
Rationale and Objectives
Severe reactions to radiographic contrast agents can be life threatening, and although they are rare, effective recognition and management are essential to improving outcomes. A high-fidelity radiology simulation course for radiology residents and technologists focusing on severe contrast reactions and immediate treatments was designed to test the hypothesis that knowledge would improve with this educational intervention.
Materials and Methods
A prospective pretest and posttest study design was used. Residents and technologists worked in teams of three to five members. Learning objectives focused on demonstrating when and how to use basic life support skills and epinephrine auto-injectors. Each resident and technologist was administered a pretest prior to the start of the case scenarios and a posttest following the debriefing session. Scores from the pretest and posttest for the residents and technologists were compared using a paired-samples t test.
Results
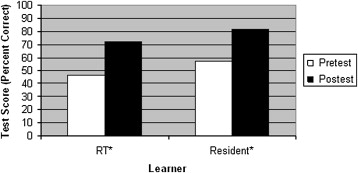
Nineteen radiology residents and 11 radiology technologists participated. The average test scores were higher and improved significantly following the simulation experience for both the radiology residents (57% vs 82%, P < .001) and technologists (47% vs 72%, P = .006). Anonymous evaluations demonstrated that the experience was well received by residents and technologists, with 97% of learners (29 of 30) rating the experience as extremely or very helpful. Important learning themes included the knowledge of epinephrine auto-injector use and basic life support skills.
Discussion
High-fidelity simulation for radiology residents and technologists focusing on epinephrine auto-injector use and basic life support skills during the first 5 minutes of a severe contrast reaction can significantly improve recognition and knowledge in treating patients having severe contrast reactions.
Severe reactions to intravenous radiographic contrast agents are rare events. A recent large-scale study of >12,000 consecutive nonionic iodinated intravenous contrast injections at a tertiary children’s hospital reported no severe reactions . Many large-scale studies of acute allergic-like reactions to intravenous gadolinium agents have report similarly low rates of severe reactions ≤0.1% . Nevertheless, these reactions must be quickly and effectively managed to ensure the best chance for survival. Many radiology residents and attending radiologists prepare for these emergencies by taking advanced cardiac life support (ACLS) or pediatric advanced life support courses. These curricula are dedicated to teaching the acute recognition and management of a broad set of patient problems, such as myocardial infarction or septic shock. The majority of the curricula is unlikely to be applicable to a radiologist. Finally, there is literature documenting the rapid decay of skills and knowledge in internal medicine and pediatric residents after participation in ACLS and pediatric advanced life support courses . Because radiology residents tend to use resuscitation skills less often than internal medicine and pediatric residents, it would be expected that radiology residents have an equal or greater decline in these skills.
Alternative forms of emergency training, such as high-fidelity simulation scenarios depicting contrast reaction events, may improve radiologists’ long-term performance during rare emergency events. High-fidelity simulation is gaining acceptance as an effective tool to train medical personnel in many disciplines. Indeed, simulation training has acquired applications in laparoscopic surgery, ophthalmology, emergency medicine, obstetrics and gynecology, pediatrics, and other high-acuity settings . Simulation training provides a safe and controlled environment and allows time for learners to reflect on their actions.
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Demographics of Radiology Residents and RTs Regarding Experience with Codes and Contrast Reactions
Variable Residents ∗ RTs Postgraduate year (residents) 2 5 (26%) 3 4 (21%) 4 5 (26%) 5 5 (26%) Experience (RTs) (y) 13 ± 6.5 Number of codes experienced 0–2 15 (79%) 6 (66%) 2–5 1 (5%) 1 (11%) 6–10 2 (10%) 1 (11%) >10 1 (5%) 1 (11%) Number of potentially life threatening contrast reactions 0–2 19 (100%) 6 (66%) 2–5 0 (0%) 3 (33%) Certifications BLS 13 (68%) 9 (100%) ACLS 19 (100%) 0 (0%) PALS 0 (0%) 0 (0%)
ACLS, advanced cardiac life support; BLS, basic life support; PALS, pediatric advanced life support; RT, radiology technologist.
Data are expressed as number (percentage) or as mean ± SD.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Appendix
Identification Number __________
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Callahan M.J., Poznauskis L., Zurakowski D., et. al.: Nonionic iodinated intravenous contrast material–related reactions: incidence in large urban children’s hospital—retrospective analysis of data in 12 494 patients. Radiology 2009; 250: pp. 674-681.
2. Dillman J.R., Ellis J.H., Cohan R.H., et. al.: Frequency and severity of acute allergic-like reactions to gadolinium-containing IV contrast media in children and adults. AJR Am J Roentgenol 2007; 189: pp. 1533-1538.
3. Chamberlain D., Smith A., Wollard M., et. al.: Trials of teaching method in basic life support: comparison of simulated CPR performance after training and at 6 months with a note on the value of retraining. Resuscitation 2002; 53: pp. 179-187.
4. Grant E.R., Marczinski C.A., Menon K.: Using pediatric advanced life support in pediatric residency training: does the curriculum need resuscitation?. Pediatr Crit Care Med 2007; 8: pp. 433-439.
5. Wolfram R.W., Warren C.M., Doyle C.R., et. al.: Retention of pediatric advanced life support (PALS) course concepts. J Emerg Med 2003; 25: pp. 475-479.
6. Kaye W., Mancini M.E., Rallis S.F.: Advanced cardiac life support refresher course using standardized objective-based mega code testing. Crit Care Med 1987; 15: pp. 55-60.
7. Solverson D.J., Mazzoli R.A., Raymond W.R., et. al.: Virtual reality simulation in acquiring and differentiating basic ophthalmic microsurgical skills. Simul Healthc 2009; 4: pp. 98-103.
8. Gurusamy K., Aggarwal R., Palanivelu L., et. al.: Systematic review of randomized controlled trials on the effectiveness of virtual reality training for laparoscopic surgery. Br J Surg 2008; 95: pp. 1088-1097.
9. Nishisaki A., Hales R., Biagag K., et. al.: A multi-institutional high-fidelity simulation “boot camp” orientation and training program for first year pediatric critical care fellows. Pediatr Crit Care Med 2009; 10: pp. 157-162.
10. Robertson B., Schumacher L., Gosman G., et. al.: Simulation-based crisis team training for multidisciplinary obstetric providers. Simul Healthc 2009; 4: pp. 77-83.
11. Lammers R.L., Byrwa M.J., Fales W.D., et. al.: Simulation-based assessment of paramedic pediatric resuscitation skills. Prehosp Emerg Care 2009; 13: pp. 345-356.
12. Weinberg E.R., Auerbach M.A., Shah N.B.: The use of simulation for pediatric training and assessment. Curr Opin Pediatr 2009; 21: pp. 282-287.
13. McLaughlin S., Fitch M.T., Goyal D.G., et. al.: Simulation in graduate medical education 2008: a review for emergency medicine. Acad Emerg Med 2008; 15): pp. 117-129.
14. Rudolph J.W., Simon R., Dufresne R.L., et. al.: There’s no such thing as “nonjudgmental” debriefing: a theory and method for debriefing with good judgment. Simul Healthc 2006; 1: pp. 49-55.
15. Sampson H.A., Munoz-Furlong A., Campbell R.L., et. al.: Second symposium on the definition and management of anaphylaxis: summary report. J Allergy Clin Immunol 2006; 117: pp. 391-397.
16. American Heart Association: Pediatric advanced life support manual.2002.American Heart AssociationDallas, TX
17. Gaca A.M., Frush D.P., Hohenhaus S.M., et. al.: Enhancing pediatric safety: using simulation to assess radiology resident preparedness for anaphylaxis from intravenous contrast media. Radiology 2007; 245: pp. 236-244.
18. Lerner C., Gaca A.M., Frush D.P., et. al.: Enhancing pediatric safety: assessing and improving resident competency in life-threatening events with a computer-based interactive resuscitation tool. Pediatr Radiol 2009; 39: pp. 703-709.
19. Sica G.T., Barron D.M., Blum R., et. al.: Computerized realistic simulation: a teaching module for crisis management in radiology. AJR Am J Roentgenol 1999; 172: pp. 301-304.
20. Knowles M.S., Holton E.F., Swanson R.A.: The adult learner.1998.Butterworth-HeinemannWoburn, MA
21. Kolb D.A.: Experiential learning: experience as the source of learning and development.1984.Prentice-HallEnglewood Cliffs, NJ
22. Hallinan J.T.: Why we make mistakes.2009.Broadway BooksNew York
23. Edgar D.: Audio-visual methods in teaching.1954.Dryden PressHinsdale, IL
24. Marteau T.M., Wynne G., Kaye W., et. al.: Resuscitation: experience without feedback increases confidence but not skill. BMJ 1990; 300: pp. 849-850.
25. Lightfoot C.B., Abraham R.J., Mammen T., et. al.: Survey of radiologists’ knowledge regarding the management of severe contrast material induced allergic reactions. Radiology 2009; 251: pp. 691-696.
26. Simons F.E., Lieberman P.L., Read E.J., et. al.: Hazards of unintentional injection of epinephrine from autoinjectors: a systemic review. Ann Allergy Asthma Immunol 2009; 102: pp. 282-287.
27. Grouhi M., Alshehri M., Hummel D., et. al.: Anaphylaxis and epinephrine auto-injector training: who will teach the teachers?. J Allergy Clin Immunol 1999; 104: pp. 190-193.
28. Marsch S.C., Tschan F., Semmer N., et. al.: Performance of first responders in simulated cardiac arrests. Crit Care Med 2005; 33: pp. 963-967.
29. Hunt E.A., Walker A.R., Shaffner D.H., et. al.: Simulation of in-hospital pediatric medical emergencies and cardiopulmonary arrests: highlighting the importance of the first 5 minutes. Pediatrics 2008; 121: pp. e34-e43.
30. Gordon J.A., Wilkerson W.M., Shaffer D.W., et. al.: “Practicing” medicine without risk: students’ and educators’ responses to high-fidelity patient simulation. Acad Med 2001; 76: pp. 469-472.
31. Anderson J.M., Boyle K.B., Murphy A.A., et. al.: Simulating extracorporeal membrane oxygenation emergencies to improve human performance. Part I: methodologic and technologic innovation. Simul Healthc 2006; 1: pp. 220-232.
32. Joint Commission. Root causes for sentinel events, 2006. Available at: http://www.jointcommission.org/sentinel events/statistics . Accessed December 30, 2009.
33. Salas E., DiazGranados D., Weaver S.J., et. al.: Does team training work? Principles for health care. Acad Emerg Med 2008; 15: pp. 1002-1009.