine-needle aspiration biopsy of thyroid nodules: adequacy of cytologic material and procedure time with and without immediate cytologic analysis. Radiology 2002; 222: pp. 383-387.
15. Eedes C.R., Wang H.H.: Cost-effectiveness of immediate specimen adequacy assessment of thyroid fine-needle aspirations. Am J Clin Pathol 2004; 121: pp. 64-69.
16. Tublin M.E., Martin J.A., Rollin L.J., et. al.: Ultrasound-guided fine-needle aspiration versus fine-needle capillary sampling biopsy of thyroid nodules: does technique matter?. J Ultrasound Med 2007; 26: pp. 1697-1701.
17. de Carvalho G.A., Paz-Filho G., Cavalcanti T.C., et. al.: Adequacy and diagnostic accuracy of aspiration vs. capillary fine needle thyroid biopsies. Endocr Pathol 2009; 20: pp. 204-208.
18. Kandil E., Khalek M.A., Alabbas H., et. al.: Comparison of ultrasound-guided biopsy technique for thyroid nodules with respect to adequacy of cytological material. J Otorhinolaryngol Relat Spec 2011; 73: pp. 177-181.
19. Degirmenci B., Haktanir A., Albayrak R., et. al.: Sonographically guided fine-needle biopsy of thyroid nodules: the effects of nodule characteristics, sampling technique, and needle size on the adequacy of cytological material. Clin Radiol 2007; 62: pp. 798-803.
20. Gumus M., Cay N., Algin O., et. al.: Comparison of 21 and 27 gauge needles for determining sample adequacy in the aspiration biopsy of thyroid nodules. Diagn Interv Radiol 2012; 18: pp. 102-105.
21. Lee Y.J., Kim D.W., Jung S.J.: Comparison of sample adequacy, pain-scale ratings, and complications associated with ultrasound-guided fine-needle aspiration of thyroid nodules between two radiologists with different levels of experience. Endocrine 2013 Feb 21; [Epub ahead of print]
22. Houlton J.J., Sun G.H., Fernandez N., et. al.: Thyroid fine-needle aspiration: does case volume affect diagnostic yield and interpretation?. Arch Otolaryngol Head Neck Surg 2011; 137: pp. 1136-1139.
23. Baloch Z.W., Cibas E.S., Clark D.P., et. al.: The national cancer institute thyroid fine needle aspiration state of the science conference: a summation. Cytojournal 2008; 5: pp. 6. 6413-5-6
24. Wotruba A.L., Stewart J., Scheberl T., et. al.: Added value, decreased cost: the evolving role of the cytotechnologist for preliminary screening and triage of thyroid aspirates. Diagn Cytopathol 2011; 39: pp. 896-899.
25. Olson M.T., Tatsas A.D., Ali S.Z.: Cytotechnologist-attended on-site adequacy evaluation of thyroid fine-needle aspiration: comparison with cytopathologists and correlation with the final interpretation. Am J Clin Pathol 2012; 138: pp. 90-95.
26. Bruni S.G., Bartlett E., Yu E.: Factors involved in discrepant preliminary radiology resident interpretations of neuroradiological imaging studies: a retrospective analysis. AJR 2012; 198: pp. 1367-1374.
27. Tomich J., Retrouvey M., Shaves S.: Emergency imaging discrepancy rates at a level 1 trauma center: identifying the most common on-call resident “misses.”. Emerg Radiol 2013; Jul 26; [Epub ahead of print]
28. Khan R., Krupinski E., Graham J.A., et. al.: Assessing first year radiology resident competence pre-call: development and implementation of a computer-based exam before and after the 12 month training requirement. Acad Radiol 2012; 19: pp. 752-758.
29. Silas A.M., Perrich K.D., Hoffer E.K., et. al.: Complication rates and outcomes of 536 implanted subcutaneous chest ports: do rates differ based on the primary operator’s level of training?. Acad Radiol 2010; 17: pp. 464-467.
30. Xu B.J., Duszak R., McGinnis R.S., et. al.: Increased fluoroscopy time for central venous catheter placement by radiology residents versus staff radiologists. J Am Coll Radiol 2013; 10: pp. 518-522.
31. Villard P.F., Vidal F.P., Ap Cenydd L., et. al.: Interventional radiology virtual simulator for liver biopsy. Int J Comput Assist Radiol Surg 2013; Jul 24; [Epub ahead of print]
32. Meng K., Lipson J.A.: Utilizing a PACS-integrated ultrasound-guided breast biopsy simulation exercise to reinforce the ACR practice guideline for ultrasound-guided percutaneous breast interventional procedures during radiology residency. Acad Radiol 2011; 18: pp. 1324-1328.
33. Stein-Wexler R., Sanchez T., Roper G.E., et. al.: An interactive teaching device simulating intussusception reduction. Pediatr Radiol 2010; 40: pp. 1810-1815.
34. Luboz V., Zhang Y., Johnson S., et. al.: ImaGiNe Seldinger: first simulator for Seldinger technique and angiography training. Comput Methods Programs Biomed 2013; 111: pp. 419-434.
35. Mendiratta-Lala M., Williams T., de Quadros N., et. al.: The use of a simulation center to improve resident proficiency in performing ultrasound-guided procedures. Acad Radiol 2010; 17: pp. 535-540.