
Rationale and Objectives
Shear wave elastography (SWE) has been shown to be a powerful tool to estimate tissue stiffness. The aim of this study was to compare the diagnostic accuracy of SWE to that of standard ultrasound (US) (combined use of B-mode US and power Doppler [PD] US) for diagnosing tendinopathies.
Materials and Methods
This is a prospective institutional review board–approved study on 112 participants (mean age 42 ± 13.4 years) with chronic (>6 months) tendon pain in Achilles, patellar, or epicondylar tendons. Participants were systematically examined with US, PD, and SWE using a high-resolution linear 15 MHz probe (SuperSonic Imagine). A semiquantitative analysis of SWE color charts and a quantitative region of interest-based analysis of tendon elasticity were performed. SWE values of symptomatic and healthy tendons were compared by using Student t test. Clinical symptom scores served as the standard of reference. US findings were compared to clinical symptom scores by using Spearman correlation.
Results
At semiquantitative analysis of SWE color charts, symptomatic tendons were rated as “soft” in 80/140 (57.1%), as “intermediate” in 54/140 (38.6%), and as “rigid” in 6/140 (4.3%).
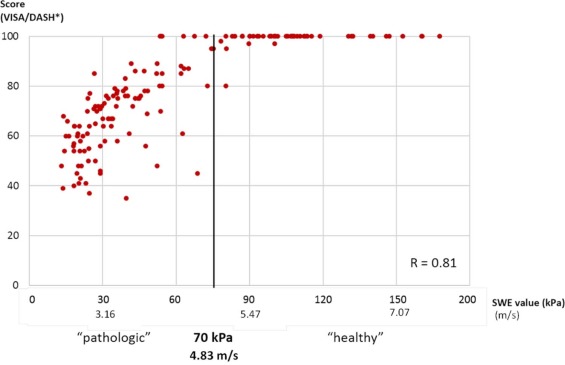
Healthy tendons were rated as “soft” in 8/84 (10%), as “intermediate” in 31/84 (37%), and as “rigid” in 45/84 (53%). At quantitative analysis, symptomatic tendons exhibited significantly lower mean SWE values (60.3 kPa/4.48 m/s; range 15.3–201.4 kPa/2.26–14.18 m/s) than healthy tendons (185 kPa/7.85 m/s; range 56–265 kPa/4.32–9.23 m/s) ( P = 0.0004). SWE values correlated closely with patients’ clinical symptoms obtained by clinical scores (r = 0.81). Overall sensitivity of conventional US and PD in detecting tendinopathies could be enhanced from 67.1% (94/140) to 94.3% (132/140) when combined with SWE.
Conclusions
SWE is a simple way to estimate tissue stiffness and, by reduced tissue rigidity, to identify tendon pathology. SWE significantly increases the diagnostic accuracy of tendon sonography and may prove to be a sensitive tool to early detect or monitor tendinopathy.
Introduction
Tendinopathies of Achilles and patellar tendons are common orthopedic overuse injuries, especially among sportsmen or athletes . The pathophysiology of both chronic tendon pain and chronic tendon injury, potentially leading to tendon rupture, begins with a prolonged phase of accumulation of subclinical microdamage .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Study Design and Population
Get Radiology Tree app to read full this article<
Inclusion Criteria
Get Radiology Tree app to read full this article<
Clinical Assessment
Get Radiology Tree app to read full this article<
Sonography Imaging Technique
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Data Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Demographics and Symptoms of All Study Cohort
All ( n = 112) Achilles Tendon ( n = 41) Patellar Tendon ( n = 38) Humeral Epicondylar Tendon ( n = 33) Age Mean ± SD 42 ± 13.4 50 ± 15.4 35 ± 9.4 49 ± 14.6 Median/Range 45/20–71 49/31–69 30/20–54 43/24–71 Sex Male 74(66%) 26(63%) 33(87%) 15(45%) Female 38(34%) 15(37%) 5(13%) 18(55%) Clinical score VISA-A Score VISA-P Score DASH Score \* Mean/SD 58.3 ± 14.5 56.2 ± 15.7 59.1 ± 11.9 40.7 ± 12.4 Median/Range 55/26–78 54/26–68 56/43–78 45/49–25 Evaluated tendons Asymptomatic 84(38%) 34(41%) 25(33%) 25(38%) Symptomatic 140(62%) 48(59%) 51(67%) 41(62%) unilateral 84(60%) 36(75%) 34(67%) 14(34%) bilateral 56(40%) 12(25%) 17(33%) 27(66%)
DASH, Disabilities of the Arm, Shoulder and Hand; SD, standard deviation; VISA, Victorian Institute of Sports Assessment.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Visual and Quantitative Tendon Evaluation by SWE
Get Radiology Tree app to read full this article<
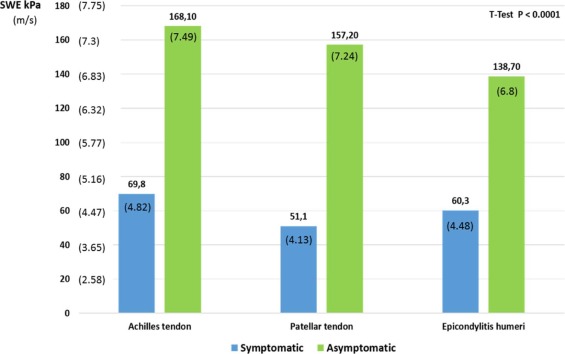
Table 2
SWE Values of Asymptomatic and Symptomatic Tendons for All Tendons and for Achilles Tendons, Patellar Tendons, and Humeral Epicondylar Tendons Separately
All Achilles Tendon Patellar Tendon Humeral Epicondylar Tendon Asymptomatic ( n = 84) Symptomatic ( n = 140) Asymptomatic ( n = 34) Symptomatic ( n = 48) Asymptomatic ( n = 25) Symptomatic ( n = 51) Asymptomatic ( n = 25) Symptomatic ( n = 41) Visual SWE Blue (soft) 12(14%) 80(57%) 3(9%) 32(67%) 3(12%) 26(51%) 6(24%) 22(54%) [7.6%–23.6%] [48.5%–65.5%] [1.9%–23.7%] [51.6%–79.6%] [2.6%–31.2%] [36.6%–65.3%] [9.4%–45.1%] [37.4%–69.3%] Turquoise–yellow (intermediate) 14(17%) 54(39%) 4(12%) 14(29%) 5(20%) 24(47%) 5(20%) 16(39%) [9.4%–26.4%] [30.5%–47.2%] [3.3%–27.5%] [17.0%–44.1%] [6.8%–40.7%] [32.9%–61.5%] [6.8%–40.7%] [24.2%–55.5%] Red (hard) 58(69%) 6(4%) 27(79%) 2(4%) 17(68%) 1(2%) 14(56%) 3(7%) [58.0%–78.7%] [1.6%–9.1%] [62.1%–91.3%] [0.5%–14.3%] [46.5%–88.7%] [0.05%–10.5%] [34.9%–75.6%] [1.5%–24.3%] Quantitative SWE in kPa and (m/s) Mean/SD 168.2 ± 20.3 60.3 ± 16.3 154.2 ± 28.3 53.4 ± 23. 2 176. 2 ± 18.2 56.3 ± 18.3 176.2 ± 18.2 64.1 ± 29.3 (7.49 ± 2.6) (4.48 ± 2.33) (7.17 ± 3.07) (4.22 ± 2.78) (7.66 ± 2.46) (4.33 ± 2.47) (7.66 ± 2.46) (4.62 ± 3.13) Median/Range 160(7.3)/ 58(4.4)/ 152(7.12)/ 55(4.28)/ 167(7.46)/ 57(4.35)/ 167/(7.46)/ 60(4.47)/ 53.7–271.3 15.3–201.4 67.2–231.3 13.4–176.1 89.2–231.2 14.5–153.1 89.2–231.2 23.1–201.2 (4.23–9.51) (2.26–8.19) (4.73–8.78) (2.11–7.66) (5.45–8.78) (2.2–7.14) (5.45–8.78) (2.77–8.19) <70 kPa (<4.83 m/s) 16(19%) 102(73%) 4(12%) 38(79%) 6(24%) 41(80%) 8(32%) 23(56%) [11.3%–29.1%] [64.7%–80.0%] [3.3%–27.5%] [65.0%–89.5%] [9.4%–45.1%] [66.9%–90.2%] [15.0%–53.5%] [39.8%–71.5%] 70–140 kPa (4.83–6.83 m/s) 21(25%) 32(23%) 6(18%) 8(17%) 8(32%) 9(18%) 7(28%) 15(37%) [16.2%–35.6%] [16.2%–30.7%] [6.8%–34.5%] [7.5%–30.2%] [15.0%–53.5%] [8.4%–30.1%] [12.1%–49.4%] [22.1%–53.1%] >140 kPa (>6.83 m/s) 47(56%) 6(4%) 24(71%) 2(4%) 11(44%) 1(2%) 10(40%) 3(7%) [44.7%–66.8%] [1.6%–9.1%] [52.5%–84.9%] [0.05%–14.3%] [24.4%–65.1%] [0.05%–10.5%] [21.1%–61.3%] [1.5%–24.3%]
SD, standard deviation; SWE, shear wave elastography.
Data in square brackets are 95% confidence intervals.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Comparison Between SWE Results in Asymptomatic and Symptomatic Tendons in the Same Patients
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Correlation of SWE Data and Clinical Symptom Scores
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Comparison of SWE with Conventional US (US and PD)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Diagnostic Accuracies of SWE Compared to Multimodal Ultrasound (B-mode US + Power Doppler)
Conventional Imaging (B-mode + Power Doppler) Conventional Imaging + SWE True positive 94 132 True negative 67 58 False negative 46 8 False positive 17 26 Sum 224 224 Sensitivity 67.1% 94.3% (94/140) (132/140) [587%–74.8%] [89.1%–97.5%] Specificity 81.7% 69.1% (67/82) (58/84) [71.6%–89.4%] [58.0%–78.7%] Positive predictive value 84.6% 83.5% (94/111) (132/158) [76.6.0%–90.8%] [76.8%–89.0%] Negative predictive value 59.3% 87.9% (67/113) (58/66) [49.7%–68.4%] [77.5%–94.6%] Diagnostic accuracy 71.9% 84.8% (161/224) (190/224) [65.5%–77.7%] [79.4%–89.3%]
SWE, shear wave elastography; US, ultrasound.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Maffulli N., Sharma P., Luscombe K.L.: Achilles tendinopathy: aetiology and management. J R Soc Med 2004; 97: pp. 472-476.
2. Cassel M., Baur H., Hirschmüller A., et. al.: Prevalence of Achilles and patellar tendinopathy and their association to intratendinous changes in adolescent athletes. Scand J Med Sci Sports 2015; 25: pp. e310-e318.
3. Patterson-Kane J.C., Rich T.: Achilles tendon injuries in elite athletes: lessons in pathophysiology from their equine counterparts. ILAR J 2014; 55: pp. 86-99.
4. Pingel J., Lu Y., Starborg T., et. al.: 3-D ultrastructure and collagen composition of healthy and overloaded human tendon: evidence of tenocyte and matrix buckling. J Anat 2014; 224: pp. 548-555.
5. Notarnicola A., Maccagnano G., Di Leo M., et. al.: Overload and neovascularization of Achilles tendons in young artistic and rhythmic gymnasts compared with controls: an observational study. Musculoskelet Surg 2014; 98: pp. 115-120.
6. de Jonge S., van den Berg C., de Vos R.J., et. al.: Incidence of midportion Achilles tendinopathy in the general population. Br J Sports Med 2011; 45: pp. 1026-1028.
7. Klauser A.S., Miyamoto H., Tamegger M., et. al.: Achilles tendon assessed with sonoelastography: histologic agreement. Radiology 2013; 267: pp. 837-842.
8. Lehtinen A., Peltokallio P., Taavitsainen M.: Sonography of Achilles tendon correlated to operative findings. Ann Chir Gynaecol 1994; 83: pp. 322-327.
9. Khan K.M., Forster B.B., Robinson J., et. al.: Are ultrasound and magnetic resonance imaging of value in assessment of Achilles tendon disorders? A two year prospective study. Br J Sports Med 2003; 37: pp. 149-153.
10. Paavola M., Paakkala T., Kannus P., et. al.: Ultrasonography in the differential diagnosis of Achilles tendon injuries and related disorders: a comparison between pre-operative ultrasonography and surgical findings. Acta Radiol 1998; 39: pp. 612-619.
11. Kayser R., Mahlfeld K., Heyde C.E.: Partial rupture of the proximal Achilles tendon: a differential diagnostic problem in ultrasound imaging. Br J Sports Med 2005; 39: pp. 838-842.
12. Visnes H., Tegnander A., Bahr R.: Ultrasound characteristics of the patellar and quadriceps tendons among young elite athletes. Scand J Med Sci Sports 2015; 25: pp. 205-215.
13. Athanasiou A., Tardivon A., Tanter M., et. al.: Breast lesions: quantitative elastography. Radiology 2010; 256: pp. 297-303.
14. Tanter M., Bercoff J., Athanasiou A., et. al.: Quantitative assessment of breast lesion viscoelasticity: initial clinical results using supersonic shear imaging. Ultrasound Med Biol 2008; 34: pp. 1373-1386.
15. Boehm K., Budäus L., Tennstedt P., et. al.: Prediction of significant prostate cancer at prostate biopsy and per core detection rate of targeted and systematic biopsies using real-time shear wave elastography. Urol Int 2015; 95: pp. 189-196.
16. Correas J.M., Tissier A.M., Khairoune A., et. al.: Prostate cancer: diagnostic performance of real-time shear-wave elastography. Radiology 2015; 275: pp. 280-289.
17. Ragazzoni F., Deandrea M., Mormile A., et. al.: High diagnostic accuracy and interobserver reliability of real-time elastography in the evaluation of thyroid nodules. Ultrasound Med Biol 2012; 38: pp. 1154-1162.
18. Berg W.A., Mendelson E.B., Cosgrove D.O., et. al.: Quantitative maximum shear-wave stiffness of breast masses as a predictor of histopathologic severity. AJR Am J Roentgenol 2015; 205: pp. 448-455.
19. Feldmann A., Langlois C., Dewailly M., et. al.: Shear wave elastography (SWE): an analysis of breast lesion characterization in 83 breast lesions. Ultrasound Med Biol 2015; 41: pp. 2594-2604.
20. De Zordo T., Fink C., Feuchtner G.M., et. al.: Real-time sonoelastography findings in healthy Achilles tendons. AJR Am J Roentgenol 2009; 193: pp. 134-138.
21. Aubry S., Nueffer J.P., Tanter M., et. al.: Viscoelasticity in Achilles tendonopathy: quantitative assessment by using real-time shear-wave elastography. Radiology 2015; 274: pp. 821-829.
22. Kot B.C.W., Zhang Z.J., Lee A.W.C., et. al.: Elastic modulus of muscle and tendon with shear wave. PLoS ONE 2012; 7:
23. Chen X.M., Cui L.G., He P., et. al.: Shear wave elastographic characterization of normal and torn achilles tendons: a pilot study. J Ultrasound Med 2013; 32: pp. 449-455.
24. Ooi C.C., Richards P.J., Maffulli N., et. al.: A soft patellar tendon on ultrasound elastography is associated with pain and functional deficit in volleyball players. J Sci Med Sport 2016; 19: pp. 373-378.
25. Iversen J.V., Bartels E.M., Langberg H.: The Victorian Institute of Sports Assessment – Achilles questionnaire (VISA-A)—a reliable tool for measuring achilles tendinopathy. Int J Sports Phys Ther 2012; 7: pp. 76-84.
26. Germann G., Harth A., Wind G., et. al.: Standardisation and validation of the German version 2.0 of the Disability of Arm, Shoulder, Hand (DASH) questionnaire. Unfallchirurg 2003; 106: pp. 13-19.
27. Ohberg L., Alfredson H.: Ultrasound guided sclerosis of neovessels in painful chronic Achilles tendinosis: pilot study of a new treatment. Br J Sports Med 2002; 36: pp. 173-175.
28. Glazebrook M.A., Wright J.R., Langman M., et. al.: Histological analysis of achilles tendons in an overuse rat model. J Orthop Res 2008; 26: pp. 840-846.
29. Kraemer R., Wuerfel W., Lorenzen J., et. al.: Analysis of hereditary and medical risk factors in Achilles tendinopathy and Achilles tendon ruptures: a matched pair analysis. Arch Orthop Trauma Surg 2012; 132: pp. 847-853.
30. Weinreb J.H., Sheth C., Apostolakos J., et. al.: Tendon structure, disease, and imaging. Muscles Ligaments Tendons J 2014; 4: pp. 66-73.
31. Comin J., Cook J.L., Malliaras P., et. al.: The prevalence and clinical significance of sonographic tendon abnormalities in asymptomatic ballet dancers: a 24-month longitudinal study. Br J Sports Med 2013; 47: pp. 89-92.
32. Sunding K., Fahlström M., Werner S., et. al.: Evaluation of Achilles and patellar tendinopathy with greyscale ultrasound and color Doppler: using a four-grade scale. Knee Surg Sports Traumatol Arthrosc 2016; 47: pp. 89-92.