
Rationale and Objectives
Initial data suggest that elastography can improve the specificity of ultrasound in differentiating benign and malignant breast lesions. The aim of this study was to compare elastography and B-mode ultrasound to determine whether the calculation of strain ratios (SRs) can further improve the differentiation of focal breast lesions.
Materials and Methods
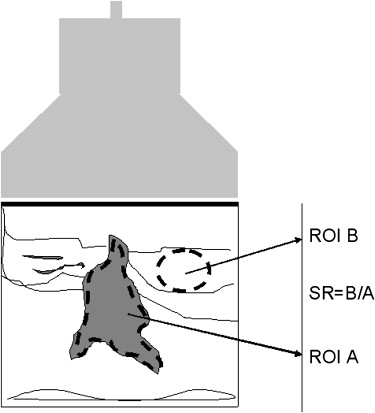
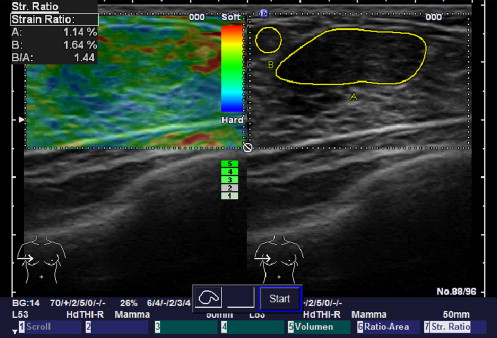
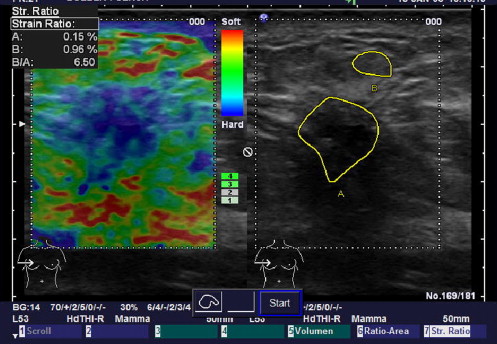
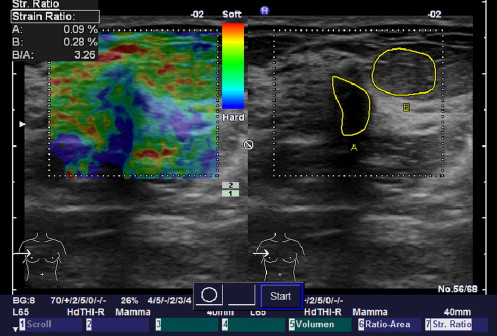
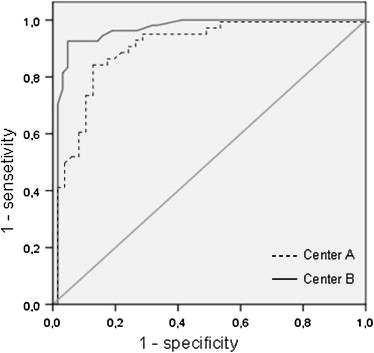
A total of 227 women with histologically proven focal breast lesions (113 benign, 114 malignant) were included at two German breast centers. The women underwent a standardized ultrasound procedure using a high-end ultrasound system with a 9-MHz broadband linear transducer. B-mode scans and sonoelastograms were analyzed by two experienced readers using the Breast Imaging Reporting and Data System criteria. SRs were calculated from a tumor-adjusted region of interest (mean color pixel density) and a comparable region of interest placed in the lateral fatty tissue. Sensitivity, specificity, and cutoff values were calculated for SRs (receiver-operating characteristic analysis).
Results
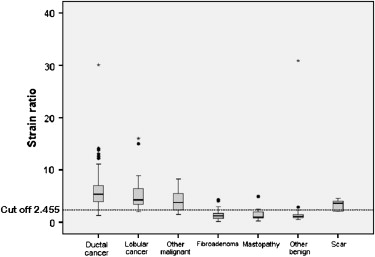
The women had a mean age of 54 years (range, 19–87 years). The mean lesion diameter was 1.6 ± 0.9 cm. Sensitivity and specificity were 96% and 56% for B-mode scanning, 81% and 89% for elastography, and 90% and 89% for SRs. An SR cutoff value of 2.45 (area under the curve, 0.949) allowed significant differentiation ( P < .001) of malignant (mean, 5.1 ± 4.2) and benign (mean, 1.6 ± 1.0) lesions. The quantitative method of SR calculation was superior to subjective interpretation of sonoelastograms and B-mode scans, with a positive predictive value of 89% compared to 68% and 84% for the other two methods.
Conclusions
Calculation of SRs contributes to the standardization of sonoelastography with high sensitivity and allows significant differentiation of benign and malignant breast lesions with higher specificity compared to B-mode ultrasound but not elastography.
Elasticity is an important property of biologic tissues that changes with age and in the presence of pathology. It is defined as the elongation (stretching) of tissue under strain. Elasticity therefore is a measure of the amount of pressure that needs to be applied to induce elastic deformation of the tissue . Tissue elasticity can be visualized by sonoelastography, an imaging modality based on the analysis of ultrasound information . Numerous studies have recently shown that information on tissue elasticity has clinical benefit in the diagnostic evaluation of different organ systems . Several investigators have shown that elastography can improve specificity in characterizing focal breast lesions . Elastography is the visualization of tissue properties traditionally evaluated by palpation, which is an established clinical technique to characterize focal breast lesions. Studies investigating breast sonoelastography have focused on lesions that are notoriously difficult to characterize, namely, Breast Imaging Reporting and Data System (BI-RADS) category 3 and 4 lesions and lesions occurring in the presence of lipomatous involution. If sonoelastography can identify true benign lesions in women with indeterminate lesions on the basis of other diagnostic modalities, this new technique might in the future obviate the need for histologic confirmation in these cases .
Sonoelastographic information can be obtained by real-time scanning or by offline analysis . In so-called strain imaging, the change in tissue elasticity under compression is calculated, and the information is color coded and superimposed on B-mode images. This method is limited by a lack of standardization. Elastic properties can be described quantitatively by calculating strain ratios (SR). We therefore conducted a prospective study to investigate whether the calculation of SRs can also improve the differentiation of focal breast lesions. This was done by comparing SRs with B-mode ultrasound and conventional sonoelastography.
Materials and methods
Get Radiology Tree app to read full this article<
Ultrasound Examination
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Evaluation of Ultrasound Scans
Get Radiology Tree app to read full this article<
Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Histology
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Histologic Diagnoses of 227 Benign and Malignant Breast Lesions
Benign Lesions ( n = 113) Malignant Lesions ( n = 114) Fibroadenoma 64 Invasive ductal cancer 84 Mastopathy 15 Invasive lobular cancer 19 Scar 5 Other malignant lesions 11 Other benign lesions 29
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Sensitivity, Specificity, and Positive Predictive Value of the Three Methods Compared
Parameter B-Mode Scan Elastography Strain Ratio Sensitivity 96% 81% 90% Specificity 56% 89% 89% Positive predictive value 68% 84% 89%
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Limitations
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Krouskop T.A., Wheeler T.M., Kallel F., et. al.: Elastic moduli of breast and prostate tissues under compression. Ultrason Imaging 1998; 20: pp. 260-274.
2. Konofagou E., Ophir J.: A new elastographic method for estimation and imaging of lateral displacements, lateral strains, corrected axial strains and Poisson’s ratios in tissues. Ultrasound Med Biol 1998; 24: pp. 1183-1199.
3. Frauscher F., Gradl J., Pallwein L.: Prostate ultrasound—for urologists only?. Cancer Imaging 2005; 23: pp. 76-82.
4. Lyshchik A., Higashi T., Asato R., et. al.: Thyroid gland gland tumor diagnosis at US. Radiology 2005; 237: pp. 202-211.
5. Mendelson E.B., Berg W.A., Merritt C.R.: Toward a standardized breast ultrasound lexicon, BI-RADS. ultrasound. Semin Roentgenol 2001; 36: pp. 217-225.
6. Thomas A., Kümmel S., Gemeinhardt O., et. al.: Real-time sonoelastography of the cervix: tissue elasticity of the normal and abnormal cervix. Acad Radiol 2007; 14: pp. 193-200.
7. Thomas A., Fischer T., Ohlinger R., et. al.: An advanced method of ultrasound—real-time elastography: first experience on 106 patients with breast lesions. Ultrasound Obstet Gynecol 2006; 28: pp. 335-340.
8. Thomas A., Kümmel S., Fritzsche F., et. al.: Real-time sonoelastography performed in addition to B-mode ultrasound and mammography: improved differentiation of breast lesions?. Acad Radiol 2006; 13: pp. 1496-1504.
9. Guiseppetti G.M., Martegani A., Cioccio Di, et. al.: Elastosonography in the diagnosis of the nodular breast lesions: a preliminary report. Radiol Med 2005; 110: pp. 69-76.
10. Itoh A., Ueno E., Tohno E., et. al.: Breast disease: clinical application of US elastography for diagnosis. Radiology 2006; 239: pp. 341-350.
11. Zhi H., Ou B., Luo B., et. al.: Comparison of ultrasound elastography, mammography, and sonography in the diagnosis of solid breast lesions. J Ultrasound Med 2007; 26: pp. 807-815.
12. Zhu Q., Jiang Y., Liu J., et. al.: Real-time ultrasound elastography: its potential role in assessment of breast lesions. Ultrasound Med Biol 2008; 34: pp. 1232-1238.
13. Fleury E.F.C., Rinaldi J.F., Piato S., et. al.: Appearance of breast masses on sonoelastography with special focus on the diagnosis of fibroadenomas. Eur Radiol 2009; 19: pp. 1337-1346.
14. Thomas A., Warm M., Diekmann F., et. al.: Tissue Doppler and strain imaging for evaluating tissue elasticity of breast lesions. Acad Radiol 2007; 14: pp. 522-529.
15. Frey H Realtime-Elastographie.: Ein neues sonographisches Verfahren für die Darstellung der Gewebeelastizität. Radiologe 2003; 10: pp. 850-855.
16. Hong A.S., Rosen E.L., Soo M.S., et. al.: BI-RADS for sonography: positive and negative values of sonographic features. AJR Am J Roentgenol 2005; 184: pp. 1260-1265.
17. http://www.acr.org/SecondaryMainMenuCategories/quality_safety/BIRADSAtlas/BIRADSAtlasexcerptedtext/BIRADSUltrasoundFirstEdition.aspxBI-RADS-Ultrasund, First Edition, ACR 2003 .
18. Bercoff J., Chaffai S., Tanter M., et. al.: In vivo breast tumor detection using transient elastography. Ultrasound Med Biol 2003; 10: pp. 1387-1396.
19. Cespedes I., Ophir J., Ponnekanti H., et. al.: Elastography: elasticity imaging using ultrasound with application to muscle and breast in vivo. Ultrason Imaging 1993; 15: pp. 73-88.
20. Hiltawsky K.M., Krüger M., Starke C., et. al.: Freehand ultrasound elastography of breast lesions: clinical results. Ultrasound Med Biol 2001; 27: pp. 1461-1469.
21. Tardivon A., El Khoury C., Thibault F., et. al.: Elastography of the breast: a prospective study of 122 lesions. J Radiol 2007; 88: pp. 657-662.
22. Tan S.M., Teh H.S., Kent Mancer J.F., et. al.: Improving B mode ultrasound evaluation of breast lesions with real time ultrasound elastography—a clinical approach. Breast 2008; 17: pp. 252-257.
23. Scaperrotta G., Ferranti C., Costa C., et. al.: Role of sonoelastography in non-palpable breast lesions. Eur Radiol 2008; 18: pp. 2381-2389.
24. Tohno E., Ueno E.: Current improvements in breast ultrasound, with a special focus on elastography. Breast Cancer 2008; 15: pp. 200-204.
25. Huang Y.L., Chen D.R., Jiang Y.R., et. al.: Computer-aided diagnosis using morphological features for classifying breast lesions on ultrasound. Ultrasound Obstet Gynecol 2008; 32: pp. 565-572.