
Rationale and Objectives
We aimed to investigate the diagnostic accuracy with which shear wave elastography (SWE) can be used to monitor response to treatment of tendinopathies, and to compare it to conventional ultrasound (US)-imaging methods (B-mode US (B-US) and power Doppler US (PD-US)).
Materials and Methods
A prospective Institutional Review Board-approved longitudinal study on 35 patients with 47 symptomatic tendons (17 Achilles-, 15 patellar-, and 15 humeral-epicondylar) who underwent standardized multimodal US and standardized clinical assessment before and after 6 months of treatment (tailored stretching exercise, sport break, and local Polidocanol) was carried out. All US studies were performed by radiologists blinded to the clinical symptoms on both tendon sides to avoid biased interpretations, by B-US, PD-US, and SWE, conducted in the same order, using a high-resolution linear 15 MHz probe (Aixplorer). Orthopedic surgeons who were in turn blinded to US imaging results used established orthopedic scores (Victorian Institute of Sports Assessment questionnaire for Achilles, Victorian Institute of Sports Assessment questionnaire for patellar tendons, and Disability Arm Shoulder Hand scoring system) to rate presence, degree, and possible resolution of symptoms. We analyzed the diagnostic accuracy with which the different US imaging methods were able to detect symptomatic tendons at baseline as well as treatment effects, with orthopedic scores serving as reference standard.
Results
B-US, PD-US, and SWE detected symptomatic tendons with a sensitivity of 66% (31 of 47), 72% (34 of 47), and 87.5% (41 of 47), respectively. Positive predictive value was 0.67 for B-US, 0.87 for PD-US, and 1 for SWE. After treatment, clinical scores improved in 68% (32 of 47) of tendons. Treatment effects were observable by B-US, PD-US, and SWE with a sensitivity of 3.1% (1 of 32), 28.1% (9 of 32), and 81.3% (26 of 32), respectively. B-US was false-positive in 68.8% (20 of 32), PD-US in 46.9% (15 of 32), and SWE in 12.5% (4 of 32) (SWE). Clinical scores and B-US, PD-US, and SWE findings correlated poorly (r = 0.24), moderately (r = 0.59), and strongly (r = 0.80).
Conclusion
Unlike B-US or PD-US, SWE is able to depict processes associated with tendon healing and may be a useful tool to monitor treatment effects.
Introduction
Tendinopathies of Achilles, patellar, or epicondylar tendons, characterized by pain, swelling, or function, are some of the most common orthopedic conditions, not only in sportsmen or athletes , but also in individuals with sedentary lifestyle .
To date, B-mode ultrasound (B-US), power Doppler ultrasound (PD-US), and magnetic resonance imaging (MRI) are the main diagnostic tools in detecting and monitoring tendinopathies . Typical US detectable changes, such as tendon thickening, inhomogeneous tendon structure, loss of echogenicity, and hypervascularization are known to be imaging signs associated with or indicative of tendinopathy .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Study Design and Population
Get Radiology Tree app to read full this article<
Inclusion Criteria
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Clinical Assessment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Tendinopathy Treatment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Imaging Protocol
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
B-Mode Ultrasound (B-US)
Get Radiology Tree app to read full this article<
Power Doppler Ultrasound (PD-US)
Get Radiology Tree app to read full this article<
Shear Wave Elastography (SWE)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Demographics of Symptomatic Participants at Baseline ( n = 47)
All ( n = 47) Achilles Tendon ( n = 17) Patellar Tendon ( n = 15) Humeral Epicondylar Tendon ( n = 15)Age (years) Mean ± SD 46 ± 18 50 ± 13 26 ± 5 49 ± 15 Median/range 45/20–71 49/31–69 30/20–40 43/24–70Sex Male 37 (78.7%) 11 (64.7%) 15 (100%) 11 (73.3%) Female 10 (23.4%) 6 (35.3%) 0 (0%) 4 (26.7%)Clinical score VISA-A score VISA-P score DASH score \* Baseline (Mean/SD) 40 ± 20 54 ± 16 38 ± 15 48 ± 12
DASH, Disability Arm Shoulder Hand scoring system; SD, standard deviation; VISA-A, Victorian Institute of Sports Assessment questionnaire for Achilles; VISA-P, Victorian Institute of Sports Assessment questionnaire for patellar tendons.
Get Radiology Tree app to read full this article<
Table 2
Imaging Findings in Symptomatic Tendons at Baseline and After 6 Months of Therapy ( n = 47)
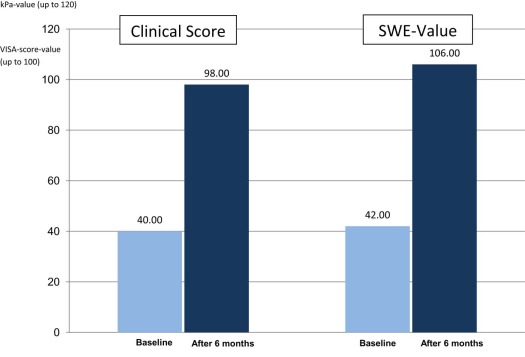
Baseline 6 Months Following Treatment Measureable Improvement_P_ Value Clinical score 40 ± 20 98 ± 17 +245% <.01 SWE score (kPa) 42 ± 15 106 ± 27 +152.4% <.01 Symptomatic tendons 47/47 (100%) 15/47 (31.9%) +68.1% <.01 Positive B-mode US 31/47 (66%) 29/47 (61.7%) +4.3% >.05 Positive PD-US 34/47 (72.3%) 25/47 (53.2%) +26.5% >.05 Positive SWE 41/47 (87%) 6/47 (12.8%) +85.4% <.01
B-mode US, B-mode ultrasound; PD-US, power Doppler ultrasound; SWE, shear wave elastography.
Get Radiology Tree app to read full this article<
Baseline (Pretreatment) Findings
Clinical Scores
Get Radiology Tree app to read full this article<
Ultrasound Findings
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
After 6 Months of Treatment
Clinical Scores
Get Radiology Tree app to read full this article<
B-Mode Ultrasound
Get Radiology Tree app to read full this article<
Power Doppler Ultrasound
Get Radiology Tree app to read full this article<
Shear Wave Elastography
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Sensitivity/Specificity of Different Modalities Prior to and 6 Months After Initiating Tendinopathy Treatment
Baseline 6 Months Following Treatment Modality SENS SPEC PPV NPV SENS SPEC PPV NPV B-mode 0.66 0.83 0.67 0.58 0.05 0.31 0.3 0.13 Power Doppler 0.72 0.79 0.87 0.65 0.47 0.53 0.32 0.32 SWE 0.87 1 1 0.83 0.81 0.88 0.75 0.57
NPV, negative predictive value; PPV, positive predictive value; SENS, sensitivity; SPEC, specificity; SWE, shear wave elastography.
Get Radiology Tree app to read full this article<
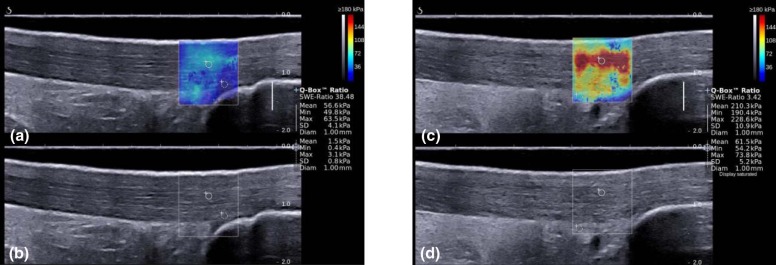
Quantitative Tendon Assessment by SWE
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Maffulli N., Sharma P., Luscombe K.L.: Achilles tendinopathy: aetiology and management. J R Soc Med 2004; 97: pp. 472-476.
2. Cassel M., Baur H., Hirschmüller A., et. al.: Prevalence of Achilles and patellar tendinopathy and their association to intratendinous changes in adolescent athletes. Scand J Med Sci Sports 2015; 25: pp. 310-318.
3. Ames P.R., Longo U.G., Denaro V., et. al.: Achilles tendon problems: not just an orthopaedic issue. Disabil Rehabil 2008; 30: pp. 1646-1650.
4. Mahoney J.M.: Imaging techniques and indications. Clin Podiatr Med Surg 2017; 34: pp. 115-128.
5. Gaulke R., Krettek C.: Tendinopathies of the foot and ankle: evidence for the origin, diagnostics and therapy. Unfallchirurg 2017; 120: pp. 205-213.
6. de Jonge S., van den Berg C., de Vos R.J., et. al.: Incidence of midportion Achilles tendinopathy in the general population. Br J Sports Med 2011; 45: pp. 1026-1028.
7. Ohberg L., Alfredson H.: Ultrasound guided sclerosis of neovessels in painful chronic Achilles tendinosis: pilot study of a new treatment. Br J Sports Med 2002; 36: pp. 173-175.
8. Pingel J., Lu Y., Starborg T., et. al.: 3-D ultrastructure and collagen composition of healthy and overloaded human tendon: evidence of tenocyte and matrix buckling. J Anat 2014; 224: pp. 548-555.
9. Notarnicola A., Maccagnano G., Di Leo M., et. al.: Overload and neovascularization of Achilles tendons in young artistic and rhythmic gymnasts compared with controls: an observational study. Musculoskelet Surg 2014; 98: pp. 115-120.
10. Visnes H., Tegnander A., Bahr R.: Ultrasound characteristics of the patellar and quadriceps tendons among young elite athletes. Scand J Med Sci Sports 2015; 25: pp. 205-215.
11. Comin J., Cook J.L., Malliaras P., et. al.: The prevalence and clinical significance of sonographic tendon abnormalities in asymptomatic ballet dancers: a 24-month longitudinal study. Br J Sports Med 2013; 47: pp. 89-92.
12. Klauser A.S., Miyamoto H., Tamegger M., et. al.: Achilles tendon assessed with sonoelastography: histologic agreement. Radiology 2013; 267: pp. 837-842.
13. Lehtinen A., Peltokallio P., Taavitsainen M.: Sonography of Achilles tendon correlated to operative findings. Ann Chir Gynaecol 1994; 83: pp. 322-327.
14. Khan K.M., Forster B.B., Robinson J., et. al.: Are ultrasound and magnetic resonance imaging of value in assessment of Achilles tendon disorders? A two year prospective study. Br J Sports Med 2003; 37: pp. 149-153.
15. Paavola M., Paakkala T., Kannus P., et. al.: Ultrasonography in the differential diagnosis of Achilles tendon injuries and related disorders: a comparison between pre-operative ultrasonography and surgical findings. Acta Radiol 1998; 39: pp. 612-619.
16. Kayser R., Mahlfeld K., Heyde C.E.: Partial rupture of the proximal Achilles tendon: a differential diagnostic problem in ultrasound imaging. Br J Sports Med 2005; 39: pp. 838-842.
17. De Zordo T., Fink C., Feuchtner G.M., et. al.: Real-time sonoelastography findings in healthy Achilles tendons. AJR Am J Roentgenol 2009; 193: pp. 134-138.
18. Dirrichs T., Quack V., Gatz M., et. al.: Shear wave elastography (SWE) for the evaluation of patients with tendinopathies. Acad Radiol 2016; 23: pp. 1204-1213.
19. Aubry S., Nueffer J.P., Tanter M., et. al.: Viscoelasticity in Achilles tendinopathy: quantitative assessment by using real-time shear-wave elastography. Radiology 2015; 274: pp. 821-829.
20. Ooi C.C., Richards P.J., Maffulli N., et. al.: A soft patellar tendon on ultrasound elastography is associated with pain and functional deficit in volleyball players. J Sci Med Sport 2016; 19: pp. 373-378.
21. Vestergård Iversen J., Bartels E.M., Langberg H.: The Victorian Institute of Sports Assessment—Achilles Questionnaire (VISA-A)—a reliable tool for measuring Achilles tendinopathy. Int J Sports Phys Ther 2012; 7: pp. 76-84.
22. Germann G., Harth A., Wind G., et. al.: Standardisation and validation of the German version 2.0 of the Disability of Arm, Shoulder, Hand (DASH) questionnaire. Unfallchirurg 2003; 106: pp. 13-19.
23. Andres B.M., Murrell G.A.: Treatment of tendinopathy: what works, what does not, and what is on the horizon. Clin Orthop Relat Res 2008; 466: pp. 1539-1554.
24. Mafi N., Lorentzon R., Alfredson H.: Superior short-term results with eccentric calf muscle training compared to concentric training in a randomized prospective multicenter study on patients with chronic Achilles tendinosis. Knee Surg Sports Traumatol Arthrosc 2001; 9: pp. 42-47.
25. Dong Q., Fessell D.P.: Achilles tendon ultrasound technique. AJR Am J Roentgenol 2009; 193: pp. W173.
26. Clopper C., Pearson E.S.: The use of confidence or fiducial limits illustrated in the case of the binomial. Biometrika 1934; 26: pp. 404-413.
27. Glazebrook M.A., Wright J.R., Langman M., et. al.: Histological analysis of Achilles tendons in an overuse rat model. J Orthop Res 2008; 26: pp. 840-846.
28. Bah I., Kwak S.T., Chimenti R.L., et. al.: Mechanical changes in the Achilles tendon due to insertional Achilles tendinopathy. J Mech Behav Biomed Mater 2016; 53: pp. 320-328.
29. Aubry R.: Shear wave elastography in the assessment of tendon stiffness and for monitoring patients undergoing treatment. Diagn Imaging Eur 2015; 31: pp. 54-57.
30. Zwiers R., Wiegerinck J.I., van Dijk C.N.: Treatment of midportion Achilles tendinopathy: an evidence-based overview. Knee Surg Sports Traumatol Arthrosc 2016; 24: pp. 2103-2111.
31. Ryan M., Bisset L., Newsham-West R.: Should we care about tendon structure? The disconnect between structure and symptoms in tendinopathy. J Orthop Sports Phys Ther 2015; 45: pp. 823-825.
32. Docking S.I., Ooi C.C., Connell D.: Tendinopathy: is imaging telling us the entire story?. J Orthop Sports Phys Ther 2015; 45: pp. 842-852.
33. Chen X.M., Cui L.G., He P., et. al.: Shear wave elastographic characterization of normal and torn Achilles tendons: a pilot study. J Ultrasound Med 2013; 32: pp. 449-455.