
Rationale and Objectives
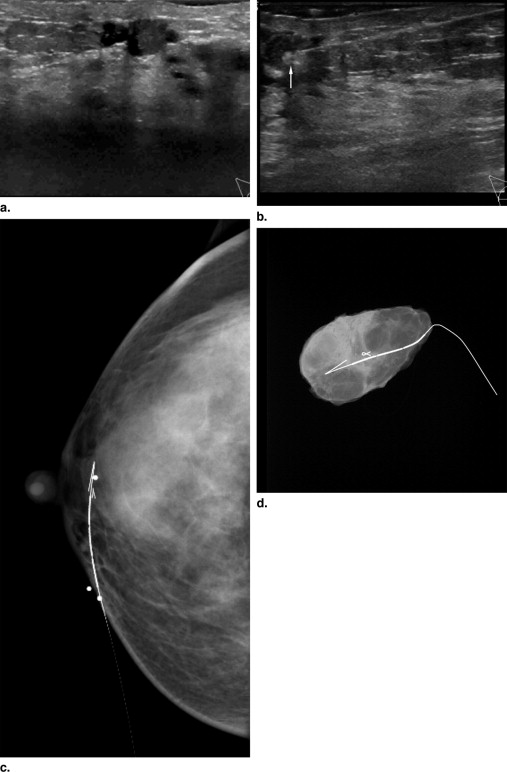
To propose deploying a metallic marker using sonographic guidance immediately before wire localization for excisional biopsy to identify intraductal or complex cystic lesions at specimen radiography.
Materials and Methods
Institutional review board approval was obtained for this study and is Health Insurance Portability and Accountability Act compliant. The clinical, radiographic, and pathologic records of 21 patients, ages 21–78 years, with 22 intraductal or complex cystic masses who underwent excisional biopsy with wire localization immediately after sonographically-guided marker placement were reviewed. The procedure mammogram, ultrasound, and specimen radiographs were reviewed and evaluated for the presence of a metallic marker, lesion, or both. Pathology of all specimens was recorded and reviewed for concordance.
Results
Twenty-one (95%) of the markers were visualized on specimen radiographs. No lesions were apparent on specimen radiographs. Mammographic findings in 17 were negative (17/22; 77%); 3 circumscribed or partially obscured masses (3/22; 14%), 1 focal asymmetry (1/22; 5%), and 1 architectural distortion (5%) were also seen. Sonographic findings were 12 intraductal masses (12/22; 55%) and 10 complex cystic masses (10/22; 45%). Median and average size of all lesions were 9 mm (intraductal masses: median, 6 mm, mean, 7; complex cystic masses: median, 10 mm, mean, 11). All lesions were benign and all pathology was concordant with imaging findings.
Conclusions
Given the high rate of marker retrieval on specimen radiography and pathologic concordance, marker placement at the time of wire localization is an efficient way to confirm retrieval of intraductal or complex cystic lesions.
The miss rates for excisional biopsy of nonpalpable breast lesions, defined as the lack of partial or complete removal of the lesion, range from 0% to 17.9% ( ). With the use of image-guided core needle biopsies of nonpalpable breast lesions increasing, those lesions undergoing presurgical wire localization for excision may be more subtle ( ). If the lesion is apparent only by sonography, confirmation of excision by specimen radiography may be problematic ( ). Although specimen sonography has been described as a reliable method to confirm excision of breast masses ( ), Mesurolle et al ( ) recently described limitations of specimen sonography. Specifically, small lesions (smaller than 1 cm), particularly in a fatty background, may lead to false-negative specimen sonography. Also, lesions with a fluid component (papillomas) may disappear in the specimen on ex vivo examination and make sonographic confirmation difficult ( ). According to the recent National Comprehensive Cancer Network practice guidelines for breast cancer screening and diagnosis, primary surgical excision is preferred if sonographic findings are of an irregular cyst wall or intracystic mass ( ). Although the accuracy of sonographically guided core biopsy, including large-gauge vacuum-assisted biopsy, has been described ( ), little has been published describing the accuracy or validity of sonographic core biopsy of nonpalpable, cystic, or intraductal lesions <1 cm ( ). Lesions may become obscured by hemorrhage during sonographic core biopsy ( ), potentially limiting sampling of the lesion. The usefulness of metallic marker placement at the time of percutaneous core biopsy, and in patients undergoing neoadjuvant chemotherapy has already been well documented ( ). The purpose of our study is to propose deploying a metallic marker using sonographic guidance immediately before wire localization for excisional biopsy to aid in the identification of intraductal or complex cystic lesions at specimen radiography.
Materials and methods
Institutional review board approval was obtained. Individual patient informed consent for this retrospective study was not required. The study is Health Insurance Portability and Accountability Act compliant.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Jackman R.J., Marzoni F.A.: Needle-localized breast biopsy: why do we fail?. Radiology 1997; 204: pp. 677-684.
2. Hall F.M.: Missed rates for surgical biopsy of needle-localized breast lesions. Radiology 1998; 207: pp. 832.
3. Mesurolle B., El-Khoury M., Hori D., et. al.: Sonography of postexcision specimens of nonpalpable breast lesions: value, limitations, and description of a method. Am J Roentgenol 2006; 186: pp. 1014-1024.
4. Frenna T.H., Meyer J.E., Sonnenfeld M.R.: US of breast biopsy specimens. Radiology 1994; 190: pp. 573.
5. Fornage B.D., Ross M.I., Singletary S.E., et. al.: Localization of impalpable breast masses: value of sonography in the operating room and scanning of excised specimens. Am J Roentgenol 1994; 163: pp. 569-573.
6. Vujovic P., Gianduzzo T., Archibald C., et. al.: Ultrasonic specimen radiography for non-palpable breast lesions. Breast 2002; 11: pp. 144-150.
7. Rissanen T.J., Makarainen H.P., Kiviniemi H.O., et. al.: Ultrasonographically guided wire localization of nonpalpable breast lesions. J Ultrasound Med 1994; 13: pp. 183-188.
8. National Comprehensive Cancer Network: Breast Cancer Screening and Diagnosis Guidelines (v.1.2007). http://www.nccn.org/professionals/physician_gls/PDF/breast-screening.pdf Accessed on June 4, 2008.
9. Parker S.H., Jobe W.E., Dennis M.A., et. al.: US-guided automated large core breast biopsy. Radiology 1993; 187: pp. 507-511.
10. Youk J.H., Kim E.K., Kim M.J., et. al.: Sonographically guided 14 gauge core needle biopsy of breast masses: a review of 2420 cases with long-term follow-up. Am J Roentgenol 2008; 190: pp. 202-207.
11. Simon J.R., Kalbhen C.L., Cooper R.A., et. al.: Accuracy and complication rates of US-guided vacuum-assisted core breast biopsy: initial results. Radiology 2000; 215: pp. 694-697.
12. Cassano E., Uban L.A.B.D., Pizzamiglio M., et. al.: Ultrasound-guided vacuum-assisted core breast biopsy: experience with 406 cases. Breast Cancer Res Treat 2007; 1022: pp. 103-110.
13. Perez-Fuentes J.A., Longobardi I.R., Acosta V.F., et. al.: Sonographically guided directional vacuum-assisted breast biopsy: preliminary experience in Venezuela. Am J Roentgenol 2001; 177: pp. 1459-1463.
14. Philpotts L.E., Hooley R.J., Lee C.H.: Comparison of automated versus vacuum-assisted biopsy methods for sonographically guided core biopsy of the breast. Am J Roentgenol 2003; 180: pp. 347-351.
15. Dennis M.A., Parker S., Kaske T.I., et. al.: Incidental treatment of nipple discharge caused by benign intraductal papilloma through diagnostic mammotome biopsy. Am J Roentgenol 2000; 174: pp. 1263-1268.
16. Phillips S.W., Gabriel H., Comstock C.E., et. al.: Sonographically guided metallic clip placement after core needle biopsy of the breast. Am J Roentgenol 2000; 175: pp. 1353-1355.
17. Liberman L., Dershaw D., Morris E.A., et. al.: Clip placement after stereotactic vacuum-assisted breast biopsy. Radiology 1997; 205: pp. 417-422.
18. Dash N., Chafin S.H., Johnson R.R., et. al.: Usefulness of tissue marker clips in patients undergoing neoadjuvant chemotherapy for breast cancer. Am J Roentgenol 1999; 173: pp. 911-917.
19. American College of Radiology: Breast imaging reporting and data system.4th ed.2003.American College of RadiologyReston, VA
20. Abrahamson P.E., Dunlap L.A., Amamoo A., et. al.: Factor predicting successful needle-localized breast biopsy. Acad Radiol 2003; 10: pp. 601-606.
21. Golub R.M., Bennett C.L., Stinson T., et. al.: Cost minimization study of image-guided core biopsy versus surgical excisional biopsy for women with abnormal mammograms. J Clin Oncol 2004; 22: pp. 2430-2437.
22. White R.R., Halperin T.J., Olson J.A., et. al.: Impact of core-needle biopsy on the surgical management of mammographic abnormalities. Ann Surg 2001; 233: pp. 769-777.
23. Acheson M.B., Patton R.G., Howisey R.L., et. al.: Three- to six year follow-up for 379 benign image-guided large core needle biopsies of nonpalpable breast abnormalities. J Am Coll Surg 2002; 195: pp. 462-466.
24. Lannin D.R., Ponn T., Andrejeva L., et. al.: Should all breast cancers be diagnosed by needle biopsy?. Am J Surg 2006; 192: pp. 450-454.
25. Jackman R.J., Marzoni F.A.: Stereotactic histologic biopsy with patients prone: technical feasibility in 98% of mammographically detected lesions. Am J Roentgenol 2003; 180: pp. 785-794.
26. Chung S.Y., Lee K.W., Park K.S., et. al.: Breast tumors associated with nipple discharge correlation of findings on galactography and sonography. Clin Imaging 1995; 19: pp. 165-171.
27. Lam W.W.M., Chu W.C.W., Tang A.P.Y., et. al.: Role of radiologic features in the management of papillary lesions of the breast. Am J Roentgenol 2006; 186: pp. 1322-1327.
28. Liberman L., Tornos C., Huzjan R., et. al.: is surgical excision warranted after benign, concordant diagnosis of papilloma at percutaneous breast biopsy?. Am J Roentgenol 2006; 186: pp. 1328-1334.
29. Mercado C.L., Hamele-Bena D., Oken S.M., et. al.: Papillary lesions of the breast at percutaneous core-needle biopsy. Radiology 2006; 238: pp. 801-808.
30. Berg W.: Image-guided breast biopsy and management of high-risk lesions. Radiol Clin N Am 2004; 42: pp. 935-946.
31. Ernst M.F., Avenarius A., Schur K.H., et. al.: Wire localization of non-palpable breast lesions: out of date?. Breast 2002; 11: pp. 408-413.
32. Blichert-Toft M., Dyreborg U., et. al.: Nonpalpble breast lesions: mammographic wire-guided biopsy and radiologic-histologic correlation. World J Surg 1982; 2: pp. 119-125.
33. Reid S.E., Scanlon E.F., Bernstein J.R., et. al.: An alternative approach to nonpalpable breast biopsies. J Surg Oncol 1990; 44: pp. 3-96.