
Rationale and Objectives
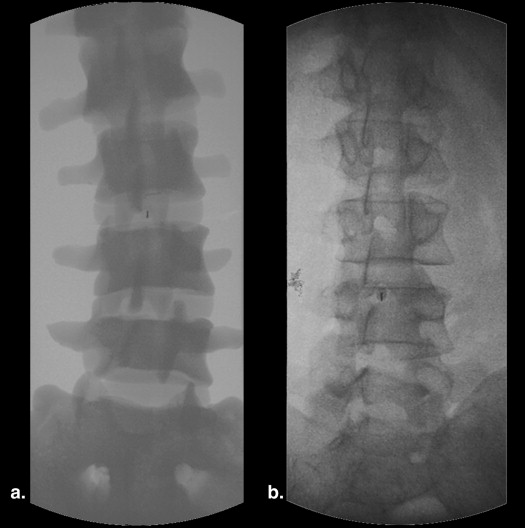
Fluoroscopically guided lumbar puncture (FGLP) is a commonly performed procedure with increased success rates relative to bedside technique. However, FGLP also exposes both patient and staff to ionizing radiation. The purpose of this study was to determine if the use of a simulation-based FGLP training program using an original, inexpensive lumbar spine phantom could improve operator confidence and efficiency, while also reducing patient dose.
Materials and Methods
A didactic and simulation-based FGLP curriculum was designed, including a 1-hour lecture and hands-on training with a lumbar spine phantom prototype developed at our institution. Six incoming post-graduate year 2 (PGY-2) radiology residents completed a short survey before taking the course, and each resident practiced 20 simulated FGLPs using the phantom before their first clinical procedure. Data from the 114 lumbar punctures (LPs) performed by the six trained residents (prospective cohort) were compared to data from 514 LPs performed by 17 residents who did not receive simulation-based training (retrospective cohort). Fluoroscopy time (FT), FGLP success rate, and indication were compared.
Results
There was a statistically significant reduction in average FT for the 114 procedures performed by the prospective study cohort compared to the 514 procedures performed by the retrospective cohort. This held true for all procedures in aggregate, LPs for myelography, and all procedures performed for a diagnostic indication. Aggregate FT for the prospective group (0.87 ± 0.68 minutes) was significantly lower compared to the retrospective group (1.09 ± 0.65 minutes) and resulted in a 25% reduction in average FT ( P = .002). There was no statistically significant difference in the number of failed FGLPs between the two groups.
Conclusions
Our simulation-based FGLP curriculum resulted in improved operator confidence and reduced FT. These changes suggest that resident procedure efficiency was improved, whereas patient dose was reduced. The FGLP training program was implemented by radiology residents and required a minimal investment of time and resources. The LP spine phantom used during training was inexpensive, durable, and effective. In addition, the phantom is compatible with multiple modalities including fluoroscopy, computed tomography, and ultrasound and could be easily adapted to other applications such as facet injections or joint arthrograms.
Lumbar puncture (LP) is a commonly performed procedure used to provide access into the intrathecal subarachnoid space, either for diagnostic and/or therapeutic collection of cerebrospinal fluid or for the intrathecal administration of medications such as contrast media or chemotherapeutic agents. Although classically performed at the bedside using visual and palpable landmarks, the use of image guidance is associated with increased success rates and has been shown to decrease the rate of traumatic LP . The use of image guidance is particularly useful for difficult cases such as patients with severe scoliosis, lumbar hardware, or morbid obesity . Fluoroscopically guided LP (FGLP) is considered a core competency and is listed in the diagnostic radiology residency milestones by the American College of Graduate Medical Education and the American Board of Radiology .
Fluoroscopy is an essential component of many image-guided procedures because it provides real-time visualization of procedural instruments and patient anatomy. However, the use of fluoroscopy is not entirely benign. Fluoroscopy exposes both the patient and staff members to potentially high levels of ionizing radiation . In 2006, the National Council on Radiation Protection released a report describing a 5.7-fold increase in annual effective radiation dose per individual in the US population owing to medical imaging from 1980 to 2006 . More recently, a Sentinel Event Alert from the Joint Commission in 2011 regarding the radiation risks of diagnostic imaging noted that the average radiation exposure in the United States is 4.7 times that of the global population (3 mSv per individual in the United States compared to 0.64 mSv per individual globally) .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
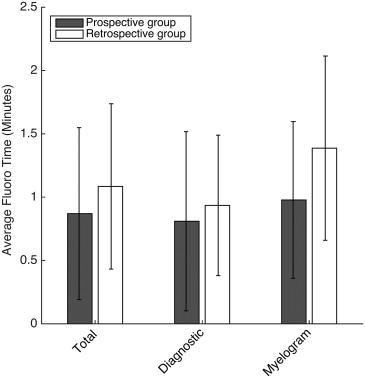
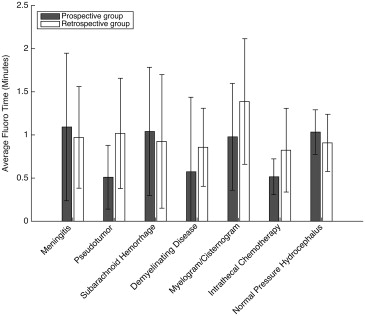
Table 1
Average Fluoroscopy Time (Minutes) for All Indications in Prospective versus Retrospective Study Cohorts
Indication Avg. Fluoro Time (Prospective), Minutes Avg. Fluoro Time (Retrospective), Minutes_P_ Value Meningitis 1.09 0.97 .87 Pseudotumor 0.51 1.02 .009 ∗ SAH 1.04 0.93 .8 Demyelination 0.57 0.86 .09 Myelography 0.98 1.39 .001 ∗ Intrathecal chemotherapy 0.52 0.82 .04 ∗ NPH 1.03 0.91 .43
Avg., average; NPH, normal pressure hydrocephalus; SAH, subarachnoid hemorrhage.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Average Fluoroscopy Time (Minutes) for Prospective versus Retrospective Study Cohorts
Avg. Fluoro Time (Prospective), Minutes Avg. Fluoro Time (Retrospective), Minutes_P_ Value Diagnostic LP 0.81 0.94 .002 ∗ LP for myelogram 0.98 1.4 .001 ∗ All FGLP (total) 0.87 1.09 .002 ∗
Avg., average; FGLP, fluoroscopically guided lumbar puncture; LP, lumbar puncture.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Supplementary Data
Get Radiology Tree app to read full this article<
Appendix
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Eskey C.J., Ogilvy C.S.: Fluoroscopy-guided lumbar puncture: decreased frequency of traumatic tap and implications for the assessment of CT-negative acute subarachnoid hemorrhage. AJNR Am J Neuroradiol 2001; 22: pp. 571.
2. Boddu S.R., Corey A., Peterson R., et. al.: Fluoroscopic-guided lumbar puncture: fluoroscopic time and implications of body mass index—a baseline study. AJNR Am J Neuroradiol 2014;
3. Accreditation Council for Graduate Medical Education: ACGME program requirements for graduate medical education in diagnostic radiology.2007. http://www.acgme.org/acgmeweb/Portals/0/PFAssets/2013-PR-FAQ-PIF/420_diagnostic_radiology_07012013.pdf Accessed July 6, 2014
4. 2012. https://www.acgme.org/acgmeweb/Portals/0/PDFs/Milestones/DiagnosticRadiologyMilestones.pdf Accessed July 6, 2014
5. European Society of Radiology (ESR): White paper on radiation protection by the European Society of Radiology. Insights Imaging 2011; 2: pp. 357-362.
6. Schauer D.A., Linton O.W.: National Council on Radiation Protection and Measurements report shows substantial medical exposure increase. Radiology 2009; 253: pp. 293-296.
7. The Joint Commission: Sentinel Event Alert: Radiation risks of diagnostic imaging.2011. https://www.wvdhhr.org/rtia/pdf/SEA_47[1].pdf Accessed July 6, 2014
8. Mahesh M.: Fluoroscopy: patient radiation exposure issues. Radiographics 2001; 21: pp. 1033-1045.
9. Jones AK, Pasciak AS, Steele J. A Comprehensive Course in the Safe Use of Fluoroscopy, Fluoroscopic Safety, LLC. http://fluorosafety.com/advanced-training-program/ . December 19, 2013. Accessed July 6, 2014.
10. Frederick-Dyer K.C., Faulkner A.R., Chang T.T., et. al.: Web-based training on the safe use of fluoroscopy can result in substantial decrease in patient dose. Academic Radiology 2013; 20: pp. 1272-1277.
11. Faulkner A.R., Bourgeois A.C., Bradley Y.C., Pasciak A.S.: A robust and inexpensive phantom for fluoroscopically guided lumbar puncture training. Simulation in Healthcare 2015; 10: pp. 54-58.
12. Dawson D.L., Meyer J., Lee E.S., et. al.: Training with simulation improves residents’ endovascular procedure skills. J Vasc Surg 2007; 45: pp. 149-154.