
Rationale and Objectives
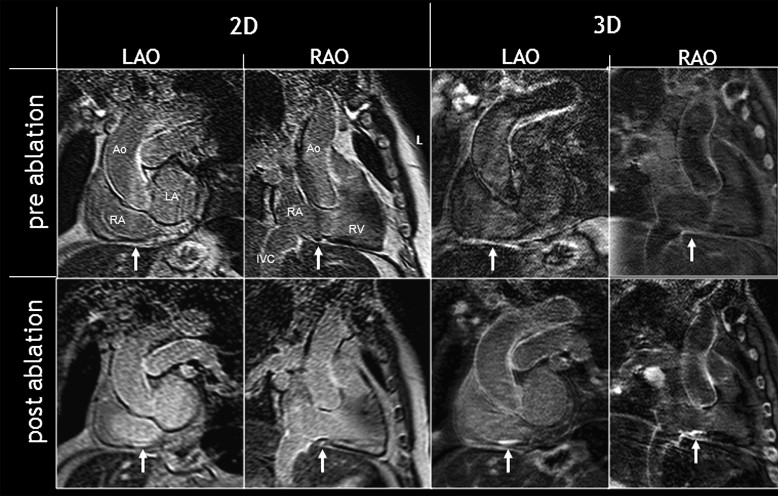
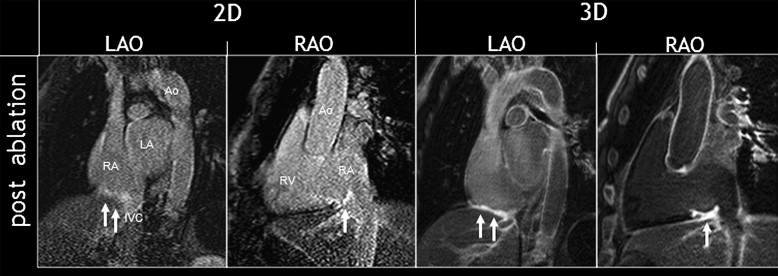
To prospectively compare the diagnostic performance of two-dimensional (2D) and high spatial resolution three-dimensional (3D) late enhancement magnetic resonance imaging (MRI) for the detection of scar tissue caused by catheter ablation of the right atrium in patients with atrial flutter.
Materials and Methods
Forty-seven patients were enrolled. In 16 patients, imaging of the cavotricuspid isthmus was performed before and after catheter ablation, 16 subjects were imaged before, and 15 after catheter ablation, resulting in a total of 63 examinations. MRI included a standard 2D breathhold and a high-resolution navigator-gated 3D T1-weighted gradient-echo inversion-recovery sequence in right and left anterior oblique views. Two readers assessed the subjective image quality on a 4-point scale (1 = excellent) and the presence of late enhancement (blinded/ in consensus).
Results
The average image quality was 1.6 for both imaging approaches. In consensus reading, the sensitivity was 83% versus 100%, specificity 97% versus 89%, accuracy 90% versus 94%, positive predictive value 96% versus 89%, negative predictive value 86% versus 100% for 2D and 3D, respectively. The interobserver agreement was 0.86 for 2D and 0.78 for 3D imaging.
Conclusions
For the noninvasive identification of scars in the cavotricuspid isthmus after right atrial flutter, ablation 2D imaging was more consistent, whereas 3D sequences showed superior sensitivity for the depiction of late enhancement.
Introduction
Radiofrequency ablation (RFA) of the isthmus between the vena cava inferior and tricuspid annulus is the recommended therapy for isthmus-dependent (“typical”) atrial flutter, and catheter-based isolation of the pulmonary veins is a highly effective therapeutic option to prevent recurrent atrial fibrillation in symptomatic patients.
Although atrial fibrillation has a much higher prevalence and rising incidence among elder people, atrial flutter is less frequent. Ablation of the cavotricuspid isthmus (CTI) aims to generate linear scars in the atrial myocardium to cut off macro-reentry mechanisms around the tricuspid valve . A single catheter ablation of the CTI cures a high percentage (about 80%) of the patients ; reablation has to be performed in recurrent cases, which count up to approximately 40% including late recurrent cases .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Patients
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Atrial Flutter RFA Technique
Get Radiology Tree app to read full this article<
MRI of the Cavotricuspid Isthmus
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data and Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Po=(both readers with positive finding+both readers with negative finding)/allfindings. Po
=
(
both readers with positive finding
+
both readers with negative finding
)
/
all
findings
.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Ppos=(2× both readers’positive findings)/(2× both readers’positive findings+disagreeing findings) Ppos
=
(
2
× both readers
’
positive findings
)
/
(
2
× both readers
’
positive findings
+
disagreeing findings
)
Ppos estimates the conditional probability, given that one of the raters, randomly selected, makes a positive rating, the other rater will also do so.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Kappa(K)=(Po−Pe)/(1−Pe) Kappa
(
K
)
=
(
Po
-
Pe
)
/
(
1
-
Pe
)
and Pe defined as:
Pe=[(all positive findings of reader1/all findings)×(all positive findings of reader2/all findings)]+[(all negative findings of reader1/all findings)×all negative findings of reader2/all findings)]. Pe
=
[
(
all positive findings of reader
1
/
all findings
)
×
(
all positive findings of reader
2
/
all findings
)
]
+
[
(
all negative findings of reader
1
/
all findings
)
×
all negative findings of reader
2
/
all findings
)
]
.
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Diagnostic Values for Two-dimensional Sequence Sets
Reader 1 (%) Reader 2 (%) Consensus (%) Specificity 90.6 95.3 96.8 Sensitivity 62.1 71.0 83.3 Accuracy 77.0 82.0 90.2 Positive predictive value 85.7 91.7 96.2 Negative predictive value 72.5 75.7 85.7
Table 2
Diagnostic Values for Three-dimensional Sequence Sets
Reader 1 (%) Reader 2 (%) Consensus (%) Specificity 82.1 93.1 89.3 Sensitivity 95.8 95.8 100 Accuracy 88.5 94.3 94.1 Positive predictive value 82.1 92.0 88.5 Negative predictive value 95.8 96.4 100
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Feld G.K., Fleck R.P., Chen P.S., et. al.: Radiofrequency catheter ablation for the treatment of human type 1 atrial flutter. Identification of a critical zone in the reentrant circuit by endocardial mapping techniques. Circulation 1992; 86: pp. 1233-1240.
2. Cappato R., Calkins H., Chen S.A., et. al.: Updated worldwide survey on the methods, efficacy, and safety of catheter ablation for human atrial fibrillation. Circ Arrhythm Electrophysiol 2009; 3: pp. 32-38.
3. Wokhlu A., Hodge D.O., Monahan K.H., et. al.: Long-term outcome of atrial fibrillation ablation: impact and predictors of very late recurrence. J Cardiovasc Electrophysiol 2010; 21: pp. 1071-1078.
4. Cabrera J.A., Sanchez-Quintana D., Ho S.Y., et. al.: The architecture of the atrial musculature between the orifice of the inferior caval vein and the tricuspid valve: the anatomy of the isthmus. J Cardiovasc Electrophysiol 1998; 9: pp. 1186-1195.
5. Cabrera J.A., Sanchez-Quintana D., Ho S.Y., et. al.: Angiographic anatomy of the inferior right atrial isthmus in patients with and without history of common atrial flutter. Circulation 1999; 99: pp. 3017-3023.
6. Heidbuchel H., Willems R., van Rensburg H., et. al.: Right atrial angiographic evaluation of the posterior isthmus: relevance for ablation of typical atrial flutter. Circulation 2000; 101: pp. 2178-2184.
7. Saremi F., Pourzand L., Krishnan S., et. al.: Right atrial cavotricuspid isthmus: anatomic characterization with multi-detector row CT. Radiology 2008; 247: pp. 658-668.
8. Da Costa A., Faure E., Thevenin J., et. al.: Effect of isthmus anatomy and ablation catheter on radiofrequency catheter ablation of the cavotricuspid isthmus. Circulation 2004; 110: pp. 1030-1035.
9. Kirchhof P., Ozgun M., Zellerhoff S., et. al.: Diastolic isthmus length and ‘vertical’ isthmus angulation identify patients with difficult catheter ablation of typical atrial flutter: a pre-procedural MRI study. Europace 2009; 11: pp. 42-47.
10. Komatsu S., Okuyama Y., Omori Y., et. al.: Evaluation of the cavotricuspid isthmus and right atrium by multidetector-row computed tomography in patients with common atrial flutter. Heart Vessels 2005; 20: pp. 264-270.
11. Ozgun M., Kirchhof P., Bunck A.C., et. al.: MRI of right atrial function after catheter ablation of atrial flutter. Acad Radiol 2010; 17: pp. 856-861.
12. Lin D., Kramer C.M.: Late gadolinium-enhanced cardiac magnetic resonance. Curr Cardiol Rep 2008; 10: pp. 72-78.
13. Peters D.C., Wylie J.V., Hauser T.H., et. al.: Detection of pulmonary vein and left atrial scar after catheter ablation with three-dimensional navigator-gated delayed enhancement MR imaging: initial experience. Radiology 2007; 243: pp. 690-695.
14. Dickfeld T., Kato R., Zviman M., et. al.: Characterization of radiofrequency ablation lesions with gadolinium-enhanced cardiovascular magnetic resonance imaging. J Am Coll Cardiol 2006; 47: pp. 370-378.
15. McGann C.J., Kholmovski E.G., Oakes R.S., et. al.: New magnetic resonance imaging-based method for defining the extent of left atrial wall injury after the ablation of atrial fibrillation. J Am Coll Cardiol 2008; 52: pp. 1263-1271.
16. Haber I., Metaxas D.N., Geva T., et. al.: Three-dimensional systolic kinematics of the right ventricle. Am J Physiol Heart Circ Physiol 2005; 289: pp. H1826-H1833.
17. Scott A.D., Keegan J., Firmin D.N.: Motion in cardiovascular MR imaging. Radiology 2009; 250: pp. 331-351.
18. Peukert D., Laule M., Taupitz M., et. al.: 3D and 2D delayed-enhancement magnetic resonance imaging for detection of myocardial infarction: preclinical and clinical results. Acad Radiol 2007; 14: pp. 788-794.
19. Peters D.C., Appelbaum E.A., Nezafat R., et. al.: Left ventricular infarct size, peri-infarct zone, and papillary scar measurements: a comparison of high-resolution 3D and conventional 2D late gadolinium enhancement cardiac MR. J Magn Reson Imaging 2009; 30: pp. 794-800.
20. Kurihara Y., Yakushiji Y.K., Tani I., et. al.: Coil sensitivity encoding in MR imaging: advantages and disadvantages in clinical practice. AJR Am J Roentgenol 2002; 178: pp. 1087-1091.
21. Wang Y., Rossman P.J., Grimm R.C., et. al.: Navigator-echo-based real-time respiratory gating and triggering for reduction of respiration effects in three-dimensional coronary MR angiography. Radiology 1996; 198: pp. 55-60.
22. Judd R.M., Kim R.J.: Imaging time after Gd-DTPA injection is critical in using delayed enhancement to determine infarct size accurately with magnetic resonance imaging. Circulation 2001; 104: pp. 2838-2842.
23. Kim R.J., Shah D.J., Judd R.M.: How we perform delayed enhancement imaging. J Cardiovasc Magn Reson 2003; 5: pp. 505-514.
24. Wagner A., Mahrholdt H., Thomson L., et. al.: Effects of time, dose, and inversion time for acute myocardial infarct size measurements based on magnetic resonance imaging-delayed contrast enhancement. J Am Coll Cardiol 2006; 47: pp. 2027-2033.
25. Desai M.Y., Gupta S., Bomma C., et. al.: The apparent inversion time for optimal delayed enhancement magnetic resonance imaging differs between the right and left ventricles. J Cardiovasc Magn Reson 2005; 7: pp. 475-479.
26. Bland J.M., Altman D.G.: Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986; 1: pp. 307-310.
27. Hripcsak G., Heitjan D.F.: Measuring agreement in medical informatics reliability studies. J Biomed Inform 2002; 35: pp. 99-110.
28. Yokokawa M., Tada H., Koyama K., et. al.: The change in the tissue characterization detected by magnetic resonance imaging after radiofrequency ablation of isthmus-dependent atrial flutter. Int J Cardiol 2009 Nov 8; [Epub ahead of print].
29. Petitjean C., Rougon N., Cluzel P.: Assessment of myocardial function: a review of quantification methods and results using tagged MRI. J Cardiovasc Magn Reson 2005; 7: pp. 501-516.
30. Al-Kwifi O., Stainsby J., Foltz W.D., et. al.: Characterizing coronary motion and its effect on MR coronary angiography—initial experience. J Magn Reson Imaging 2006; 24: pp. 842-850.
31. Kim W.Y., Stuber M., Kissinger K.V., et. al.: Impact of bulk cardiac motion on right coronary MR angiography and vessel wall imaging. J Magn Reson Imaging 2001; 14: pp. 383-390.
32. Shechter G., Resar J.R., McVeigh E.R.: Rest period duration of the coronary arteries: implications for magnetic resonance coronary angiography. Med Phys 2005; 32: pp. 255-262.
33. Wang Y., Vidan E., Bergman G.W.: Cardiac motion of coronary arteries: variability in the rest period and implications for coronary MR angiography. Radiology 1999; 213: pp. 751-758.
34. Sievers B., Rehwald W.G., Albert T.S., et. al.: Respiratory motion and cardiac arrhythmia effects on diagnostic accuracy of myocardial delayed-enhanced MR imaging in canines. Radiology 2008; 247: pp. 106-114.
35. Kim K.A., Seo J.B., Do K.H., et. al.: Differentiation of recently infarcted myocardium from chronic myocardial scar: the value of contrast-enhanced SSFP-based cine MR imaging. Korean J Radiol 2006; 7: pp. 14-19.
36. Themudo R.E., Johansson L., Ebeling-Barbier C., et. al.: Signal intensity of myocardial scars at delayed-enhanced MRI. Acta Radiol 2009; 50: pp. 652-657.
37. Peters D.C., Wylie J.V., Hauser T.H., et. al.: Recurrence of atrial fibrillation correlates with the extent of post-procedural late gadolinium enhancement: a pilot study. JACC Cardiovasc Imaging 2009; 2: pp. 308-316.
38. Reddy V.Y., Schmidt E.J., Holmvang G., et. al.: Arrhythmia recurrence after atrial fibrillation ablation: can magnetic resonance imaging identify gaps in atrial ablation lines?. J Cardiovasc Electrophysiol 2008; 19: pp. 434-437.