
Rationale and Objectives
Core needle biopsy results of segmental calcifications on mammography can have direct impact on surgical management. Although dependent on breast size, cancer spanning greater than 5 cm is usually treated with mastectomy, and cancer less than 5 cm is managed with lumpectomy. Approach to stereotactic biopsy of morphologically similar segmental calcifications that span more than 5 cm on mammography varies geographically and is currently largely based on preference of the surgical or medical oncology colleagues. Some clinicians prefer biopsy of the anterior and posterior aspects of the abnormality, whereas others believe a single biopsy within the abnormality is adequate. There is insufficient data to support whether a single biopsy of calcifications is adequate to establish the need for mastectomy, or if pathology-proven cancer in the anterior and posterior components to define the extent of disease is required. This study aims to evaluate concordance rates of paired biopsies of suspicious segmental mammographic calcifications.
Materials and Methods
From a 5-year review of our imaging database, 32 subjects were identified with breast imaging reporting and data system (BI-RADS) 4 or 5 segmental calcifications on mammography who underwent anterior and posterior stereotactic biopsies. The paired biopsy results were independently analyzed for concordance on benign, high-risk, or malignant pathology.
Results
Of the 32 cases, there was perfect agreement (32/32 cases = 100% concordance, 95% confidence interval = 89.3–100%) in anterior and posterior pairs in benign, high-risk, or malignant findings (kappa = 1, P < 0.001).
Conclusions
The absence of data on pathological concordance in anterior and posterior aspects of suspicious, morphologically similar, segmental calcifications spanning 5 cm or more has led to a varied clinical approach to stereotactic biopsy. The 100% rate of pathological concordance in our study suggests that a single biopsy is adequate for diagnosis and representative of the whole mammographic abnormality. Implementation of this approach will potentially reduce unnecessary biopsies and surgeries, minimize healthcare costs, and decrease patient morbidity.
Introduction
Stereotactic biopsy has been established as an accurate image-guided method for the evaluation of indeterminate or suspicious calcifications visualized on mammography. Most biopsies involve a single group of calcifications that measure less than 2 cm in size. If this group of calcifications is found to represent malignancy, and no additional disease is identified in that breast, the patient is usually a candidate for breast conservation therapy with lumpectomy and radiation. In groups of calcifications spanning more than 5 cm, pathology from biopsy can have a direct impact on the decision for lumpectomy versus mastectomy as cancer spanning greater than 5 cm is usually treated with mastectomy.
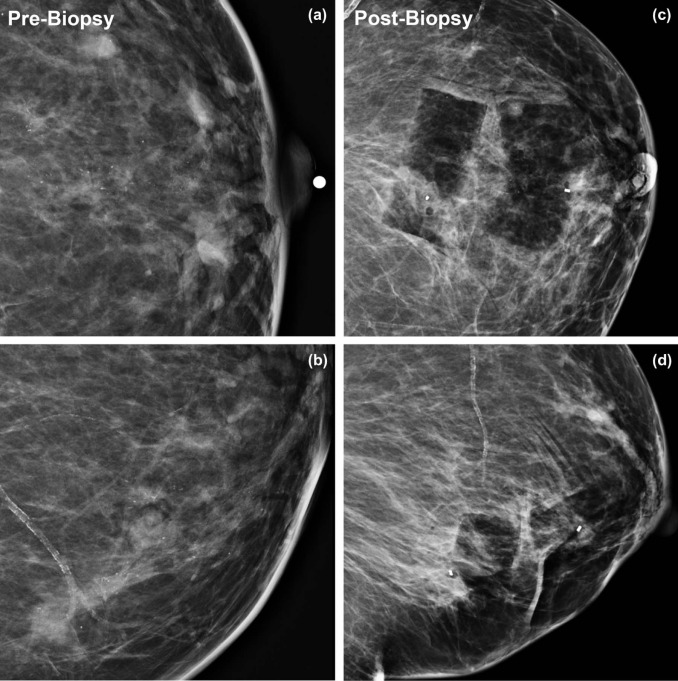
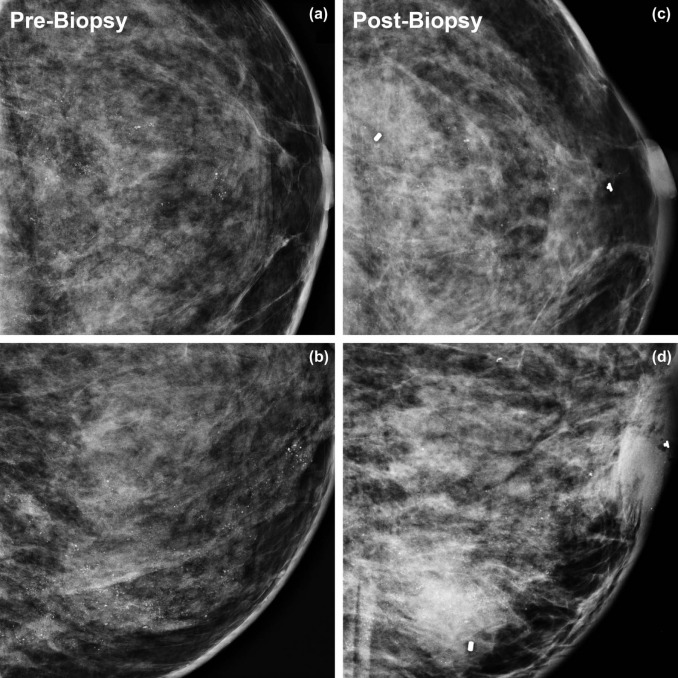
If abnormal groups of calcifications are located in different quadrants of the breast, it is generally accepted that each of the areas of calcifications must be biopsied to establish multicentric disease and the need for mastectomy. However, if the calcifications are a continuous abnormality in a segmental distribution that span 5 cm or more ( Fig 1 ), there are varying views on how to approach the biopsy of these calcifications. Some clinicians believe that given the contiguous nature and morphologically similar appearance of the calcifications, sampling a single site within the calcifications would be representative of the entire abnormality, thus sparing the patient the morbidity and cost of a second biopsy. Other clinicians find it necessary to biopsy both the anterior and the posterior aspects of the abnormality to provide pathology-proven malignancy before sending the patient for mastectomy, rather than assuming homogeneous pathology from a single sample.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Agreement Between Anterior and Posterior Biopsy Pairs
Posterior biopsy Total Benign High-risk Malignant Anterior biopsy Benign 9 0 0 9 High-risk 0 10 0 10 Malignant 0 0 13 13 Total 9 10 13 32
CI, confidence interval.
Perfect agreement (kappa = 1, P < 0.001) in anterior and posterior biopsy pairs in benign (B), high-risk (H), or malignant (M) findings with 100% concordance (32/32 cases; 95% CI = 89.3–100%).
Table 2
Pathology From Anterior and Posterior Biopsies of Segmental Calcifications Spanning Greater than 5 cm
Patient Anterior Pathology Posterior Pathology B/H/M 1 DCIS DCIS M 2 DCIS DCIS M 3 ADH ADH H 4 ADH ADH H 5 ADH ADH H 6 DCIS DCIS M 7 ADH ADH H 8 Fibrosis Fibrosis B 9 DCIS DCIS M 10 Columnar cell change Columnar cell change B 11 Columnar cell change Columnar cell change B 12 Apocrine metaplasia Apocrine metaplasia H 13 Columnar cell change Columnar cell change B 14 ALH ALH H 15 Stromal fibrosis Stromal fibrosis B 16 IDC IDC M 17 ADH ADH H 18 ADH ADH H 19 Fibroadenoma Fibroadenoma B 20 Columnar cell change Columnar cell change B 21 ADH ADH H 22 DCIS DCIS M 23 DCIS DCIS M 24 DCIS IDC M 25 Columnar cell change Columnar cell change B 26 Calcium oxalate Calcium oxalate B 27 DCIS DCIS M 28 DCIS DCIS M 29 DCIS DCIS M 30 DCIS DCIS M 31 ADH ADH H 32 DCIS DCIS M
DCIS, ductal carcinoma in situ; IDC, invasive ductal carcinoma.
Histopathology results from anterior and posterior biopsy pairs and categorized as benign (B), high-risk (H), or malignant (M) categories.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Implications for Patient Care
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. American Cancer Society : Cancer facts and figures 2015.2015.American Cancer SocietyAtlanta, GA
2. Liberman L., LaTrenta L.R., Van Zee K.J., et. al.: Stereotactic core biopsy of calcifications highly suggestive of malignancy. Radiology 1997; 203: pp. 673-677.
3. Michelle A.: CPT 2014: current procedural terminology.2013.American Medical AssociationChicago Professional ed
4. ACR Imaging 3.0. Available at: http://www.acr.org/Advocacy/Economics-Health-Policy/Imaging-3 Accessed October 1, 2015
5. Nagashima T., Hashimoto H., Oshida K., et. al.: Ultrasound demonstration of mammographically detected microcalcifications in patients with ductal carcinoma in situ of the breast. Breast Cancer 2005; 12: pp. 216-220.