
Rationale and Objectives
To compare the clinical outcomes of retrograde transplantar arch angioplasty and conventional below-the-knee (BTK) anterograde recanalization.
Materials and Methods
One hundred twelve limbs in 96 patients underwent attempt at antegrade tibial angioplasty. Among 27 technical failures, retrograde trans-dorsal or -planter percutaneous transluminal angioplasty was attempted in 22 limbs. Ankle–brachial index (ABI), thrombolysis in myocardial infarction (TIMI) flow grade, and dorsal/plantar arterial pulse score improvement were compared immediately after the procedures between patients received successful anterograde angioplasty (anterograde angioplasty group [AAG], 85 limbs in 71 patients) and retrograde angioplasty (retrograde angioplasty group [RAG], 22 limbs in 20 patients). Target vessel restenosis and limb salvage were observed during follow-up.
Results
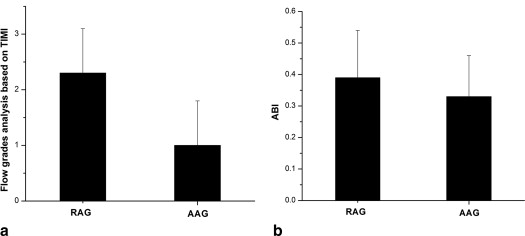
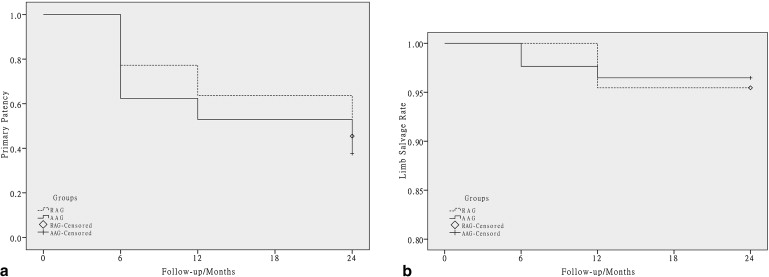
Primary technical success rate was 75.9% in the RAG (vs. 74.0% AAG, P > .05). ABI improved from 0.55 ± 0.21 to 0.93 ± 0.19 in the RAG (vs. 0.56 ± 0.14 to 0.89 ± 0.18 AAG, P > .05). TIMI flow grade demonstrated greater reperfusion of distal foot tissue in the RAG (2.3 ± 0.8 vs. 1.0 ± 0.8, P < .05). Primary patency rates at 12 and 24 months were 63.6% (14 of 22) and 45.5% (10 of 22) in the RAG and 52.9% (45 of 85) and 37.6% (32 of 85) in the AAG, respectively ( P > .05). Kaplan–Meier analysis after 24 months found limb salvage rates of 93.8% in the RAG and 96.5% in the AAG ( P > .05).
Conclusions
Retrograde transplantar arch angioplasty achieved better immediate blood flow and similar ABI improvement, primary patency rate, and limb salvage rate compared to conventional transtibial angioplasty for BTK occlusions. This could become a supplementary technique when anterograde angioplasty fails.
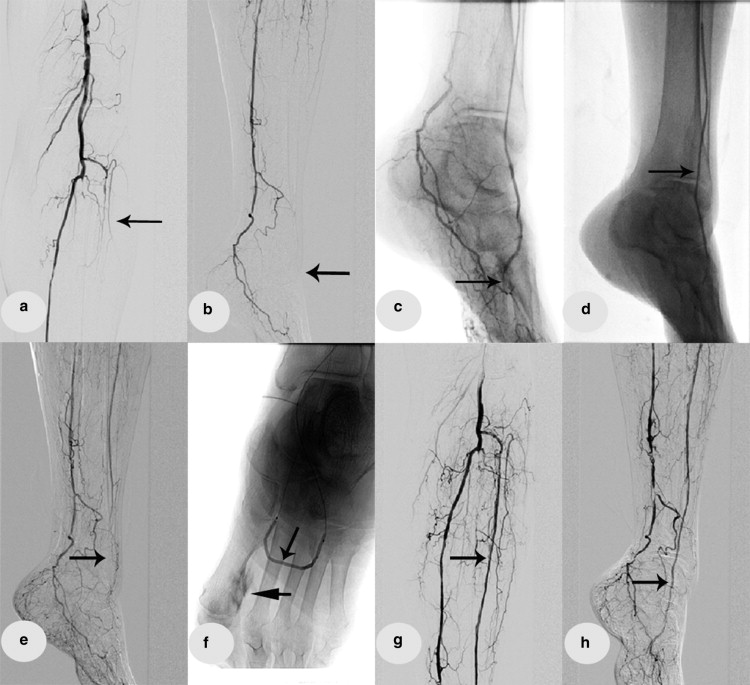
In patients with diabetes, peripheral vascular disease is a major vascular complication associated with high morbidity and mortality . Severe occlusive disease is often observed in the leg, especially in below-the-knee (BTK) arteries . The development of long balloons and new interventional procedures has provided effective treatments , but the success rate of percutaneous transluminal angioplasty (PTA) for BTK arterial occlusion remains suboptimal because of poor vessel runoff and high surgical risk. Since Fusaro et al. reported a case of plantar to dorsalis pedis artery (DPA) subintimal angioplasty (SA), there have been several reports on retrograde transplantar arch angioplasty in BTK arterial occlusion . However, most published articles are case reports or small sample studies and focused mainly on the technical success rate. There is a lack of research comparing retrograde transplantar arch angioplasty with anterograde angioplasty in terms of clinical outcome, vascular restenosis, and limb salvage rate. The aim of this study was to compare the clinical results of retrograde transplantar arch angioplasty via the DPA or the lateral plantar artery (LPA) for BTK arterial occlusion with those of conventional angioplasty.
Materials and methods
Patient Information
One hundred twelve limbs in 96 patients underwent attempt at antegrade tibial angioplasty. Among 27 technical failures, retrograde trans-dorsal or -planter PTA was attempted in 22 limbs. Ninety-one successfully treated patients were divided into a conventional anterograde angioplasty group (AAG; 85 limbs in 71 patients) and a retrograde angioplasty group (RAG; 22 limbs in 20 patients); other angioplasty techniques such as collateral vessel angioplasty and subintimal arterial flossing with antegrade–retrograde intervention technique via direct puncture of the DPA or the anterior or posterior tibial artery were beyond the scope of this study. Ulcer was present in four (18.2%) limbs in the RAG and 12 (14.1%) limbs in the AAG. Rest pain was present in four (18.5%) limbs in the RAG and 11 (12.9%) limbs in the AAG. The general condition and clinical data of the patients are outlined in Table 1 . All patients underwent a detailed physical examination, clinical assessments, and radiologic evaluation, including DPA or LPA pulse volume score, ankle–brachial index (ABI), and lower limb magnetic resonance angiography (MRA) or arterial ultrasonography. Indications of arterial occlusive disease on evaluation were reduction or absence of DPA or LPA pulse; ABI <0.9 (in the absence of arterial calcification); and vascular occlusion of BTK arteries confirmed by lower limb MRA or arterial ultrasonography. When two of these three indications were present, digital subtraction angiography was performed to further assess the vascular condition, with subsequent angioplasty if necessary.
Table 1
Patient and Lesion Characteristics in the Retrograde Angioplasty Group (RAG) and Anterograde Angioplasty Group (AAG)
Patient Characteristic RAG ( n = 20) AAG ( n = 71)P Value Age (years) 72.3 ± 6.0 (62–82) 70.0 ± 9.4 (52–85) .431 Gender (male) 14 (70.0) 52 (73.2) .774 Diabetes duration (years) 14.0 ± 4.5 (8–20) 14.0 ± 8.6 (1–30) .850 Hypertension 15 (75.0) 38 (53.5) .085 Chronic renal insufficiency (creatinine > 133 μmol/L) 6 (30.0) 16 (22.5) .778 Coronary artery disease 3 (15.0) 8 (11.3) .701 Smoking habit 6 (30.0) 25 (35.2) .383 Intermittent claudication 15 (75.0) 49 (69.0) .605 Rest pain 4 (18.2) 11 (12.9) .734 Ulcer 4 (18.2) 12 (14.1) .746 Rutherford classification .244 Stage 0 1 16 Stage 1 1 11 Stage 2 2 14 Stage 3 8 5 Stage 4 4 3 Stage 5 0 0 Stage 6 4 22 Lesion characteristic — Total number of limbs 22 85 Unilateral limb 18 (93.3) 57 (80.3) Bilateral limbs 2 (6.7) 14 (19.7) Location ATA + DPA 14 80 PTA + LPA 6 5 DPA 1 0 LPA 1 0 Length (cm) ≥10 18 76 <10 4 9
ATA, anterior tibial artery; DPA, dorsalis pedis artery; LPA, lateral plantar artery; PTA, posterior tibial artery.
Continuous data are presented as the mean ± standard deviation (range); categorical data are given as counts (percentages).
Get Radiology Tree app to read full this article<
Procedures
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Outcome Evaluation and Definitions
Get Radiology Tree app to read full this article<
Follow-up Protocol
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Faglia E., Clerici G., Caminiti M., et. al.: Mortality after major amputation in diabetic patients with critical limb ischemia who did and did not undergo previous peripheral revascularization data of a cohort study of 564 consecutive diabetic patients. J Diabetes Complications 2010; 24: pp. 265-269.
2. Faglia E., Dalla Paola L., Clerici G., et. al.: Peripheral angioplasty as the first-choice revascularization procedure in diabetic patients with critical limb ischemia: prospective study of 993 consecutive patients hospitalized and followed between 1999 and 2003. Eur J Vasc Endovasc Surg 2005; 29: pp. 620-627.
3. Park S.W., Kim J.S., Yun I.J., et. al.: Clinical outcomes of endovascular treatments for critical limb ischemia with chronic total occlusive lesions limited to below-the-knee arteries. Acta Radiol 2013; 54: pp. 785-789.
4. Lo R.C., Darling J., Bensley R.P., et. al.: Outcomes following infrapopliteal angioplasty for critical limb ischemia. J Vasc Surg 2013; 57: pp. 1455-1463. discussion 63–4
5. Scheinert D., Katsanos K., Zeller T., et. al.: A prospective randomized multicenter comparison of balloon angioplasty and infrapopliteal stenting with the sirolimus-eluting stent in patients with ischemic peripheral arterial disease: 1-year results from the ACHILLES trial. J Am Coll Cardiol 2012; 60: pp. 2290-2295.
6. Fusaro M., Dalla Paola L., Brigato C., et. al.: Plantar to dorsalis pedis artery subintimal angioplasty in a patient with critical foot ischemia: a novel technique in the armamentarium of the peripheral interventionist. J Cardiovasc Med (Hagerstown) 2007; 8: pp. 977-980.
7. Zhu Y.Q., Zhao J.G., Li M.H., et. al.: Retrograde transdorsal-to-plantar or transplantar-to-dorsal intraluminal re-entry following unsuccessful subintimal angioplasty for below-the-ankle arterial occlusion. J Endovasc Ther 2010; 17: pp. 712-721.
8. Manzi M., Fusaro M., Ceccacci T., et. al.: Clinical results of below-the knee intervention using pedal-plantar loop technique for the revascularization of foot arteries. J Cardiovasc Surg (Torino) 2009; 50: pp. 331-337.
9. Chomel S., Douek P., Moulin P., et. al.: Contrast-enhanced MR angiography of the foot: anatomy and clinical application in patients with diabetes. AJR Am J Roentgenol 2004; 182: pp. 1435-1442.
10. Manzi M., Cester G., Palena L.M., et. al.: Vascular imaging of the foot: the first step toward endovascular recanalization. Radiographics 2011; 31: pp. 1623-1636.
11. Palena L.M., Brocco E., Manzi M.: The clinical utility of below-the-ankle angioplasty using “transmetatarsal artery access” in complex cases of CLI. Catheter Cardiovasc Interv 2014; 83: pp. 123-129.
12. Palena L.M., Manzi M.: Extreme below-the-knee interventions: retrograde transmetatarsal or transplantar arch access for foot salvage in challenging cases of critical limb ischemia. J Endovasc Ther 2012; 19: pp. 805-811.
13. Gibson C.M., Cannon C.P., Murphy S.A., et. al.: Relationship of the TIMI myocardial perfusion grades, flow grades, frame count, and percutaneous coronary intervention to long-term outcomes after thrombolytic administration in acute myocardial infarction. Circulation 2002; 105: pp. 1909-1913.
14. Gardner A.W., Parker D.E., Montgomery P.S., et. al.: Diabetic women are poor responders to exercise rehabilitation in the treatment of claudication. J Vasc Surg 2014; 59: pp. 1036-1043.
15. Liu J., Wu Y., Li Z., et. al.: Endovascular treatment for intermittent claudication in patients with peripheral arterial disease: a systematic review. Ann Vasc Surg 2013;
16. Giugliano G., Perrino C., Schiano V., et. al.: Endovascular treatment of lower extremity arteries is associated with an improved outcome in diabetic patients affected by intermittent claudication. BMC Surg 2012; 12: pp. S19.