
Rationale and Objectives
To evaluate the potential benefits, harms, and cost-effectiveness of screening for asymptomatic, unruptured intracranial aneurysms in family members of patients with aneurysmal subarachnoid hemorrhage (SAH).
Materials and Methods
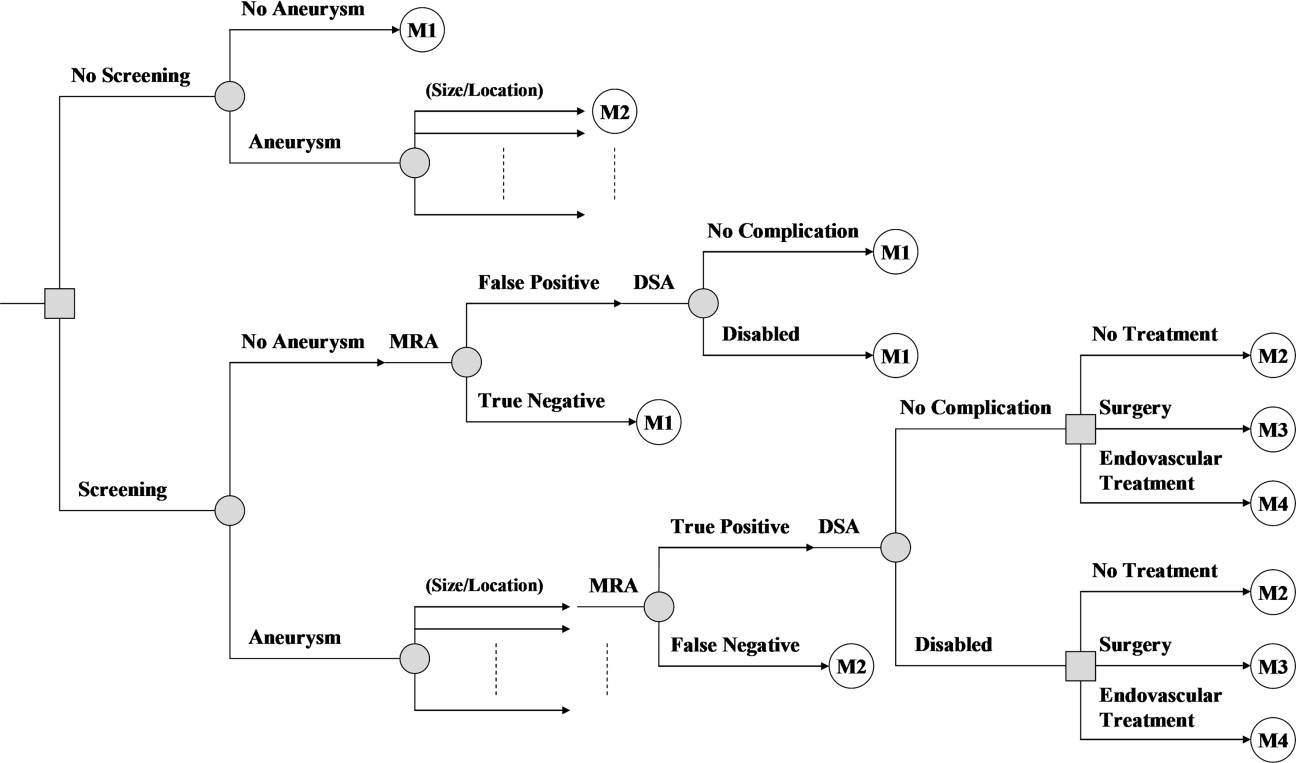
Using a Markov model, we performed a decision and cost-effectiveness analysis comparing magnetic resonance (MR) angiography screening for asymptomatic, unruptured intracranial aneurysms to no screening in family members of patients with aneurysmal SAH. Treatment of unruptured intracranial aneurysms was determined according to patient age and aneurysm size and location. Cohort age was taken as 40 years.
Results
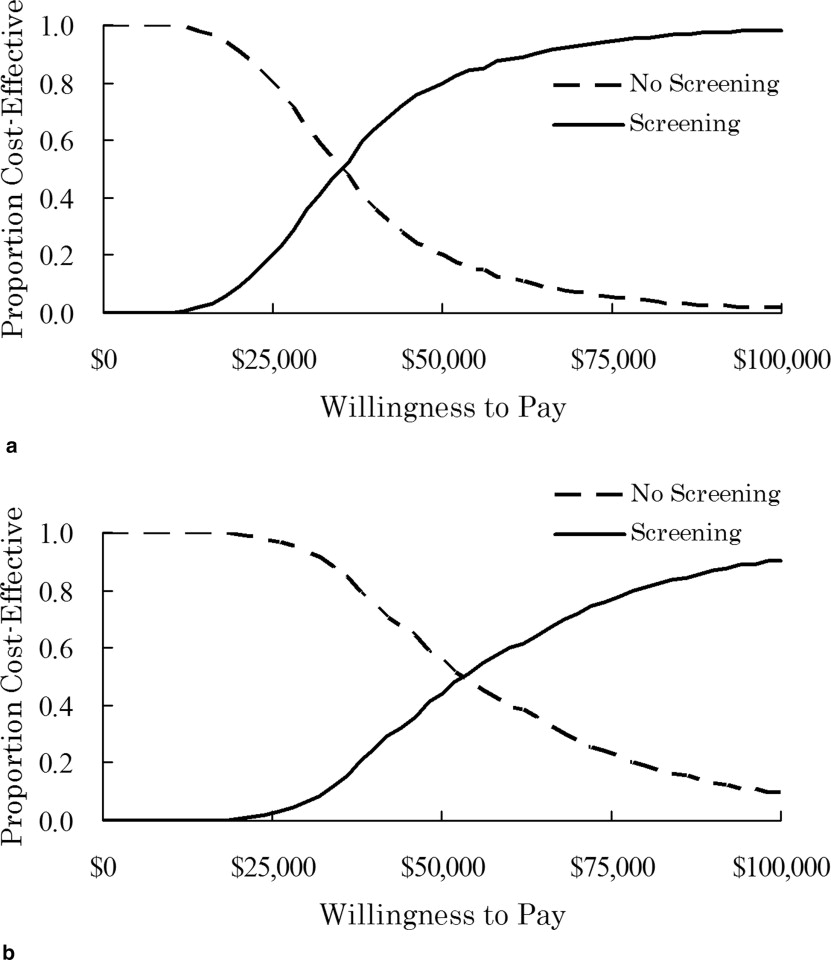
In family members with two or more affected first-degree relatives, screening compared with no screening had an incremental cost-effectiveness ratio (ICER) of $37,400 per quality-adjusted life-year (QALY). With screening, life expectancy increased from 39.44 years to 39.55 years. The ICER of screening was >$50,000 per QALY if age at screening was ≥50 years. In family members with one affected first-degree relative, screening compared with no screening had an ICER of $56,500 per QALY.
Conclusions
The results suggest that MR angiography screening for asymptomatic, unruptured intracranial aneurysms in family members with two or more affected first-degree relatives is cost-effective. The benefit and cost-effectiveness are dependent on age at screening.
Unruptured intracranial aneurysms affects up to 2%–4% of the population ( ). Family members with one or more first-degree relatives with aneurysmal subarachnoid hemorrhage (SAH) have a higher relative risk of harboring an unruptured intracranial aneurysm than the general population ( ). In family members with only one affected first-degree relative, the risk of harboring an unruptured intracranial aneurysm is approximately 4%. Family members with two or more affected first-degree relatives have an approximately 8% risk of harboring an unruptured intracranial aneurysm. The management of patients with unruptured intracranial aneurysms depends on the natural history of these lesions and on morbidity and mortality rates associated with their repair. In 2003, the International Study of Unruptured Intracranial Aneurysms (ISUIA) investigators reported prospective data on the natural history and treatment outcomes of unruptured intracranial aneurysms ( ). Aneurysm rupture rates varied depending on aneurysm size and location and treatment outcomes depended on patient age and aneurysm size and location ( ).
Recommendations regarding screening for asymptomatic, unruptured intracranial aneurysms in family members with one or more affected first-degree relatives are controversial ( ). In 2000, a task force of the Stroke Council of the American Heart Association published recommendations for the management of patients with an unruptured intracranial aneurysm ( ). They concluded that screening in these populations should be considered on an individual basis. Previous decision analyses ( ) showed that there was no benefit of screening for asymptomatic, unruptured intracranial aneurysms in these populations with the assumption that all detected aneurysms were surgically treated. Treatment of unruptured intracranial aneurysms should be determined based on the natural history of these lesions and on morbidity and mortality rates associated with their repair. The purpose of our study was to evaluate the potential benefits, harms, and cost-effectiveness of screening for asymptomatic, unruptured intracranial aneurysms in family members of patients with aneurysmal SAH, incorporating the results of the prospective ISUIA ( ).
Materials and Methods
Study Design
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Probabilities, Costs, and Utilities
Baseline Range Source Age, y 40 30–70 ⁎ Sex Male/Female CDC, 2003 ( ) Probabilities Unruptured intracranial aneurysms Prevalence Meta-analysis ( ) Family members with one affected first-degree relative 4.0% 2.6%–5.8% † Family members with two or more affected first-degree relatives 8.0% 3.9%–14% † Site distribution Meta-analysis ( ) Cavernous carotid artery 8.3% 7.5%–9.2% † ISUIA, 2003 ( ) Anterior circulation 82% 78%–85% † Posterior circulation 10% 7.7%–13% † Size distribution Meta-analysis ( ) <7 mm 72% 68%–77% † 7–12 mm 21% 17%–25% † 13–24 mm 6.5% 4.1%–9.5% † ≥25 mm 0.8% 0.09%–2.8% † MRA Meta-analysis ( ) Sensitivity, <7 mm 92% 88%–96% † ≥7 mm 99% 93%–100% † Specificity 95% 91%–97% † Angiography Meta-analysis ( ) Disability 0.07% 0.01%–0.21% † Aneurysm rupture rates (per year),% ISUIA, 2003 ( ) Cavernous carotid artery <7 mm 0 — 7–12 mm 0 — 13–24 mm 0.6 0.1–2.0 † ≥25 mm 1.3 0.1–5.3 † Anterior communicating or anterior cerebral artery/middle cerebral artery/internal carotid artery <7 mm 0 — 7–12 mm 0.5 0.3–0.9 † 13–24 mm 3.1 2.1–4.4 † ≥25 mm 9.7 6.9–13.3 † Posterior circulation/posterior communicating artery <7 mm 0.5 0.2–1.0 † 7–12 mm 3.1 2.0–4.5 † 13–24 mm 4.0 2.4–6.2 † ≥25 mm 12.9 8.5–18.7 † Background mortality US age/sex specific CDC, 2002 ( ) Relative risks of mortality No disability after SAH Cohort study ( ) Age, 4–39 6.3 4.4–9.0 † Age, 40–54 2.4 1.8–3.2 † Age, >55 1.3 1.0–1.7 † Disability after SAH Cohort study ( ) Age, 4–44 8.7 7.1–10.6 † Age, 45–54 5.4 4.5–6.5 † Age, >55 3.4 2.9–3.8 † Disability from cerebral angiography or treatment of unruptured aneurysms 2.0 1.5–2.5 † Cohort study ( ) SAH Case fatality 0.50 0.32–0.67 Meta-analysis ( ) Case disability 0.15 0.10–0.20 Meta-analysis ( ) Rate of cognitive impairment 50% 41%–58% Cohort study ( ) Surgery ISUIA, 2003 ( ) Poor outcome rates Anterior circulation <13 mm (age <50) 0.06 0.04–0.08 † (age ≥50) 0.12 0.09–0.15 † 13–24 mm (age <50) 0.04 0.02–0.09 † (age ≥50) 0.25 0.19–0.31 † ≥25 mm (age <50) 0.23 0.09–0.44 † (age ≥50) 0.32 0.22–0.44 † Posterior circulation <13 mm (age <50) 0.12 0.05–0.21 † (age ≥50) 0.13 0.06–0.22 † 13–24 mm (age <50) 0.29 0.11–0.54 † (age ≥50) 0.43 0.28–0.60 † ≥25 mm (age <50) 0.44 0.30–0.60 † (age ≥50) — — Poor outcome Death 19% 18%–21% Disability 11% 9%–12% Cognitive impairment 47% 45%–49% Disability with cognitive impairment 23% 21%–25% Posttreatment annual rupture rate 0% Estimate ( ) Endovascular treatment ISUIA, 2003 ( ) Poor outcome rates Anterior circulation <13 mm (age <50) 0.07 0.03–0.15 † (age ≥50) 0.07 0.03–0.12 † 13–24 mm (age <50) 0.05 0.01–0.15 † (age ≥50) 0.08 0.04–0.15 † ≥25 mm (age <50) 0.16 0.03–0.43 † (age ≥50) 0.13 0.06–0.25 † Posterior circulation <13 mm (age <50) 0.11 0.03–0.28 † (age ≥50) 0.08 0.02–0.19 † 13–24 mm (age <50) 0.17 0.01–0.59 † (age ≥50) 0.23 0.10–0.42 † ≥25 mm (age <50) — — (age ≥50) 0.40 0.23–0.60 † Poor outcome Death 33% 28%–37% Disability 9% 7%–12% Cognitive impairment 37% 33%–42% Disability with cognitive impairment 21% 17%–25% Posttreatment relative risk of rupture 0.39 0.28–0.49 ‡ Estimate ( ) Posttreatment annual rupture rate Rupture rate × relative risk of rupture Estimate ( ) Costs, $ MRA 560 390–770 † ‡ Medicare ( ) Angiography 1,400 1,000–2,000 † ‡ Medicare ( ) Surgery 30,000 21,000–42,000 † ‡ Cohort study ( ) Endovascular treatment 25,000 17,000–34,000 † ‡ Cohort study ( ) SAH 59,000 42,000–82,000 † ‡ Cohort study ( ) Disability (annual) 25,000 18,000–35,000 † ‡ Cohort study ( ) Utilities Disability 0.26 0.11–0.39 Meta-analysis ( ) Quality reduction Cognitive impairment 50% 30%–70% ‡ Estimate ( ) Treatment of unruptured aneurysms (3 months) 75% 0%–100% ⁎ ‡ Estimate ( ) SAH (3 months) 0% 0%–100% ⁎ ‡ Estimate ( ) Knowingly living with unruptured aneurysm 0.95 § 0.90–1.00 ‡ Estimate ( )
ISUIA: International Study of Unruptured Intracranial Aneurysms; CDC: Centers for Disease Control and Prevention; MRA: magnetic resonance angiography; SAH: subarachnoid hemorrhage.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
The Markov Model and Its Transition Probabilities
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Costs
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Quality of Life
Get Radiology Tree app to read full this article<
Outcome Measures
Get Radiology Tree app to read full this article<
Analyses
Get Radiology Tree app to read full this article<
Results
Base-Case Analysis
Get Radiology Tree app to read full this article<
Table 2
Effectiveness, Cost, and Cost-effectiveness Compared with No Screening (40-Year-Old Cohorts)
QALYs Cost, $ Incremental cost per QALY, $ Average Incremental Average Incremental Family members with two or more affected first-degree relatives (base case) No screening 22.40 590 Screening 22.43 0.04 1,900 1,300 37,400 Family members with one affected first-degree relative No screening 22.44 290 Screening 22.45 0.02 1,300 1,000 56,500
QALY: quality-adjusted life-year.
Get Radiology Tree app to read full this article<
Sensitivity Analyses
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Rinkel G.J.E., Djibuti M., Algra A., et. al.: Prevalence and risk of rupture of intracranial aneurysms: a systematic review. Stroke 1998; 29: pp. 251-256.
2. Rinkel G.J.E.: Intracranial aneurysm screening: indications and advice for practice. Lancet Neurol 2005; 4: pp. 122-128.
3. International Study of Unruptured Intracranial Aneurysms Investigators: Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet 2003; 362: pp. 103-110.
4. Bederson J.B., Awad I.A., Wiebers D.O., et. al.: Recommendations for the management of patients with unruptured intracranial aneurysms: a statement for healthcare professionals from the Stroke Council of the American Heart Association. Stroke 2000; 31: pp. 2742-2750.
5. Crawley F., Clifton A., Brown M.M.: Should we screen for familial intracranial aneurysm?. Stroke 1999; 30: pp. 312-316.
6. The Magnetic Resonance Angiography in Relatives of Patients with Subarachnoid Hemorrhage Study Group: Risks and benefits of screening for intracranial aneurysms in first-degree relatives of patients with sporadic subarachnoid hemorrhage. N Engl J Med 1999; 341: pp. 1344-1350.
7. Doubilet P., Begg C.B., Weinstein M.C., et. al.: Probabilistic sensitivity analysis using Monte Carlo simulation: a practical approach. Med Decis Making 1985; 5: pp. 157-177.
8. Takao H., Nojo T.: Treatment of unruptured intracranial aneurysms: decision and cost-effectiveness analysis. Radiology 2007; 244: pp. 755-766.
9. White P.M., Wardlaw J.M., Easton V.: Can noninvasive imaging accurately depict intracranial aneurysms?. Radiology 2000; 217: pp. 361-370.
10. Cloft H.J., Joseph G.J., Dion J.E.: Risk of cerebral angiography in patients with subarachnoid hemorrhage, cerebral aneurysm, and arteriovenous malformation: a meta-analysis. Stroke 1999; 30: pp. 317-320.
11. Vindlacheruvu R.R., Mendelow A.D., Mitchell P.: Risk-benefit analysis of the treatment of unruptured intracranial aneurysms. J Neurol Neurosurg Psychiatry 2005; 76: pp. 234-239.
12. Mitchell P., Gholkar A., Vindlacheruvu R.R., et. al.: Unruptured intracranial aneurysms: benign curiosity or ticking bomb?. Lancet Neurol 2004; 3: pp. 85-92.
13. US Department of Health and Human Services, Centers for Disease Control and Prevention: http://www.cdc.gov Accessed February 15, 2006
14. Johnston S.C., Gress D.R., Kahn J.G.: Which unruptured cerebral aneurysms should be treated?. Neurology 1999; 52: pp. 1806-1815.
15. Hop J.W., Rinkel G.J.E., Algra A., et. al.: Case-fatality rates and functional outcome after subarachnoid hemorrhage: a systemic review. Stroke 1997; 28: pp. 660-664.
16. Mayer S.A., Kreiter K.T., Copeland D., et. al.: Global and domain-specific cognitive impairment and outcome after subarachnoid hemorrhage. Neurology 2002; 59: pp. 1750-1758.
17. Kreiter K.T., Copeland D., Bernardini G.L., et. al.: Predictors of cognitive dysfunction after subarachnoid hemorrhage. Stroke 2002; 33: pp. 200-209.
18. Ronkainen A., Niskanen M., Rinne J., et. al.: Evidence for excess long-term mortality after treated subarachnoid hemorrhage. Stroke 2001; 32: pp. 2850-2853.
19. Strauss D.J., Shavelle R.M., Anderson T.W.: Long-term survival of children and adolescents after traumatic brain injury. Arch Phys Med Rehabil 1998; 79: pp. 1095-1100.
20. Wiebers D.O.: Patients with small, asymptomatic, unruptured intracranial aneurysms and no history of subarachnoid hemorrhage should generally be treated conservatively. Stroke 2005; 36: pp. 408-409.
21. Post P.N., Kievit J., van Baalen J.M., et. al.: Routine duplex surveillance does not improve the outcome after carotid endarterectomy: a decision and cost utility analysis. Stroke 2002; 33: pp. 749-755.
22. Gage B.F., Cardinalli A.B., Albers G.W., et. al.: Cost-effectiveness of warfarin and aspirin for prophylaxis of stroke in patients with nonvalvular atrial fibrillation. JAMA 1995; 274: pp. 1839-1845.
23. US Department of Labor, Bureau of Labor Statistics: http://www.bls.gov Accessed March 6, 2006
24. Huang J.: van Gelder JM. Neurosurgery 2002; 51: pp. 1101-1107.
25. Post P.N., Stiggelbout A.M., Wakker P.P.: The utility of health states after stroke: a systematic review of the literature. Stroke 2001; 32: pp. 1425-1429.
26. Aoki N., Beck J.R., Kitahare T., et. al.: Reanalysis of unruptured intracranial aneurysm management: effect of a new international study on the threshold probabilities. Med Decis Making 2001; 21;: pp. 87-96.
27. King J.T., Glick H.A., Mason T.J., et. al.: Elective surgery for asymptomatic, unruptured, intracranial aneurysms: a cost-effectiveness analysis. J Neurosurg 1995; 83: pp. 403-412.
28. Hunink M.G.M., Glasziou P.P., Siegel J.E., et. al.: Decision making in health and medicine: integrating evidence and values.2001.Cambridge University PressCambridge
29. Gold M.R., Siegel J.E., Russell L.B., et. al.: Cost-effectiveness in health and medicine.1996.Oxford University PressNew York
30. Drummond M.F., Sculpher M.J., Torrance G.W., et. al.: Methods for the economic evaluation of health care programmes.2005.Oxford University PressNew York
31. TreeAge Pro 2006 user’s manual.2006.TreeAge Software, IncWilliamstown, MA
32. Yoshimoto Y., Wakai S.: Cost-effectiveness analysis of screening for asymptomatic, unruptured intracranial aneurysms: a mathematical model. Stroke 1999; 30: pp. 1621-1627.
33. Butler W.E., Barker F.G., Crowell R.M.: Patients with polycystic kidney disease would benefit from routine magnetic resonance angiographic screening for intracranial aneurysms: a decision analysis. Neurosurgery 1996; 38: pp. 506-516.
34. Wermer M.J.H., Buskens E., van der Schaaf I.C., et. al.: Yield of screening for new aneurysms after treatment for subarachnoid hemorrhage. Neurology 2004; 62: pp. 369-375.