
Rationale and Objectives
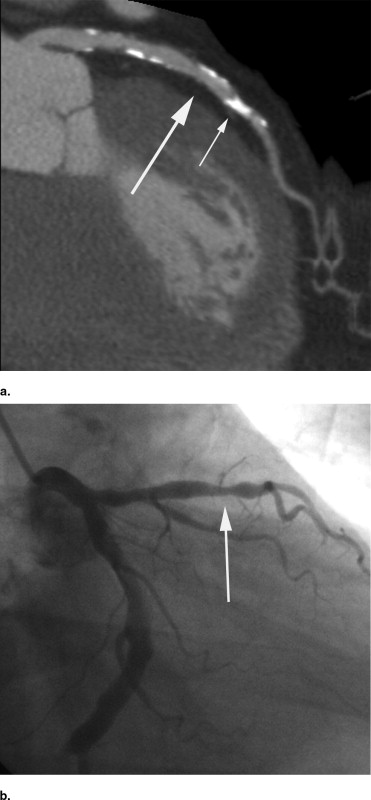
Compare stent size selection using coronary computed tomography angiography (CCTA) to invasive coronary angiography (ICA). CCTA is increasingly performed before cardiac catheterization; however, the utility of incorporating these data into coronary interventions is unknown.
Methods
Retrospective study of 18 consecutive patients with 24 coronary artery lesions evaluated with 64-detector CCTA followed by ICA and resulting stent placement. Two blinded interventional cardiologists independently reviewed designated arterial segments on both CCTA and ICA during different reading sessions and determined anticipated stent length and nominal diameter, maximum stenosis, the need for postdilation of either stent margin, and final proximal and distal stent diameters.
Results
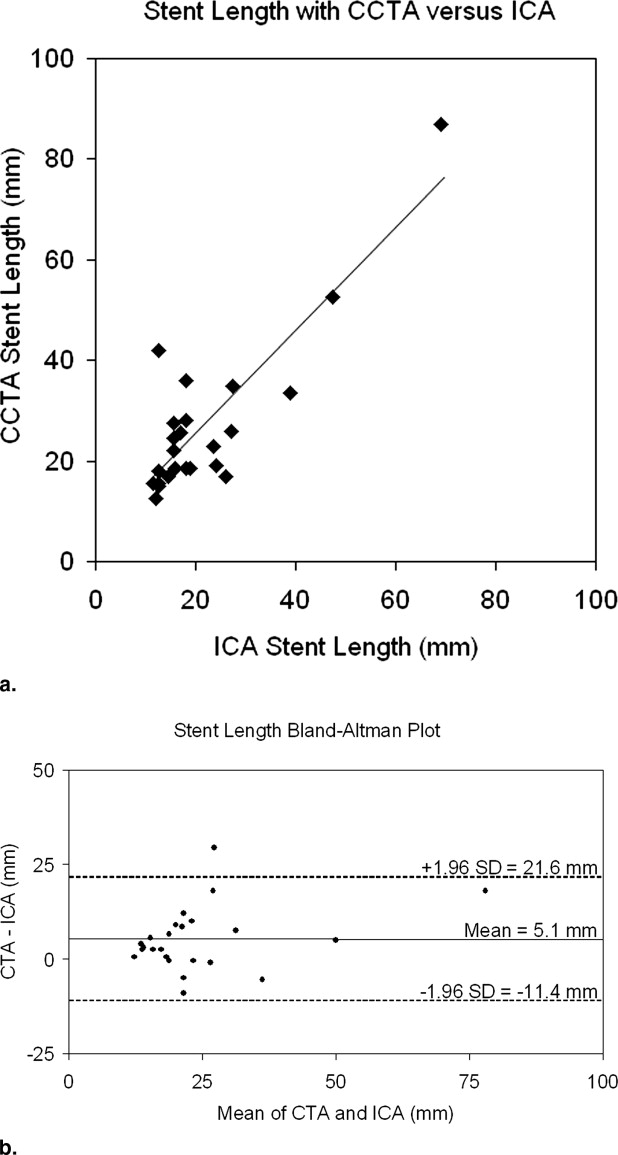
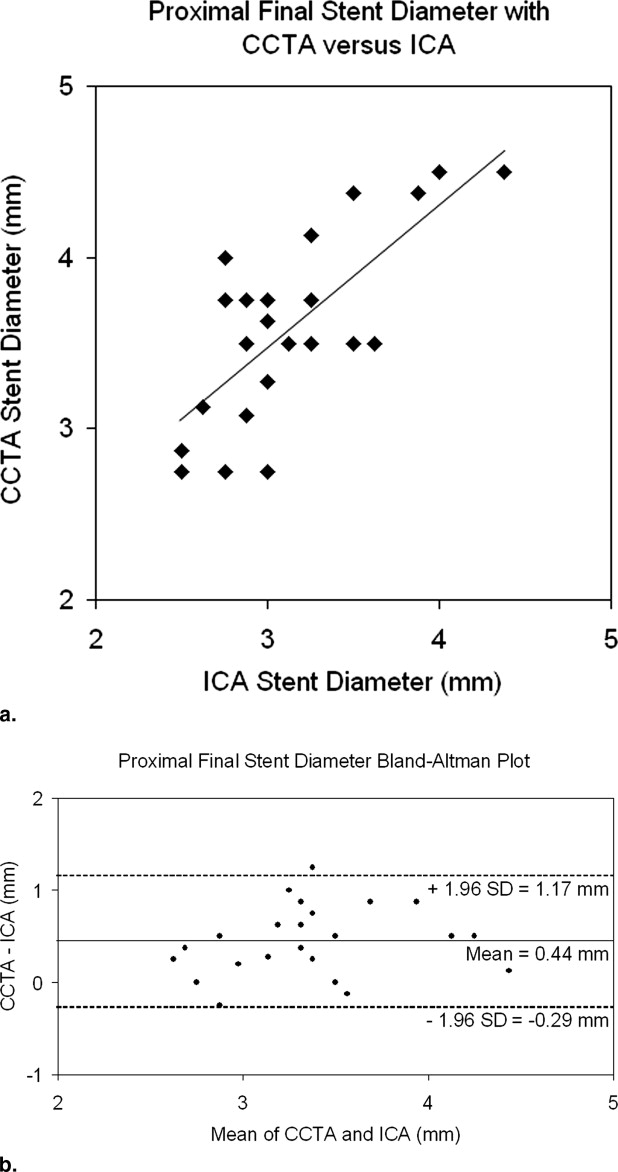
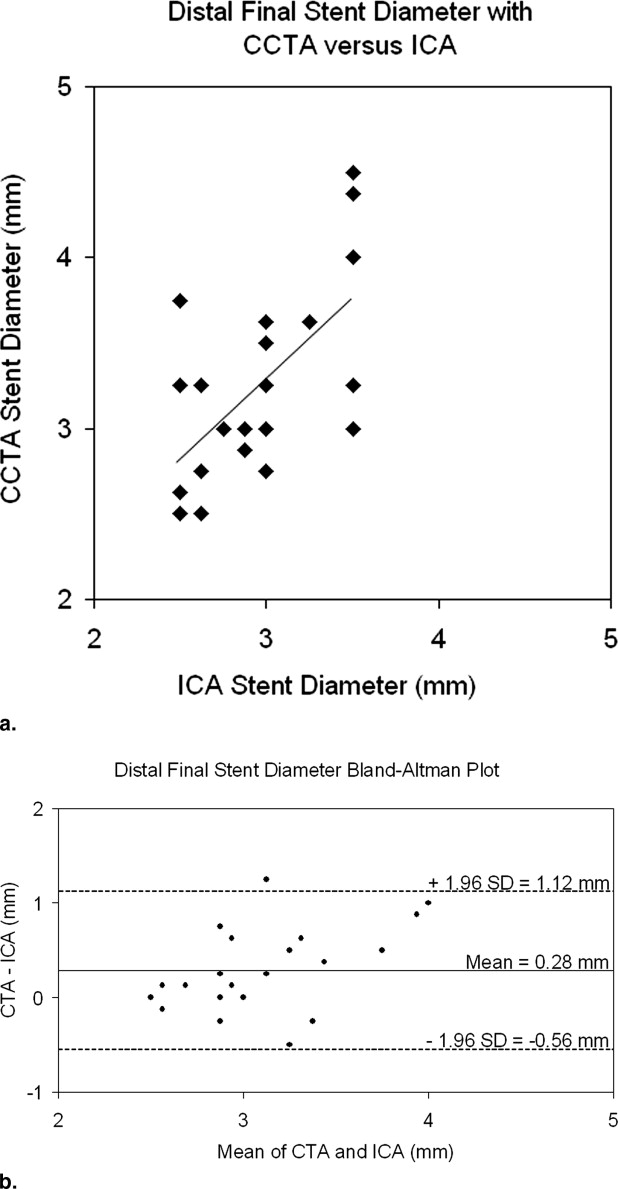
There was strong correlation between CCTA and ICA in the anticipated stent length ( r = 0.85, P < .001) and final stent diameter (proximal end r = 0.74, P < .001; distal end r = 0.63, P = .001). Anticipated stent length was longer with CCTA compared to ICA (27.0 ± 16.0 vs. 21.8 ± 13.3 mm; P = .006). The final stent diameters were larger with CCTA compared to ICA, both at the proximal end (3.6 ± 0.5 vs. 3.1 ± 0.5 mm; P < .001) and distal end (3.2 ± 0.6 vs. 2.9 ± 0.4 mm; P = .004).
Conclusions
Using 64-detector CCTA, interventional cardiologists select longer stents with larger final stent diameters than with ICA. Further studies are needed to determine the clinical utility of incorporating CCTA, when available, in defining interventional strategy.
Cardiovascular disease is the leading cause of death in the United States, with coronary artery disease (CAD) diagnosed in more than 13 million American adults. Invasive coronary angiography (ICA) is the reference standard for the diagnosis of CAD, and in 2003 there were more than 1.4 million diagnostic coronary angiograms and 664,000 percutaneous coronary interventions (PCI) performed in the United States ( ). Coronary computed tomography angiography (CCTA) provides noninvasive imaging of the coronary arteries, is rapidly growing in use, and now has established appropriateness indications ( ). As its use increases, more patients undergoing PCI will have had prior CCTA.
In patients who have CCTA and subsequent ICA with PCI, the added utility of incorporating CCTA data into the interventional strategy has not been evaluated. ICA has major limitations given its two-dimensional view of a three-dimensional structure ( ). CCTA is able to visualize the lumen in any dimension and can characterize plaque and the coronary artery wall morphology. It may provide a more accurate estimation of the vessel wall diameter and lesion length, potentially allowing for more accurate stent size selection. This could result in less size mismatch between the stent and vessel wall and allow optimal placement of the stent margins in relatively disease-free segments. Although intravascular ultrasound (IVUS) can also provide some of this information, it is associated with increased cost, a small increased risk of adverse events ( ), and longer procedural time, all of which limit its routine clinical use.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CCTA Technique and Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
ICA Technique and Image Analysis
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Thom T., Haase N., Rosamond W., et. al., American Heart Association Statistics Committee, Stroke Statistics Subcommittee: Heart disease and stroke statistics—2006 update. Circulation 2006; 113: pp. e51-e85.
2. ACCF/ACR/SCCT/SCMR/ASNC/NASCI/SCAI/SIR 2006 appropriateness criteria for cardiac computed tomography and cardiac magnetic resonance imaging: a report of the American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group, American College of Radiology, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, American Society of Nuclear Cardiology, North American Society for Cardiac Imaging, Society for Cardiovascular Angiography and Interventions, and Society of Interventional Radiology. J Am Coll Cardiol 2006; 48: pp. 1475-1497.
3. Topol E.J., Nissen S.E.: Our preoccupation with coronary luminology. Circulation 1995; 92: pp. 2333-2342.
4. Hausmann D., Erbel R., Alibelli-Chemarin M.J., et. al.: The safety of intracoronary ultrasound. Circulation 1995; 91: pp. 623-630.
5. Pfisterer M., Brunner-La Rocca H.P., Buser P.T., et. al., BASKET-LATE Investigators: Late clinical events after clopidogrel discontinuation may limit the benefit of drug-eluting stents: an observational study of drug-eluting versus bare-metal stents. J Am Coll Cardiol 2006; 48: pp. 2584-2591.
6. Airoldi F., Colombo A., Morici N., et. al.: Incidence and predictors of drug-eluting stent thrombosis during and after discontinuation of thienopyridine treatment. Circulation 2007; 116: pp. 745-754.
7. Stettler C., Wandel S., Allemann S., et. al.: Outcomes associated with drug-eluting and bare-metal stents: a collaborative network meta-analysis. Lancet 2007; 370: pp. 937-948.
8. Fujii K., Carlier S.G., Mintz G.S., et. al.: Stent underexpansion and residual reference segment stenosis are related to stent thrombosis after sirolimus-eluting stent implantation. J Am Coll Cardiol 2005; 45: pp. 995-998.
9. Sun Z., Jiang W.: Diagnostic value of multislice computed tomography angiography in coronary artery disease: a meta-analysis. Eur J Radiol 2006; 60: pp. 279-286.
10. Cordeiro M.A., Lima J.A.: Atherosclerotic plaque characterization by multidetector row computed tomography angiography. J Am Coll Cardiol 2006; 47: pp. C40-C47.
11. Sinha A.M., Mahnken A.H., Borghans A., et. al.: Multidetector-row computed tomography vs. angiography and intravascular ultrasound for the evaluation of the diameter of proximal coronary arteries. Int J Cardiol 2006; 110: pp. 40-45.
12. Achenbach S., Ulzheimer S., Baum U., et. al.: Noninvasive coronary angiography by retrospectively ECG-gated multislice spiral CT. Circulation 2000; 102: pp. 2823-2828.
13. Moselewski F., Ropers D., Pohle K., et. al.: Comparison of measurement of cross-sectional coronary atherosclerotic plaque and vessel areas by 16-slice multidetector computed tomography versus intravascular ultrasound. Am J Cardiol 2004; 94: pp. 1294-1297.
14. Leber A.W., Knez A., von Ziegler F., et. al.: Quantification of obstructive and nonobstructive coronary lesions by 64-slice computed tomography. J Am Coll Cardiol 2005; 46: pp. 147-154.
15. Gregory S.A., Ferencik M., Achenbach S., et. al.: Comparison of sixty-four-slice multidetector computed tomographic coronary angiography to coronary angiography with intravascular ultrasound for the detection of transplant vasculopathy. Am J Cardiol 2006; 98: pp. 877-884.
16. Oemrawsingh P.V., Mintz G.S., Schalij M.J., et. al.: Intravascular ultrasound guidance improves angiographic and clinical outcome of stent implantation for long coronary artery stenoses. Circulation 2003; 107: pp. 62-67.