
Rationale and Objectives
To evaluate the performance of radiology residents in the interpretation of on-call, emergency “triple-rule-out” (TRO) computed tomographic (CT) studies in patients with acute chest pain.
Materials and Methods
The study was institutional review board–approved and Health Insurance Portability and Accountability Act compliant. Data from 617 on-call TRO studies were analyzed. Dedicated software enables subspecialty attendings to grade discrepancies in interpretation between preliminary trainee reports and their final interpretation as “unlikely to be significant” (minor discrepancies) or “likely to be significant” for patient management (major discrepancies). The frequency of minor, major and all discrepancies in resident’s TRO interpretations was compared to 609 emergent non–electrocardiography (ECG)-synchronized chest CT studies using Pearson χ 2 test.
Results
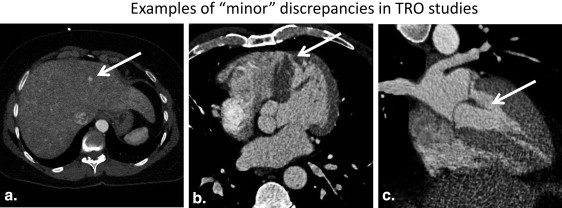
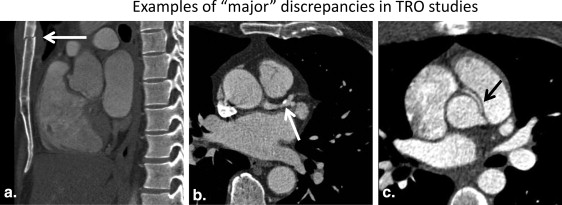
Minor discrepancies occurred more often in the TRO group (9.1% vs. 3.9%, P < .001), but there was no difference in the frequency of major discrepancies (2.1% vs. 2.8%, P = .55). Minor discrepancies in the TRO group most commonly resulted from missed extrathoracic findings with missed liver lesions being the most frequent. Major discrepancies mostly encompassed cardiac and extracardiac vascular findings but did not result in unnecessary interventions, significant immediate changes in management, or adverse patient outcomes.
Conclusions
On-call resident interpretation of TRO CT studies in patients with acute chest pain is congruent with final subspecialty attending interpretation in the overwhelming majority of cases. The rate of discrepancies likely to affect patient management in this domain is not different from emergent non–ECG-synchronized chest CT.
In patients presenting with acute, undifferentiated, or atypical chest pain, computed tomography (CT) offers the possibility of ruling out obstructive coronary artery disease, pulmonary embolism, acute aortic syndrome, and other pathologies in a single comprehensive evaluation . This approach is commonly referred to as “triple-rule-out” (TRO) CT and is performed as an electrocardiography (ECG)–synchronized CT angiography (CTA) study of the heart or the entire chest . Evidence on the clinical utility of this approach is rapidly accumulating .
At the majority of academic institutions throughout the United States, preliminary interpretation of emergent diagnostic imaging studies in the on-call setting is provided by radiology trainees. On-call imaging studies are typically reviewed and finalized by subspecialty attending radiologists during normal business hours. For a number of imaging modalities and indications, a small but significant discrepancy rate between preliminary residents’ and final subspecialists’ interpretation has been demonstrated .
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Study Design and Selection of Studies
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CT Examination Protocols
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Grading of Discrepancies between Preliminary and Final Interpretation
Get Radiology Tree app to read full this article<
Analysis of Sources of Discrepancies
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Analysis of Potential Impact on Patient Management and Outcome
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Examinations Included
Get Radiology Tree app to read full this article<
Frequency of Discrepancies between Preliminary and Final Interpretation
Get Radiology Tree app to read full this article<
Table 1
Agreement and Discrepancy Rates for the Triple-Rule-Out and Control Groups
Triple-Rule-Out Group ( n = 617), n (%) Control Group ( n = 609), n (%)P Value All discrepancies 69 (11.2) 41 (6.7) .008 Minor discrepancies 56 (9.1) 24 (3.9) <.001 Major discrepancies 13 (2.1) 17 (2.8) .55
Get Radiology Tree app to read full this article<
Sources of Minor Discrepancies in the Non–ECG-Synchronized Chest CT Control Group
Get Radiology Tree app to read full this article<
Table 2
Most Common Sources of “Minor” Discrepancies in the Control Group
Category of Abnormalities Number of Cases with Discrepancies Most Common Discrepancies Pulmonary parenchymal 9 Missed pulmonary nodules ( n = 4) Extrathoracic 9 Missed splenic lesions ( n = 2) Vascular 5 Missed subsegmental pulmonary embolism ( n = 2)
Get Radiology Tree app to read full this article<
Sources of Major Discrepancies in the Non–ECG-Synchronized Chest CT Control Group
Get Radiology Tree app to read full this article<
Table 3
Sources of “Major” Discrepancies in the Control Group
Number of Cases with Discrepancies Discrepancy 3 Missed pulmonary embolus 3 Missed pneumonia 3 Missed pulmonary edema 1 Missed left ventricular hypertrophy 1 Missed diffuse bronchiectasis 1 Missed stab wound tract hemorrhage 1 Missed esophagitis 1 Missed ascites 1 Missed lung mass 1 Missed pneumothorax 1 Missed premature coronary artery disease 17 Total
Get Radiology Tree app to read full this article<
Sources of Minor Discrepancies in the TRO Group
Get Radiology Tree app to read full this article<
Table 4
Most Common Sources of “Minor” Discrepancies in the Triple-Rule-Out Group
Category of Abnormalities Number of Cases with Discrepancies Most Common Discrepancy Extrathoracic 12 Missed liver lesion ( n = 8) Coronary 9 Overcalling degree of coronary stenosis ( n = 6) Congenital cardiac 9 Missed ventricular septal defect ( n = 4) Pulmonary parenchymal 7 Missed pulmonary nodules ( n = 5) Cardiac noncoronary 7 Subtle wall motion abnormalities ( n = 3)
Get Radiology Tree app to read full this article<
Sources of Major Discrepancies in the TRO Group
Get Radiology Tree app to read full this article<
Table 5
Sources of “Major” Discrepancies in the Triple-Rule-Out Group
Number of Cases with Discrepancies Discrepancy 4 Overcalling degree of coronary stenosis 1 Missed anomalous origin with “malignant” course of right coronary artery 1 Missed global hypokinesis with left ventricular enlargement and heart failure 1 Overestimation of calcium score 1 Missed displaced sternal body fracture 1 Low ejection fraction 1 Esophagitis 1 Left ventricular hypertrophy 1 Pericarditis 1 Mediastinal lymphadenopathy 13 Total
Get Radiology Tree app to read full this article<
Impact on Patient Management and Outcome
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Becker H.C., Johnson T.: Cardiac CT for the assessment of chest pain: imaging techniques and clinical results. Eur J Radiol 2012; 81: pp. 3675-3679.
2. Johnson T.R., Nikolaou K., Becker A., et. al.: Dual-source CT for chest pain assessment. Eur Radiol 2008; 18: pp. 773-780.
3. Takakuwa K.M., Halpern E.J.: Evaluation of a “triple rule-out” coronary CT angiography protocol: use of 64-Section CT in low-to-moderate risk emergency department patients suspected of having acute coronary syndrome. Radiology 2008; 248: pp. 438-446.
4. Halpern E.J.: Triple-rule-out CT angiography for evaluation of acute chest pain and possible acute coronary syndrome. Radiology 2009; 252: pp. 332-345.
5. Mammen L., White R.D., Woodard P.K., et. al.: ACR Appropriateness Criteria ® on chest pain, suggestive of acute coronary syndrome. J Am Coll Radiol 2011; 8: pp. 12-18.
6. Stillman A.E., Oudkerk M., Ackerman M., et. al.: Use of multidetector computed tomography for the assessment of acute chest pain: a consensus statement of the North American Society of Cardiac Imaging and the European Society of Cardiac Radiology. Int J Cardiovasc Imaging 2007; 23: pp. 415-427.
7. Frauenfelder T., Appenzeller P., Karlo C., et. al.: Triple rule-out CT in the emergency department: protocols and spectrum of imaging findings. Eur Radiol 2009; 19: pp. 789-799.
8. Bastarrika G., Thilo C., Headden G.F., et. al.: Cardiac CT in the assessment of acute chest pain in the emergency department. AJR Am J Roentgenol 2009; 193: pp. 397-409.
9. Hoffmann U., Nagurney J.T., Moselewski F., et. al.: Coronary multidetector computed tomography in the assessment of patients with acute chest pain. Circulation 2006; 114: pp. 2251-2260.
10. Goldstein J.A., Gallagher M.J., O’Neill W.W., et. al.: A randomized controlled trial of multi-slice coronary computed tomography for evaluation of acute chest pain. J Am Coll Cardiol 2007; 49: pp. 863-871.
11. Henzler T., Gruettner J., Meyer M., et. al.: Coronary computed tomography and triple rule out CT in patients with acute chest pain and an intermediate cardiac risk for acute coronary syndrome: part 2: economic aspects. Eur J Radiol 2013; 82: pp. 106-111.
12. Bamberg F., Marcus R.P., Schlett C.L., et. al.: Imaging evaluation of acute chest pain: systematic review of evidence base and cost-effectiveness. J Thorac Imaging 2012; 27: pp. 289-295.
13. Carney E., Kempf J., DeCarvalho V., et. al.: Preliminary interpretations of after-hours CT and sonography by radiology residents versus final interpretations by body imaging radiologists at a level 1 trauma center. AJR Am J Roentgenol 2003; 181: pp. 367-373.
14. Ruutiainen A.T., Scanlon M.H., Itri J.N.: Identifying benchmarks for discrepancy rates in preliminary interpretations provided by radiology trainees at an academic institution. J Am Coll Radiol 2011; 8: pp. 644-648.
15. Yoon L.S., Haims A.H., Brink J.A., et. al.: Evaluation of an emergency radiology quality assurance program at a level I trauma center: abdominal and pelvic CT studies. Radiology 2002; 224: pp. 42-46.
16. Herzog C., Kerl J.M., De Rosa S., et. al.: Influence of observer experience and training on proficiency in coronary CT angiography interpretation. Eur J Radiol 2013; 82: pp. 1240-1247.
17. Pugliese F., Hunink M.G., Gruszczynska K., et. al.: Learning curve for coronary CT angiography: what constitutes sufficient training?. Radiology 2009; 251: pp. 359-368.
18. Boiselle P.M., Hoffmann U., Schoepf U.J., et. al.: Expert opinion : Is 24/7 coverage necessary for implementing coronary CT angiography in the emergency room setting?. J Thorac Imaging 2013; 28: pp. 203.
19. Antman E.M., Cohen M., Bernink P.J., et. al.: The TIMI risk score for unstable angina/non-ST elevation MI: a method for prognostication and therapeutic decision making. JAMA 2000; 284: pp. 835-842.
20. Strauss A., Corbin J.: Grounded theory methodology. An overview.Denzin N.Lincoln Y.Handbook of qualitative research.1994.Sage PublicationsThousand Oaks, CA:pp. 273-285. London
21. Bechtold R.E., Chen M.Y., Ott D.J., et. al.: Interpretation of abdominal CT: analysis of errors and their causes. J Comput Assist Tomogr 1997; 21: pp. 681-685.
22. Tomich J., Retrouvey M., Shaves S.: Emergency imaging discrepancy rates at a level 1 trauma center: identifying the most common on-call resident “misses”. Emerg Radiol 2013; 20: pp. 499-505.
23. Wechsler R.J., Spettell C.M., Kurtz A.B., et. al.: Effects of training and experience in interpretation of emergency body CT scans. Radiology 1996; 199: pp. 717-720.
24. Stevens K.J., Griffiths K.L., Rosenberg J., et. al.: Discordance rates between preliminary and final radiology reports on cross-sectional imaging studies at a level 1 trauma center. Acad Radiol 2008; 15: pp. 1217-1226.
25. Davenport M.S., Ellis J.H., Khalatbari S.H., et. al.: Effect of work hours, caseload, shift type, and experience on resident call performance. Acad Radiol 2010; 17: pp. 921-927.
26. Cooper V.F., Goodhartz L.A., Nemcek A.A., et. al.: Radiology resident interpretations of on-call imaging studies: the incidence of major discrepancies. Acad Radiol 2008; 15: pp. 1198-1204.
27. Chung J.H., Strigel R.M., Chew A.R., et. al.: Overnight resident interpretation of torso CT at a level 1 trauma center an analysis and review of the literature. Acad Radiol 2009; 16: pp. 1155-1160.
28. Strub W.M., Vagal A.A., Tomsick T., et. al.: Overnight resident preliminary interpretations on CT examinations: should the process continue?. Emerg Radiol 2006; 13: pp. 19-23.
29. Lal N.R., Murray U.M., Eldevik O.P., et. al.: Clinical consequences of misinterpretations of neuroradiologic CT scans by on-call radiology residents. AJNR Am J Neuroradiol 2000; 21: pp. 124-129.
30. Ruchman R.B., Jaeger J., Wiggins E.F., et. al.: Preliminary radiology resident interpretations versus final attending radiologist interpretations and the impact on patient care in a community hospital. AJR Am J Roentgenol 2007; 189: pp. 523-526.
31. Jakanani G.C., Botchu R., Gupta S., et. al.: Out of hours multidetector computed tomography pulmonary angiography: are specialist resident reports reliable?. Acad Radiol 2012; 19: pp. 191-195.
32. Gruettner J., Fink C., Walter T., et. al.: Coronary computed tomography and triple rule out CT in patients with acute chest pain and an intermediate cardiac risk profile. Part 1: impact on patient management. Eur J Radiol 2013; 82: pp. 100-105.