
Rationale and Objectives
To determine the cancer detection rate and abnormal interpretation rate of screening breast magnetic resonance imaging (MRI) in previously treated breast cancer patients.
Materials and Methods
Institutional review board–approved retrospective review of the breast MRI database from 2009 to 2011 identified a total of 3297 screening examinations. After excluding genetic mutation carriers, untested first-degree relatives of known mutation carriers, and patients with a history of chest irradiation, there were 1194 (36.2%) examinations in 691 patients previously treated for breast cancer. MRI reports were reviewed to determine MRI findings and breast imaging reporting and data system (BI-RADS) assessments. The longitudinal medical record was reviewed to determine patient demographics and outcomes of imaging surveillance and biopsy.
Results
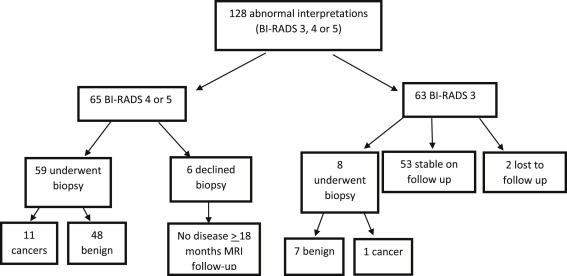
Mean patient age at initial cancer diagnosis was 46.1 years, and mean patient age during the study interval was 52 years. Cancer detection rate was 10 per 1000 (1%; 95% confidence interval [CI], 0.5%–1.8%]; 12 of 1194 examinations). Overall 10.7% (128 of 1194) of examinations received an abnormal interpretation, including 5.4% (65 of 1194) BI-RADS 4 or 5 and 5.3% (63 of 1194) BI-RADS 3 assessments with a 9.4% positive predictive value (PPV1; 12 of 128 examinations) and a 17.9% PPV3 (12 malignancies per 67 biopsies).
Conclusions
Screening breast MRI in women previously treated for breast cancer detected cancer in 1.0% of examinations, with a 10.7% abnormal interpretation rate, and a PPV for malignancy of 17.9%.
Breast magnetic resonance imaging (MRI) is recommended as a supplemental screening examination for women at an increased (at least 20%–25%) lifetime risk of developing breast cancer because of its high sensitivity for the detection of invasive malignancies. Groups recommended for supplemental MRI screening include genetic mutation carriers and first-degree untested relatives of genetic mutation carriers; women with Li-Fraumeni, Cowden, Bannayan-Riley-Ruvalcaba syndromes and their untested first-degree relatives; and women with a history of chest irradiation. Evidence supporting supplemental breast MRI screening has been considered to be insufficient to justify routine MRI surveillance for women with a lesser lifetime risk (15%–20%) of developing breast cancer and for women with a previous history of breast cancer .
Breast cancer survivors remain at risk for recurrent or new breast cancer, and they warrant careful clinical and mammographic follow-up. The 10-year incidence of ipsilateral breast cancer recurrence after lumpectomy and radiation therapy has been reported to be 6.4% in node-negative disease and 8.7% in node-positive disease . In another study reporting 20-year follow-up results in women who had undergone prior breast conservation and radiation therapy, a 14.3% local recurrence rate was reported . Women treated with mastectomy for breast cancer have been reported to develop contralateral breast malignancies ranging from 8.9% to 12% at 20-year follow-up.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Patient Demographics
Get Radiology Tree app to read full this article<
Screen-Detected Malignancies
Get Radiology Tree app to read full this article<
Table 1
Comparison of Women with Cancer-Detected on MRI Compared to Women without Cancer
Demographic Women with Cancer Women without Cancer_P_ Value Family history of breast cancer in first degree relative .19 Positive 5 167 Negative 7 504 Menopausal status at time of diagnosis .53 Premenopausal 7 451 Postmenopausal 5 204 Perimenopausal 21 Mean age at initial breast cancer diagnosis 48.9 years 46.9 years Mean age at MRI screening 56.7 years 53.0 years
BIRADS, breast imaging reporting and data system; MRI, magnetic resonance imaging.
Table 2
Twelve Malignancies Detected on Screening Breast MRI
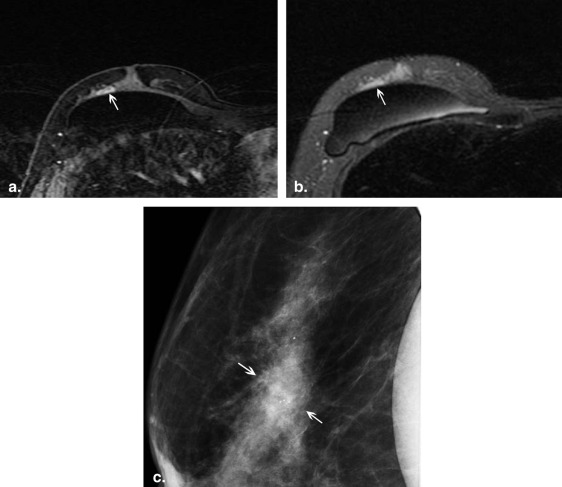
Malignancy Age at Screening MR Diagnosis Age at Initial Cancer Diagnosis Side of Lesion MRI Finding Pathology 1 49 43 Ipsilateral Nonmass enhancement DCIS 2 76 61 Ipsilateral Nonmass enhancement DCIS 3 46 44 Ipsilateral Nonmass enhancement DCIS 4 64 61 Ipsilateral Nonmass enhancement DCIS 5 47 38 Contralateral Mass DCIS 6 48 46 Contralateral Focus IDC, Stage 1A 7 64 59 Ipsilateral Mass IDC 8 26 22 Ipsilateral Mass IDC 9 47 41 Ipsilateral Mass IDC 10 72 41 Ipsilateral Nonmass enhancement IDC 11 59 55 Contralateral Focus IDLC, Stage 1B 12 82 76 Contralateral Mass ILC, Stage 1B
DCIS, ductal carcinoma in situ; IDC, invasive ductal carcinoma; IDLC, invasive ductal and lobular carcinoma; ILC, invasive lobular carcinoma; MRI, magnetic resonance imaging.
Ipsilateral lesions were considered breast cancer recurrences, and therefore, no staging is given.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Abnormal Screening MRI Interpretations
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Saslow D., Boetes C., Burke W., et. al.: American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin 2007; 57: pp. 75-89.
2. Lee C.H., Dershaw D.D., Kopans D., et. al.: Breast cancer screening with imaging: recommendations from the Society of Breast Imaging and the ACR on the use of mammography, breast MRI, breast ultrasound, and other technologies for the detection of clinically occult breast cancer. J Am Coll Radiol 2010; 7: pp. 18-27.
3. Anderson S.J., Wapnir I., Dignam J.J., et. al.: Prognosis after ipsilateral breast tumor recurrence and locoregional recurrences in patients treated by breast-conserving therapy in five national surgical adjuvant breast and bowel project protocols of node-negative breast cancer. J Clin Oncol 2009; 27: pp. 2466-2473.
4. Wapnir I.L., Anderson S.J., Mamounas E.P., et. al.: Prognosis after ipsilateral breast tumor recurrence and locoregional recurrences in five national surgical adjuvant breast and bowel project node-positive adjuvant breast cancer trials. J Clin Oncol 2006; 24: pp. 2028-2037.
5. Fisher B., Anderson S., Bryant J., et. al.: Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med 2002; 347: pp. 1233-1241.
6. Gao X., Fisher S.G., Emami B.: Risk of second primary cancer in the contralateral breast in women treated for early-stage breast cancer: a population-based study. Int J Radiat Oncol Biol Phys 2003; 56: pp. 1038-1045.
7. Houssami N., Abraham L.A., Miglioretti D.L., et. al.: Accuracy and outcomes of screening mammography in women with a personal history of early-stage breast cancer. JAMA 2011; 305: pp. 790-799.
8. Morris E.A., Comstock C., Lee C., et. al.: ACR BI-RADS magnetic resonance imaging 2013.ACR BI-RADS Atlas: Breast Imaging and Reporting and Data System 2013.2013.American College of RadiologyReston, VA:pp. 1-173.
9. Sickles E.A., D’Orsi C.J.: ACR BI-RADS follow-up and outcome monitoring 2013.ACR BI-RADS Atlas: Breast Imaging and Reporting and Data System 2013.2013.American College of RadiologyReston, VA:pp. 1-73.
10. Viehweg P., Heinig A., Lampe D., et. al.: Retrospective analysis for evaluation of the value of contrast-enhanced MRI in patients treated with breast conservation therapy. MAGMA 1998; 7: pp. 141-152.
11. Brennan S., Liberman L., Dershaw D.D., et. al.: Breast MRI screening of women with a personal history of breast cancer. AJR 2010; 195: pp. 510-516.
12. Elmore L., Margenthaler J.A.: Breast MRI surveillance in women with prior curative-intent therapy for breast cancer. J Surg Research 2010; 163: pp. 58-62.
13. Schact D.V., Yamaguchi K., Lai J., et. al.: Importance of a personal history of breast cancer as a risk factor for the development of subsequent breast cancer: results from screening breast MRI. AJR 2014; 202: pp. 289-292.
14. Gweon H.M., Cho N., Han W., et. al.: Breast MR imaging screening in women with a history of breast conservation therapy. Radiology 2014; 272: pp. 366-373.
15. Rosenberg R.D., Yankaskas B.C., Abraham L.A., et. al.: Performance benchmarks for screening mammography. Radiology 2006; 241: pp. 55-66.
16. Breast cancer surveillance consortium, National Cancer Institute. http://breastcancerscreening.cancer.gov/statistics/benchmarks/screening/2009/table6.html . (Accessed on March 3, 2015).
17. Kuhl C.K., Schrading S., Leutner C.C., et. al.: Mammography, ultrasound, and magnetic resonance imaging for surveillance of women at high familial risk of breast cancer. J Clin Oncol 2005; 23: pp. 8469-8476.
18. Warner E., Plewes D.B., Shumak R.S., et. al.: Comparison of breast magnetic resonance imaging, mammography, and ultrasound for surveillance of women at high genetic risk for hereditary breast cancer. J Clin Oncol 2001; 19: pp. 3524-3531.
19. Warner E., Plewes D.B., Hill K.A., et. al.: Surveillance of BRCA1 and BRCA2 mutation carriers with magnetic resonance imaging, ultrasound, mammography, and clinical breast examination. JAMA 2004; 292: pp. 1317-1325.
20. Kriege M., Brekelmans C.T.M., Boetes C., et. al.: Efficacy of MRI and mammography for breast-cancer screening in women with a familial or genetic predisposition. N Engl J Med 2004; 351: pp. 427-437.
21. Kuhl C.: The current status of breast MR imaging: I. Choice of technique, image interpretation, diagnostic accuracy, and transfer to clinical practice. Radiology 2007; 244: pp. 356-378.
22. Lord S.J., Lei W., Craft P., et. al.: A systematic review of the effectiveness of magnetic resonance imaging (MRI) as an addition to mammography and ultrasound in screening young women at high risk of breast cancer. Eur J Cancer 2007; 43: pp. 1905-1917.
23. Moore S.G., Shenoy P.J., Fanucchi L., et. al.: Cost-effectiveness of MRI compared to mammography for breast cancer screening in a high risk population. BMC Health Services Research 2009; 9: pp. 1-8.
24. Pataky R., Armstrong L., Chia S., et. al.: Cost-effectiveness of MRI for breast cancer screening in BRCA ½ mutation carriers. BMC Cancer 2013; 13: pp. 339. published online July 10, 2013
25. Taneja C., Edelsberg J., Weycker D., et. al.: Cost-effectiveness of breast cancer screening with contrast-enhanced MRI in high-risk women. J Am Coll Radiol 2009; 6: pp. 171-179.
26. Reiner A.S., John E.M., Brooks J.D., et. al.: Risk of asynchronous contralateral breast cancer in noncarriers of BRCA 1 and BRCA 2 mutations with a family history of breast cancer: a report from the women’s environmental cancer and radiation epidemiology study. J Clin Oncol 2012; 31: pp. 433-439.
27. Saltzman B.S., Malone K.E., McDougall J.A., et. al.: Estrogen receptor, progesterone receptor and HER2-neu expression in first primary breast cancers and risk of second primary contralateral breast cancer. Breast Cancer Res Treat 2012; 135: pp. 849-855.
28. Kurian A.W., McClure L.A., John E.M., et. al.: Second primary breast cancer occurrence according to hormone receptor status. J Natl Cancer Inst 2009; 101: pp. 1058-1065.
29. Punglia R.S., Hassett M.J.: Using lifetime risk estimates to recommend magnetic resonance imaging screening for breast cancer survivors. J Clin Oncol 2010; 28: pp. 4108-4110.
30. SEER Cancer Statistics Factsheets: Breast Cancer. National Cancer Institute. Bethesda, MD, http://seer.cancer.gov/statfacts/html/breast.html . (Accessed March 5, 2015).