
Rationale and Objectives
Vascular calcification independently predicts cardiovascular disease (CVD), and computed tomography (CT) is a useful tool to evaluate and quantify not only coronary but also thoracic aortic calcification (TAC). Previous TAC progression reports were limited to dialysis and renal transplant patients. This is the first study to evaluate TAC progression in a large multiethnic cohort without clinically evident CVD at entry.
Methods
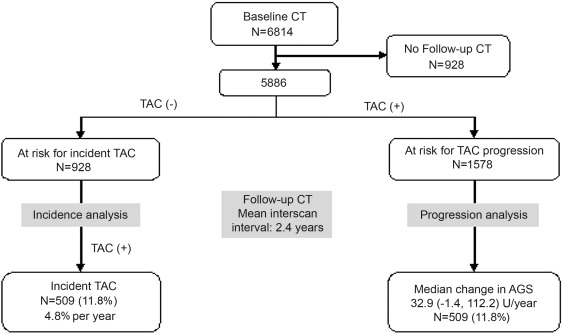
Non–contrast-enhanced cardiac CTs were obtained in 5886 of 6814 Multi-Ethnic Study of Atherosclerosis (MESA) participants (mean age, 62 years; 48% males; 40% white, 27% black, 21% Hispanic, and 12% Chinese). Baseline and follow-up TAC scores were derived.
Results
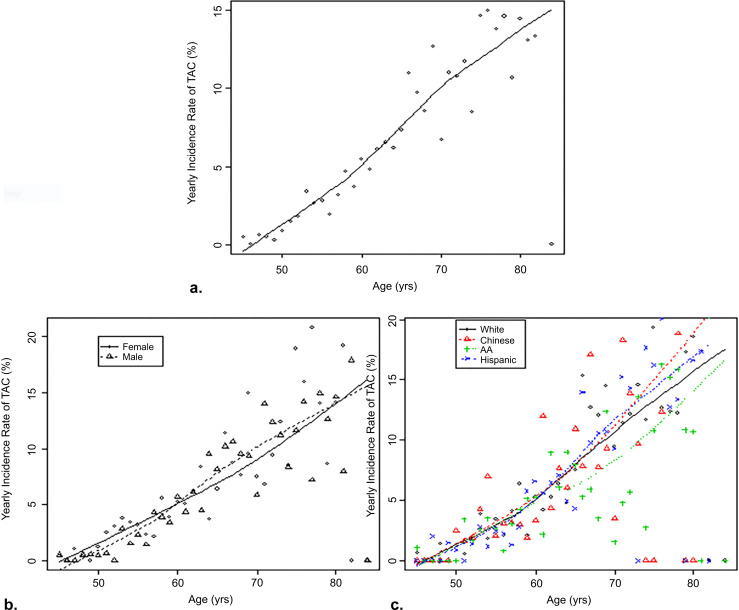
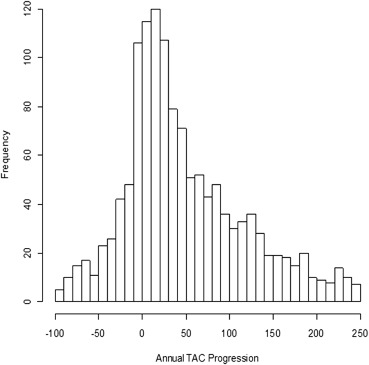
Overall, 4308 (73%) participants had no detectable baseline TAC. Mean follow-up duration was 2.4 ± 0.8 years, during which 12% developed TAC. The overall incidence rate was 4.8%/year and was greater with age across gender and ethnic groups; TAC incidence was significantly lower in blacks than whites. After adjustment for follow-up duration, regression analyses showed age, systolic blood pressure, antihypertensives, and smoking were associated with incident TAC. A total of 1578 (27%) participants had TAC at baseline with a positive association between average annual TAC change and baseline age. Although the overall median change was 32.9 (−1.4 to 112.2) Agatston units, 27% showed an annual score change of ≥100 and blacks showed the lowest median across ethnic groups; 22.7 (−3 to 86.8). Age, systolic blood pressure, lipid-lowering medication, diabetes, and smoking were associated with TAC progression.
Conclusions
In MESA, traditional CV risk factors were related to both TAC incidence and progression. Blacks had the lowest incidence and median change across ethnic groups, consistent with previous findings for coronary calcification.
Vascular calcification has long been a major area of interest in cardiovascular medicine. Intimal calcification, a surrogate marker of atherosclerosis, has been associated with traditional and nontraditional (uremia-related) risk factors and predictive of future cardiovascular events .
Noncontrast computed tomography (CT) is the most sensitive method to quantify vascular calcification. Previous reports from the Multi-Ethnic Study of Atherosclerosis (MESA) study have shown that traditional cardiovascular risk factors were associated with thoracic aortic calcification (TAC) with the highest prevalence in both white and Chinese populations . Moreover, TAC was shown to be a significant predictor of future coronary events in women with increased event rate in symptomatic patients with stable angina . In contrast to coronary artery calcium (CAC) progression, TAC progression reports were limited to dialysis and renal transplant patients. This is the first study to evaluate TAC progression in a large multiethnic cohort without clinically evident clinical cardiovascular disease (CVD) at entry. We evaluated the risk factors associated with both TAC incidence and progression.
Methods
Recruitment and Baseline Examination
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Measurement of TAC
Get Radiology Tree app to read full this article<
Statistical Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Sample Size and Baseline Characteristics
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Baseline Characteristics of Included and Excluded Patients
Variable Included Excluded Mean/Frequency Standard Deviation/Percentage × 100 Mean/Frequency Standard Deviation/Percentage × 100 Age, y 61.83 10.13 64.18 10.61 Systolic BP 125.89 21.02 131.05 23.71 Diastolic BP 71.86 10.17 72.29 10.79 Body mass index 28.33 5.43 28.41 5.79 Packs of cigarettes per year 11.18 22.18 12.82 22.67 LDL cholesterol 117.29 31 116.61 34.3 HDL cholesterol 50.98 14.72 50.85 15.49 Triglycerides 130.89 86.5 136.04 102.16 C-reactive protein 3.67 5.36 4.53 8.48 Gender 0: Female 3087 52.4 514 55.4 1: Male 2799 47.6 414 44.6 Race 1:White 2351 39.9 271 29.2 2:Chinese 686 11.7 117 12.6 3:AA 1584 26.9 309 33.3 4:Hispanic 1265 21.5 231 24.9 Education 1: Less than high school 972 16.6 253 27.5 2: High school 2746 46.8 427 46.4 3: College 1058 18 113 12.3 4: Graduate school 1095 18.7 127 13.8 Hypertension medication No 3750 63.7 525 56.6 Yes 2133 36.3 403 43.4 Lipid-lowering medication No 4925 83.7 786 84.7 Yes 958 16.3 142 15.3 Cigarette smoking 0: Never 2958 50.4 460 50 1: Former 2174 37 313 34 2: Current 740 12.6 147 16 Diabetes Normal 5173 88.1 758 82.3 Treated/untreated diabetes 696 11.9 163 17.7 Family history of heart attack No 3157 57.1 504 58 Yes 2369 42.9 365 42
AA, African American; BP, blood pressure; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Get Radiology Tree app to read full this article<
Incidence Rate for Participants Free of TAC at Baseline
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Association of Traditional CVD Risk Factors and Incidence of TAC
Get Radiology Tree app to read full this article<
Table 2
Relative Risk of Incident Thoracic Aortic Calcium Among Those Free of Thoracic Aortic Calcium at Baseline
Variable Age and Follow-up Time Adjusted Model (n = 4308) Multivariable Model (n = 4252) RR (95% CI)P RR (95% CI)P Follow-up time 1.35 (1.22–1.48) <.001 1.28 (1.16–142) <.001 Age (10 y) 1.91 (1.75–2.08) <.001 1.78 (1.61–1.96) <.001 BMI 1.01 (0.99–1.02) .506 Systolic blood pressure (10 mm Hg) 1.10 (1.06–1.14) <.001 1.11 (1.07–1.15) <.001 Diastolic blood pressure (10 mm Hg) 1.06 (0.98–1.16) .15 LDL-C (10 mg/dL) 1.01 (0.98–1.03) .69 HDL-C (10 mg/dL) 0.98 (0.93–1.04) .50 Log triglycerides (log mg/dL) 1.43 (1.22–1.68) <.001 Fibrinogen (mg/dL) 1.00 (1.00–1.00) .77 Log CRP (log mg/L) 1.03 (0.96–1.11) .37 Male gender 0.90 (0.76–1.06) .21 Race White Reference Chinese 0.95 (0.72–1.25) .716 0.89 (0.66–1.21) .463 African American 0.70 (0.56–0.86) .001 0.6 (0.48–0.74) <.001 Hispanic 0.87 (0.70–1.09) .233 0.88 (0.71–1.09) .236 Education Less than high school Reference High school 0.94 (0.75–1.18) .598 College 0.92 (0.70–1.21) .553 Graduate school 0.94 (0.72–1.24) .659 Income <50,000 Reference 50,000–100,000 1.12 (0.88–1.41) .352 >100,000 0.95 (0.76–1.21) .698 Antihypertensive medication 1.33 (1.12–1.57) .001 1.32 (1.11–1.57) .001 Lipid-lowering medication 1.24 (1–1.52) .046 Diabetes status Normal/impaired fasting glucose Reference Treated/untreated diabetes 1.24 (0.98–1.58) .075 Family history of heart attack 1.01 (0.85–1.2) .944 Creatinine, mg/dL ≤0.9 1.03 (0.82–1.29) .799 1 Reference ≥1.1 0.82 (0.63–1.06) .125 Alcohol Never Reference Former 1.07 (0.83–1.38) .595 Current 1.04 (0.83–1.29) .745 Smoking Never Reference Former 1.02 (0.85–1.24) .808 1.02 (0.85–1.23) .799 Current 1.15 (0.85–1.56) .361 1.28 (0.96–1.72) .094 10 Pack-years of smoking ∗ 1.06 (1.03–1.09) <.001 1.06 (1.03–1.08) <.001
BMI, body mass index; CI, confidence interval; CRP, C-reactive protein; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; RR, relative risk.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Annual TAC Change for Participants with Prevalent TAC at Baseline
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Summary of Average Annual TAC Change (Agatston Score) in Participants with Prevalent TAC at Baseline
Annual TAC Change Women, N (%) Men, N (%) Total, N (%) <0 242 (28.2) 201 (27.9) 443 (28.1) 0–9 43 (5.0) 59 (8.2) 102 (6.5) 10–99 341 (39.8) 263 (36.5) 604 (38.3) 100–199 138 (16.1) 89 (12.3) 227 (14.4) >200 93 (10.9) 109 (15.1) 202 (12.8)
TAC, thoracic aortic calcification.
Table 4
Robust Regression Models for the Change in TAC Over Time Among Participants with Prevalent TAC at Baseline
Variable Robust Regression Model 1 (n = 1578) ∗ Robust Regression Model 2 (n = 1550) Difference in Average Progression (95% CI)P Value Difference in Average Progression_P_ Value Scanner type change EBCT to EBCT Reference EBCT to MDCT −16.8 (−41 to 7.4) .173 −17 (−41.6 to 7.5) .174 MDCT to MDCT −23 (−31.7 to −14.3) <.001 −25.2 (−35.4 to −15) <.001 Follow-up time 18.8 (13.8–23.8) <.001 19.1 (14–24.2) <.001 Age (10 year) 7.9 (2.5–13.3) .004 8.1 (2.4–13.7) .005 BMI 0.3 (−0.6 to 1.2) .512 Systolic blood pressure (10 mm Hg) 2.6 (0.6–4.5) .01 2.6 (0.7–4.6) .009 Diastolic blood pressure (10 mm Hg) 1.6 (−2.6 to 5.7) .465 LDL-C (10 mg/dL) −1.6 (−3 to −0.2) .028 HDL-C (10 mg/dL) −0.3 (−3.3 to 2.7) .838 Log triglycerides (log mg/dL) 4.0 (−4.4 to 12.5) .347 Fibrinogen (mg/dL) 0.1 (0.0–0.1) .048 Log CRP (log mg/L) 2.0 (−1.9 to 5.8) .316 Male gender −2.1 (−10.7 to 6.5) .632 Race White Reference Chinese −9.6 (−24.9 to 5.7) .217 −5.9 (−21.5 to 9.6) .453 African American −9.7 (−21.1 to 1.7) .097 −18.4 (−30.2 to −6.6) .002 Hispanic −14.8 (−27.2 to −2.3) .02 −14.8 (−27.5 to −2) .023 Education Less than high school Reference High school −2.1 (−13.3 to 9) .706 College −9.1 (−23.7 to 5.5) .222 Graduate school −2.7 (−17.6 to 12.2) .723 Income <50,000 Reference 50,000–100,000 3.1 (−8.4 to 14.7) .593 >100,000 3.5 (−8 to 14.9) .551 Antihypertensive medication 5.5 (−3.1 to 14.1) .212 Lipid-lowering medication 19.7 (9.8–29.5) <.001 18.8 (8.8–28.9) <.001 Diabetes status Normal/impaired fasting glucose Reference Treated/untreated diabetes 12.9 (1.2–24.7) .031 15.5 (3.5–27.5) .012 Family history of heart attack 6 (−2.9 to 14.9) .184 Creatinine, mg/dL ≤0.9 −3.9 (−15.3 to 7.6) .505 1 Reference ≥1.1 −7.7 (−20.5 to 5) .236 Alcohol Never Reference Former −3.2 (−15.7 to 9.4) .621 Current −3.4 (−14.1 to 7.4) .54 Smoking Never Reference Former 5.8 (−4.6 to 16.3) .274 7.1 (−3.4 to 17.5) .184 Current 20.6 (4.6–36.6) .012 27 (10.9–43) .001 10 Pack-years of smoking † −0.5 (−2.1 to 1.2) .588 −0.9 (−2.5 to 0.8) .302
BMI, body mass index; CI, confidence interval; CRP, C-reactive protein; EBCT; electron beam computed tomography; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; MDCT, multidetector computed tomography.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Association of Traditional CVD Risk Factors with TAC Progression Among Those with Prevalent TAC at Baseline
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Prevalence and Incidence of TAC
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Progression of TAC
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Strengths and limitations
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Simon A., Levenson J.: Early detection of subclinical atherosclerosis in asymptomatic subjects at high risk for cardiovascular disease. Clin Exp Hypertens 1993; 15: pp. 1069-1076.
2. Wexler L., Brundage B., Crouse J., et. al.: Coronary artery calcification: pathophysiology, epidemiology, imaging methods, and clinical implications. A statement for health professionals from the American Heart Association. Writing Group. Circulation 1996; 94: pp. 1175-1192.
3. Ross R.: The pathogenesis of atherosclerosis: a perspective for the 1990s. Nature 1993; 362: pp. 801-809.
4. Takasu J., Katz R., Nasir K., et. al.: Relationships of thoracic aortic wall calcification to cardiovascular risk factors: the Multi-Ethnic Study of Atherosclerosis (MESA). American heart journal 2008; 155: pp. 765-771.
5. Budoff M.J., Nasir K., Katz R., et. al.: Thoracic aortic calcification and coronary heart disease events: the multi-ethnic study of atherosclerosis (MESA). Atherosclerosis 2011; 215: pp. 196-202.
6. Eisen A., Tenenbaum A., Koren-Morag N., et. al.: Calcification of the thoracic aorta as detected by spiral computed tomography among stable angina pectoris patients: association with cardiovascular events and death. Circulation 2008; 118: pp. 1328-1334.
7. Carr J.J., Nelson J.C., Wong N.D., et. al.: Calcified coronary artery plaque measurement with cardiac CT in population-based studies: standardized protocol of Multi-Ethnic Study of Atherosclerosis (MESA) and Coronary Artery Risk Development in Young Adults (CARDIA) study. Radiology 2005; 234: pp. 35-43.
8. Kronmal R.A., McClelland R.L., Detrano R., et. al.: Risk factors for the progression of coronary artery calcification in asymptomatic subjects: results from the Multi-Ethnic Study of Atherosclerosis (MESA). Circulation 2007; 115: pp. 2722-2730.
9. Okuda K., Kobayashi S., Hayashi H., et. al.: Case-control study of calcification of the hepatic artery in chronic hemodialysis patients: comparison with the abdominal aorta and splenic artery. Journal of gastroenterology and hepatology 2002; 17: pp. 91-95.
10. Rodriguez-Garcia M., Gomez-Alonso C., Naves-Diaz M., et. al.: Vascular calcifications, vertebral fractures and mortality in haemodialysis patients. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association 2009; 24: pp. 239-246.
11. Erbel R., Delaney J.A., Lehmann N., et. al.: Signs of subclinical coronary atherosclerosis in relation to risk factor distribution in the Multi-Ethnic Study of Atherosclerosis (MESA) and the Heinz Nixdorf Recall Study (HNR). European heart journal 2008; 29: pp. 2782-2791.
12. Honkanen E., Kauppila L., Wikstrom B., et. al.: Abdominal aortic calcification in dialysis patients: results of the CORD study. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association 2008; 23: pp. 4009-4015.
13. Bild D.E., Detrano R., Peterson D., et. al.: Ethnic differences in coronary calcification: the Multi-Ethnic Study of Atherosclerosis (MESA). Circulation 2005; 111: pp. 1313-1320.
14. Nasir K., Katz R., Takasu J., et. al.: Ethnic differences between extra-coronary measures on cardiac computed tomography: multi-ethnic study of atherosclerosis (MESA). Atherosclerosis 2008; 198: pp. 104-114.
15. Iribarren C., Sidney S., Sternfeld B., et. al.: Calcification of the aortic arch: risk factors and association with coronary heart disease, stroke, and peripheral vascular disease. JAMA: the journal of the American Medical Association 2000; 283: pp. 2810-2815.
16. Jayalath R.W., Mangan S.H., Golledge J.: Aortic calcification. European journal of vascular and endovascular surgery : the official journal of the European Society for Vascular Surgery 2005; 30: pp. 476-488.
17. Reaven P.D., Sacks J.: Reduced coronary artery and abdominal aortic calcification in Hispanics with type 2 diabetes. Diabetes care 2004; 27: pp. 1115-1120.
18. Matsushita M., Nishikimi N., Sakurai T., et. al.: Relationship between aortic calcification and atherosclerotic disease in patients with abdominal aortic aneurysm. International angiology : a journal of the International Union of Angiology 2000; 19: pp. 276-279.
19. Allison M.A., Criqui M.H., Wright C.M.: Patterns and risk factors for systemic calcified atherosclerosis. Arteriosclerosis, thrombosis, and vascular biology 2004; 24: pp. 331-336.
20. O’Donnell C.J., Chazaro I., Wilson P.W., et. al.: Evidence for heritability of abdominal aortic calcific deposits in the Framingham Heart Study. Circulation 2002; 106: pp. 337-341.
21. Witteman J.C., Grobbee D.E., Valkenburg H.A., et. al.: Cigarette smoking and the development and progression of aortic atherosclerosis. A 9-year population-based follow-up study in women. Circulation 1993; 88: pp. 2156-2162.
22. Owens D.S., Katz R., Takasu J., et. al.: Incidence and progression of aortic valve calcium in the Multi-ethnic Study of Atherosclerosis (MESA). The American journal of cardiology 2010; 105: pp. 701-708.
23. Youssef G., Kalia N., Darabian S., et. al.: Coronary calcium: new insights, recent data, and clinical role. Current cardiology reports 2013; 15: pp. 325.
24. Ryu Y., Yoshida K., Suzuki Y., et. al.: Long-term changes of aortic (18)F-FDG uptake and calcification in health-screening subjects. Annals of nuclear medicine 2012;
25. Noordzij M., Cranenburg E.M., Engelsman L.F., et. al.: Progression of aortic calcification is associated with disorders of mineral metabolism and mortality in chronic dialysis patients. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association 2011; 26: pp. 1662-1669.
26. Marechal C., Coche E., Goffin E., et. al.: Progression of coronary artery calcification and thoracic aorta calcification in kidney transplant recipients. American journal of kidney diseases : the official journal of the National Kidney Foundation 2012; 59: pp. 258-269.
27. Takasu J., Mao S., Budoff M.J.: Aortic atherosclerosis detected with electron-beam CT as a predictor of obstructive coronary artery disease. Academic radiology 2003; 10: pp. 631-637.
28. Budoff M.J., Katz R., Wong N.D., et. al.: Effect of scanner type on the reproducibility of extra-coronary measures of calcification: the Multi-Ethnic Study of Atherosclerosis. Acad Radiol 2007; 14: pp. 1043-1049.
29. Budoff M.J., Young R., Lopez V.A., et. al.: Progression of coronary calcium and incident coronary heart disease events: the Multi-Ethnic Study of Atherosclerosis. J Am Coll Cardiol 2013; 61: pp. 1231-1239.