
Rationale/Objectives
Smoking has been associated with decreased incidence and prevalence of sarcoidosis, but few studies have evaluated effects of smoking on clinical parameters of the disease. The objectives were to determine the association of smoking with radiographic patterns and to evaluate the associations of these smoking-related radiographic patterns on airflow obstruction in sarcoidosis.
Materials and Methods
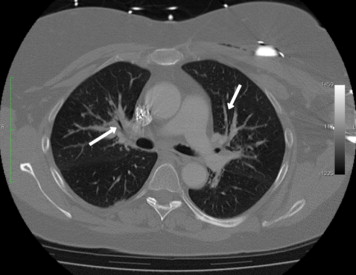
Clinical data and computed tomography (CT) scans of 124 patients with sarcoidosis were reviewed. CT scans were assessed for lymph nodes, nodules, bronchiectasis, bronchovascular bundle thickening, displaced hilum, fibrosis, ground glass, emphysema, pleural changes, and alveolar opacities. CT patterns were compared between patients with and without a history of smoking. The effect of smoking on the associations between radiographic patterns and airflow obstruction was assessed with multivariable analysis.
Results
Smokers had less frequency of bronchovascular bundle thickening than nonsmokers (11/38 subjects [29%] vs 50/86 subjects [58%], P = .003) and more emphysema (7/38 subjects [18%] vs 1/86 subjects [1%], P = .001). Patients who had bronchovascular bundle thickening were less likely to have ever smoked (11/61 subjects [18%] vs 27/63 subjects [43%], P = .003) or be current smokers (4/61 subjects [7%] vs 15/63 subjects [24%], P = .008). Age ( P = .003) and bronchovascular bundle thickening ( P = .02) were independent predictors of airflow obstruction. There were no differences in smoking history between patients with airflow obstruction versus those without (10/37 subjects [27%] vs 28/87 subjects [32%], P = .63).
Conclusions
In patients with sarcoidosis, smoking is associated with decreased frequency of bronchovascular bundle thickening, an important clinical manifestation of the lung disease. Further, bronchovascular bundle thickening and age are the only independent predictors of airflow obstruction, and smoking does not confound these associations.
Sarcoidosis is an inflammatory disease of unknown etiology predominately affecting the lungs. Noncaseating granulomas are the hallmark of the disease and can cause decreased pulmonary function, impairment of gas exchange, and fibrosis of lung parenchyma. The natural history of the disease is not completely understood, adding complexity to clinical management and treatment . Thus, further study of clinical parameters is warranted.
Multiple epidemiologic studies have found smoking to be associated with decreased incidence and prevalence of the disease . A case control etiologic study of sarcoidosis (ACCESS) showed that smoking subjects were less likely to have sarcoidosis (OR 0.62, CI 0.5–0.77), and Visser et al found that patients presenting with sarcoid arthritis were much less likely to be smoking (OR 0.09, CI 0.02–0.37) . However, there are few studies that have evaluated the effect of smoking on patients who have sarcoidosis. For instance, two descriptive studies of sarcoidosis populations have not indicated that smoking affects progression or severity of disease or that smoking prevents respiratory failure in this group . The mechanisms behind this paradoxical phenomenon (decreased incidence, but no effect on disease severity) are unclear, and the question of how smoking has an overall effect on sarcoidosis remains unanswered.
Get Radiology Tree app to read full this article<
Methods
Get Radiology Tree app to read full this article<
CT Scans
Get Radiology Tree app to read full this article<
Pulmonary Function Tests
Get Radiology Tree app to read full this article<
Analysis
Get Radiology Tree app to read full this article<
Results
Patient Characteristics
Get Radiology Tree app to read full this article<
Table 1
Patient Characteristics and CT Findings
Variable Population ( n = 124) Age (y) ∗ 45 (11) (range, 16–75) Gender Female 82 (66%) Race African-American 19 (15%) Caucasian 105 (85%) Smoking Status Never smoked 86 (69%) Ever smoked (past or active) 38 (31%) Active smoker 20 (16%) Obstructive lung disease 37 (30%) Pulmonary function (%) ∗ FVC 85 (19) FEV1 83 (22) FEV1/FVC 75 (67–80) TLC 89 (18) DLco 75 (64–85) Asthma history 16 (13%) Obstructive sleep apnea 16 (13%) Systemic treatment history 94 (76%) Prednisone therapy 87 (70%) Methotrexate 59 (48%) Reason for treatment Pulmonary disease 49 (40%) Extrapulmonary disease 45 (36%) Inhaled therapies 51 (41%) Corticosteroid inhaler only 13 (10%) Bronchodilator inhaler only 12 (10%) Steroid and bronchodilator 26 (21%) CT Findings Lymph nodes 111 (90%) Nodules 83 (67%) BVB thickening 61 (49%) Fibrosis 32 (26%) Bronchiectasis 29 (23%) Ground glass 23 (19%) Alveolar opacities 15 (12%) Displaced hilum 14 (11%) Emphysema 8 (6%) Pleural changes 7 (6%)
CT, computed tomography; DLco, diffusing capacity; FEV1, forced expiratory volume in one second; FVC, forced vital capacity; TLC, total lung capacity.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Comparison of Smokers versus Nonsmokers
Get Radiology Tree app to read full this article<
Table 2
Patient Characteristics and Frequencies of CT Findings According to Smoking History
Ever Smoked ( n = 38) Never Smoked ( n = 86)P Value Age (y) ∗ 42 (13) 48 (8) .01 Gender Female 28 (74%) 54 (63%) .2 Race Caucasian 28 (74%) 77 (90%) .03 African-American 10 (26%) 9 (10%) .03 Obstructive disease 10 (26%) 27 (31%) .6 Pulmonary function (%) † ∗ FVC 85 (21) 86 (18) .8 FEV1 83 (22) 83 (24) .98 FEV1/FVC 77 (70–82) 74 (66–78) .08 TLC 88 (19) 89 (17) .7 DLco 71 (55–83) 76 (66–88) .1 Treatment Total treated 28 (74%) 66 (76%) .7 CT scan prior to treatment 15 (40%) 28 (32%) .5 Ongoing treatment during CT 11 (29%) 25 (29%) 1.0 Completed treatment 2 (5%) 13 (15%) .1 Reason for treatment Pulmonary disease 9 (24%) 40 (61%) .02 Extrapulmonary disease 19 (50%) 26 (39%) .03 Type of treatment Prednisone 24 (63%) 63 (73%) .3 Methotrexate 17 (45%) 42 (49%) .7 Inhaled therapy 12 (32%) 39 (45%) .2 Corticosteroid Only 2 (5%) 11 (13%) .3 Bronchodilator Only 6 (16%) 6 (7%) .2 Steroid and Bronchodilator 4 (11%) 22 (26%) .09 CT Findings Lymph nodes 36 (95%) 75 (87%) .2 Bronchiectasis 9 (24%) 20 (23%) .9 Nodules 23 (61%) 60 (70%) .3 Thickened BV bundles 11 (29%) 50 (58%) .003 Ground glass 10 (26%) 13 (15%) .1 Displaced hilum 3 (8%) 10 (12%) .8 Emphysema 7 (18%) 1 (1%) .001 Alveolar opacities 3 (8%) 12 (14%) .6 Pleural changes 0 (0%) 7 (8%) .1 Fibrosis 9 (24%) 23 (27%) .8
CT, computed tomography; DLco, diffusing capacity; FEV1, forced expiratory volume in one second; FVC, forced vital capacity; TLC, total lung capacity.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Characteristics of Patients with the CT Finding of Bronchovascular Bundle Thickening
Thick BV Bundles ( n = 61) No Thick BV Bundles ( n = 63)P Value Age (y) ∗ 47 (13) 45 (9) .4 Smoking status Current active Smokers 4 (7%) 15 (24%) .008 Ever smoked † 11 (18%) 27 (43%) .003 Never smoked 50 (82%) 36 (57%) .003 Obstructed 25 (41%) 12 (19%) .008 Ever treated 51 (84%) 43 (68%) .04 Prednisone 48 (79%) 39 (62%) .05 Methotrexate 30 (49%) 29 (46%) .9 Inhaled therapies 29 (48%) 22 (35%) .2
BV, bronchovascular; CT, computed tomography.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CT Findings in Patients with Airflow Obstruction
Get Radiology Tree app to read full this article<
Table 4
Characteristics of Obstructed and Nonobstructed Patients
Variable Nonobstructed ( n = 87) Obstructed ( n = 37)P Value Age (y) ∗ 43 (11) 51 (10) .0008 Gender Female 57 (65%) 25 (68%) .8 Race African-American 17 (20%) 2 (5%) .06 Caucasian 70 (80%) 35 (95%) .06 Smoking Status Never smoked 59 (68%) 27 (73%) .6 Ever smoked 28 (32%) 10 (27%) .6 Obstructive disease Pulmonary function (%) ∗ † FVC 88 (20) 80 (16) .05 FEV1 90 (20) 67 (18) <.0001 FEV1/FVC 78 (75–82) 64 (57–67) <.0001 TLC 87 (17) 92 (19) .3 DLco 76 (60–84) 74 (65–88) .6 Asthma history 9 (10%) 7 (19%) .2 Obstructive sleep apnea 9 (10%) 7 (19%) .2 Treatment history Prednisone therapy 57 (65%) 30 (81%) .09 Methotrexate 39 (45%) 20 (54%) .3 Inhaled therapies 27 (27%) 24 (65%) .0005 Steroid/bronchodilator 14 (16%) 12 (32%) .04 Corticosteroid 6 (7%) 7 (19%) .06 Bronchodilator only 7 (8%) 5 (14%) .3 CT Findings Lymph nodes 79 (91%) 32 (86%) .5 Nodules 53 (61%) 30 (81%) .03 BVB thickening 36 (41%) 25 (68%) .008 Fibrosis 18 (21%) 14 (38%) .04 Bronchiectasis 17 (20%) 12 (32%) .1 Ground glass 13 (15%) 10 (27%) .1 Alveolar opacities 8 (9%) 7 (19%) .1 Displaced hilum 5 (6%) 8 (22%) .02 Emphysema 4 (5%) 4 (11%) .2 Pleural changes 5 (6%) 2 (5%) .9
CT, computed tomography; DLco, diffusing capacity; FEV1, forced expiratory volume in one second; FVC, forced vital capacity; TLC, total lung capacity.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Statement on sarcoidosis. Joint Statement of the American Thoracic Society (ATS), the European Respiratory Society (ERS) and the World Association of Sarcoidosis and Other Granulomatous Disorders (WASOG) adopted by the ATS Board of Directors and by the ERS Executive Committee, February 1999. Am J Respir Crit Care Med 1999; 160: pp. 736-755.
2. Harf R.A., Ethevenaux C., Gleize J., et. al.: Reduced prevalence of smokers in sarcoidosis. Results of a case-control study. Ann N Y Acad Sci 1986; 465: pp. 625-631.
3. Valeyre D., Soler P., Clerici C., et. al.: Smoking and pulmonary sarcoidosis: effect of cigarette smoking on prevalence, clinical manifestations, alveolitis, and evolution of the disease. Thorax 1988; 43: pp. 516-524.
4. Hance A.J., Basset F., Saumon G., et. al.: Smoking and interstitial lung disease. The effect of cigarette smoking on the incidence of pulmonary histiocytosis X and sarcoidosis. Ann N Y Acad Sci 1986; 465: pp. 643-656.
5. Douglas J.G., Middleton W.G., Gaddie J., et. al.: Sarcoidosis: a disorder commoner in non-smokers?. Thorax 1986; 41: pp. 787-791.
6. Newman L.S., Rose C.S., Bresnitz E.A., et. al.: A case control etiologic study of sarcoidosis: environmental and occupational risk factors. Am J Respir Crit Care Med 2004; 170: pp. 1324-1330.
7. Visser H., Vos K., Zanelli E., et. al.: Sarcoid arthritis: clinical characteristics, diagnostic aspects, and risk factors. Ann Rheum Dis 2002; 61: pp. 499-504.
8. Demirkok S.S., Basaranoglu M., Akinci E.D., et. al.: Analysis of 275 patients with sarcoidosis over a 38 year period; a single-institution experience. Respir Med 2007; 101: pp. 1147-1154.
9. Strom K.E., Eklund A.G.: Smoking does not prevent the onset of respiratory failure in sarcoidosis [abstract]. Sarcoidosis 1993; 10: pp. 26-28.
10. Miller M.R., Hankinson J., Brusasco V., et. al.: Standardisation of spirometry. Eur Respir J 2005; 26: pp. 319-338.
11. Koyama T., Ueda H., Togashi K., et. al.: Radiologic manifestations of sarcoidosis in various organs. Radiographics 2004; 2: pp. 87-104.
12. Nishimura K., Itoh H., Kitaichi M., et. al.: Pulmonary sarcoidosis: correlation of CT and histopathologic findings. Radiology 1993; 189: pp. 105-109.
13. Warren C.P.: Extrinsic allergic alveolitis: a disease commoner in non-smokers. Thorax 1977; 32: pp. 567-569.
14. Calkins B.M.: A meta-analysis of the role of smoking in inflammatory bowel disease. Dig Dis Sci 1989; 34: pp. 1841-1854.
15. Madretsma G.S., Donze G.J., van Dijk A.P., et. al.: Nicotine inhibits the in vitro production of interleukin 2 and tumour necrosis factor-alpha by human mononuclear cells. Immunopharmacology 1996; 35: pp. 47-51.
16. Yamaguchi E., Itoh A., Furuya K., et. al.: Release of tumor necrosis factor-alpha from human alveolar macrophages is decreased in smokers. Chest 1993; 103: pp. 479-483.
17. Blanchet M.R., Israel-Assayag E., Cormier Y.: Inhibitory effect of nicotine on experimental hypersensitivity pneumonitis in vivo and in vitro. Am J Respir Crit Care Med 2004; 169: pp. 903-909.
18. Drent M., van Velzen-Blad H., Diamant M., et. al.: Relationship between presentation of sarcoidosis and T lymphocyte profile. A study in bronchoalveolar lavage fluid. Chest 1993; 104: pp. 795-800.
19. Peros-Golubicic T., Ljubic S.: Cigarette smoking and sarcoidosis [abstract]. Acta Med Croatica 1995; 49: pp. 187-193.
20. Cottin V., Nunes H., Brillet P.Y., et. al.: Combined pulmonary fibrosis and emphysema: a distinct underrecognized entity. Eur Respir J 2005; 26: pp. 586-593.
21. Mejia M., Carrillo G., Rojas-Serrano J., et. al.: Idiopathic pulmonary fibrosis and emphysema: decreased survival associated with severe pulmonary arterial hypertension. Chest 2009; 136: pp. 10-15.
22. Terasaki H., Fujimoto K., Muller N.L., et. al.: Pulmonary sarcoidosis: comparison of findings of inspiratory and expiratory high-resolution CT and pulmonary function tests between smokers and nonsmokers. AJR Am J Roentgenol 2005; 185: pp. 333-338.
23. Handa T., Nagai S., Fushimi Y., et. al.: Clinical and radiographic indices associated with airflow limitation in patients with sarcoidosis. Chest 2006; 130: pp. 1851-1856.
24. Hansell D.M., Milne D.G., Wilsher M.L., et. al.: Pulmonary sarcoidosis: morphologic associations of airflow obstruction at thin-section CT. Radiology 1998; 209: 697–670