
Radiology reports are vital for patient care as referring physicians depend upon them for deciding appropriate patient management. Traditional narrative reports are associated with excessive variability in the language, length, and style, which can minimize report clarity and make it difficult for referring clinicians to identify key information needed for patient care. Structured reporting has been advocated as a potential solution for improving the quality of radiology reports. The Association of University Radiologists—Radiology Research Alliance Structured Reporting Task Force convened to explore the current and future role of structured reporting in radiology and summarized its finding in this article. We review the advantages and disadvantages of structured radiology reports and discuss the current prevailing sentiments among radiologists regarding structured reports. We also discuss the obstacles to the use of structured reports and highlight ways to overcome some of those challenges. We also discuss the future directions in radiology reporting in the era of personalized medicine.
Introduction
The radiology report is vital for patient management. Radiologists play a major role in patient care by the accurate interpretation of imaging studies and appropriate communication of imaging findings to referring physicians. Although some referring clinicians may interpret imaging studies by themselves, radiologists’ reports have been shown to be more accurate and comprehensive, resulting in improved patient care . To improve patient care, it is imperative for the reports to be timely and accurate and to answer the clinical question. For a health-care system, these may be the most important, readily available metrics by which the value of radiology service could be measured.
Although learning how to report imaging studies is an essential component of radiology residency training programs, formal training on how to frame a radiology report often receives less than 1 hour/year . Instead, most trainees learn the art of reporting by observing faculty, senior residents, fellows, and peers.
Traditionally, radiology reports were created using free-text, narrative language. Studies show that the use of nonstructured reports using narrative language may serve as an obstacle to optimal patient care. Excessive variability in language, length, and style can minimize report clarity, making it difficult for referring physicians to identify key information needed for patient care .
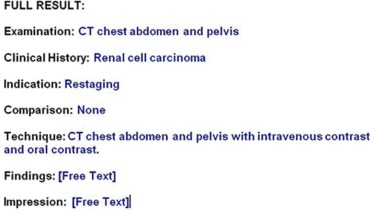
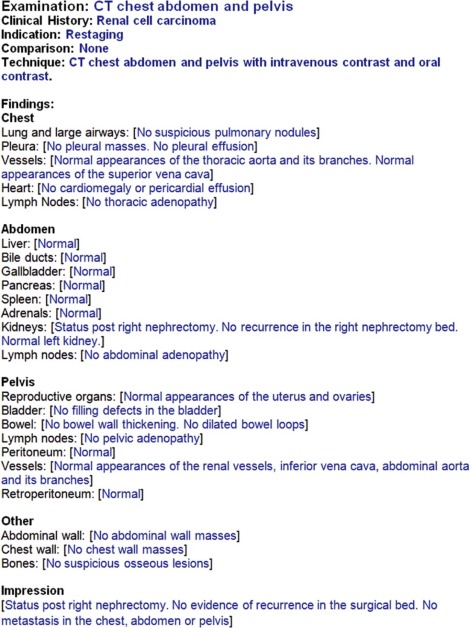
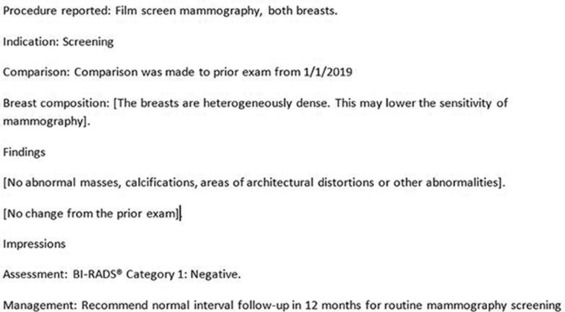
Structured reporting has been advocated as a potential solution for improving the quality of radiology reports. A tiered approach to structured reporting has been described . At its basic level, a structured report should be organized with headings, such as clinical history, indication, technique, findings, and impression ( Fig 1 ). The next tier of structured reports is where the “findings” section is organized with subheadings, such as the various organs (or anatomic structures) imaged ( Fig 2 ). At the highest tier, the structured radiology report has all of the previously mentioned characteristics and uses a standardized language based on a universally accepted lexicon ( Fig 3 ). Increasingly, academic centers are using structured radiology reports containing templates, macros, or prepopulated checklists.
Get Radiology Tree app to read full this article<
Advantages of Structured Reporting
Get Radiology Tree app to read full this article<
Table 1
Benefits and Limitations of Structured Radiology Reports
Benefits Limitations and Challenges Disease-specific report templates can improve report clarity and quality, and ensure consistent use of terminology across practices. Radiologists may be resistant to change. Checklist style reports can reduce diagnostic errors (such as failing to report incidental renal cell carcinoma in a magnetic resonance spine performed for back pain). Learning curve associated with new reporting style may negatively impact radiology workflow and productivity. Can reduce grammatical and nongrammatical digital speech recognition errors Potentially increased error rates if used improperly (eg, failing to remove the prepopulated phrase of “normal gallbladder” in a patient who is status post cholecystectomy). Ensures completeness of radiology report documentation and thereby improves radiology reimbursement Interruption of visual search pattern may increase reporting time. May be financially rewarding under the new Medicare Merit-based Incentive Payment System Including unnecessary or irrelevant information in a template report may negatively impact the coherence of the report and its subsequent comprehension by referring physicians. Positively impacts research in radiology by facilitating data mining Provides opportunities for quality improvement Can help promote evidence-based medicine by integrating clinical decision support tools with radiology reports
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Obstacles to Structured Reporting
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Overcoming Challenges
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Future Directions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Alfaro D., Levitt M.A., English D.K., et. al.: Accuracy of interpretation of cranial computed tomography scans in an emergency medicine residency program. Ann Emerg Med 1995; 25: pp. 169-174.
2. Arhami Dolatabadi A., Baratloo A., Rouhipour A., et. al.: Interpretation of computed tomography of the head: emergency physicians versus radiologists. Trauma Mon 2013; 18: pp. 86-89.
3. Gatt M.E., Spectre G., Paltiel O., et. al.: Chest radiographs in the emergency department: is the radiologist really necessary?. Postgrad Med J 2003; 79: pp. 214-217.
4. Kang M.J., Sim M.S., Shin T.G., et. al.: Evaluating the accuracy of emergency medicine resident interpretations of abdominal CTs in patients with non-traumatic abdominal pain. J Korean Med Sci 2012; 27: pp. 1255-1260.
5. Weiner S.N.: Radiology by nonradiologists: is report documentation adequate?. Am J Manag Care 2005; 11: pp. 781-785.
6. Sistrom C., Lanier L., Mancuso A.: Reporting instruction for radiology residents. Acad Radiol 2004; 11: pp. 76-84.
7. Bosmans J.M., Weyler J.J., Parizel P.M.: Structure and content of radiology reports, a quantitative and qualitative study in eight medical centers. Eur J Radiol 2009; 72: pp. 354-358.
8. Heikkinen K., Loyttyniemi M., Kormano M.: Structure and content of 400 CT reports in four teaching hospitals using a new, Windows-based software tool. Acta Radiol 2000; 41: pp. 102-105.
9. Naik S.S., Hanbidge A., Wilson S.R.: Radiology reports: examining radiologist and clinician preferences regarding style and content. AJR Am J Roentgenol 2001; 176: pp. 591-598.
10. Wallis A., McCoubrie P.: The radiology report—are we getting the message across?. Clin Radiol 2011; 66: pp. 1015-1022.
11. Bosmans J.M., Peremans L., Menni M., et. al.: Structured reporting: if, why, when, how-and at what expense? Results of a focus group meeting of radiology professionals from eight countries. Insights Imaging 2012; 3: pp. 295-302.
12. Weiss D.L., Langlotz C.P.: Structured reporting: patient care enhancement or productivity nightmare?. Radiology 2008; 249: pp. 739-747.
13. Bosmans J.M., Neri E., Ratib O., et. al.: Structured reporting: a fusion reactor hungry for fuel. Insights Imaging 2015; 6: pp. 129-132.
14. Bender L.C., Linnau K.F., Meier E.N., et. al.: Interrater agreement in the evaluation of discrepant imaging findings with the Radpeer system. AJR Am J Roentgenol 2012; 199: pp. 1320-1327.
15. Borgstede J.P., Lewis R.S., Bhargavan M., et. al.: RADPEER quality assurance program: a multifacility study of interpretive disagreement rates. Journal of the American College of Radiology : JACR. 2004; 1: pp. 59-65.
16. Donald J.J., Barnard S.A.: Common patterns in 558 diagnostic radiology errors. J Med Imaging Radiat Oncol 2012; 56: pp. 173-178.
17. Hsu W., Han S.X., Arnold C.W., et. al.: A data-driven approach for quality assessment of radiologic interpretations. J Am Med Inform Assoc 2016; 23: pp. e152-e156.
18. McCreadie G., Oliver T.B.: Eight CT lessons that we learned the hard way: an analysis of current patterns of radiological error and discrepancy with particular emphasis on CT. Clin Radiol 2009; 64: pp. 491-499. discussion 500–501
19. Berlin L., Berlin J.W.: Malpractice and radiologists in Cook County, IL: trends in 20 years of litigation. AJR Am J Roentgenol 1995; 165: pp. 781-788.
20. Halpin S.F.: Medico-legal claims against English radiologists: 1995–2006. Br J Radiol 2009; 82: pp. 982-988.
21. Pinto A., Acampora C., Pinto F., et. al.: Learning from diagnostic errors: a good way to improve education in radiology. Eur J Radiol 2011; 78: pp. 372-376.
22. Thomson N.B., Patel M.: Radiology liability update: review of claims, trends, high-risk conditions and practices, and tort reform alternatives. J Am Coll Radiol 2012; 9: pp. 729-733.
23. Lee C.S., Nagy P.G., Weaver S.J., et. al.: Cognitive and system factors contributing to diagnostic errors in radiology. AJR Am J Roentgenol 2013; 201: pp. 611-617.
24. Graber M.L., Wachter R.M., Cassel C.K.: Bringing diagnosis into the quality and safety equations. JAMA 2012; 308: pp. 1211-1212.
25. Lin E., Powell D.K., Kagetsu N.J.: Efficacy of a checklist-style structured radiology reporting template in reducing resident misses on cervical spine computed tomography examinations. J Digit Imaging 2014; 27: pp. 588-593.
26. Quattrocchi C.C., Giona A., Di Martino A.C., et. al.: Extra-spinal incidental findings at lumbar spine MRI in the general population: a large cohort study. Insights Imaging 2013; 4: pp. 301-308.
27. Semaan H.B., Bieszczad J.E., Obri T., et. al.: Incidental extraspinal findings at lumbar spine magnetic resonance imaging: a retrospective study. Spine 2015; 40: pp. 1436-1443.
28. McKee B.J., Regis S.M., McKee A.B., et. al.: Performance of ACR Lung-RADS in a clinical CT lung screening program. J Am Coll Radiol 2015; 12: pp. 273-276.
29. Rosskopf A.B., Dietrich T.J., Hirschmann A., et. al.: Quality management in musculoskeletal imaging: form, content, and diagnosis of knee MRI reports and effectiveness of three different quality improvement measures. AJR Am J Roentgenol 2015; 204: pp. 1069-1074.
30. Ghoshhajra B.B., Lee A.M., Ferencik M., et. al.: Interpreting the interpretations: the use of structured reporting improves referring clinicians’ comprehension of coronary CT angiography reports. J Am Coll Radiol 2013; 10: pp. 432-438.
31. Brook O.R., Brook A., Vollmer C.M., et. al.: Structured reporting of multiphasic CT for pancreatic cancer: potential effect on staging and surgical planning. Radiology 2015; 274: pp. 464-472.
32. Marcal L.P., Fox P.S., Evans D.B., et. al.: Analysis of free-form radiology dictations for completeness and clarity for pancreatic cancer staging. Abdom Imaging 2015; 40: pp. 2391-2397.
33. Sahni V.A., Silveira P.C., Sainani N.I., et. al.: Impact of a structured report template on the quality of MRI reports for rectal cancer staging. AJR Am J Roentgenol 2015; 205: pp. 584-588.
34. Gunn A.J., Alabre C.I., Bennett S.E., et. al.: Structured feedback from referring physicians: a novel approach to quality improvement in radiology reporting. AJR Am J Roentgenol 2013; 201: pp. 853-857.
35. Hawkins C.M., Hall S., Hardin J., et. al.: Prepopulated radiology report templates: a prospective analysis of error rate and turnaround time. J Digit Imaging 2012; 25: pp. 504-511.
36. McGurk S., Brauer K., Macfarlane T.V., et. al.: The effect of voice recognition software on comparative error rates in radiology reports. Br J Radiol 2008; 81: pp. 767-770.
37. Hawkins C.M., Hall S., Zhang B., et. al.: Creation and implementation of department-wide structured reports: an analysis of the impact on error rate in radiology reports. J Digit Imaging 2014; 27: pp. 581-587.
38. Duszak R., Nossal M., Schofield L., et. al.: Physician documentation deficiencies in abdominal ultrasound reports: frequency, characteristics, and financial impact. J Am Coll Radiol 2012; 9: pp. 403-408.
39. Faggioni L., Coppola F., Ferrari R., et. al.: Usage of structured reporting in radiological practice: results from an Italian online survey. Eur Radiol 2017; 27: pp. 1934-1943.
40. Powell D.K., Silberzweig J.E.: State of structured reporting in radiology, a survey. Acad Radiol 2015; 22: pp. 226-233.
41. Bosmans J.M., Weyler J.J., De Schepper A.M., et. al.: The radiology report as seen by radiologists and referring clinicians: results of the COVER and ROVER surveys. Radiology 2011; 259: pp. 184-195.
42. Gunderman R.B., McNeive L.R.: Is structured reporting the answer?. Radiology 2014; 273: pp. 7-9.
43. Srinivasa Babu A., Brooks M.L.: The malpractice liability of radiology reports: minimizing the risk. Radiographics 2015; 35: pp. 547-554.
44. Winter T.C.: The propaedeutics of structured reporting. Radiology 2015; 275: pp. 309-310.
45. Hall F.M.: The radiology report of the future. Radiology 2009; 251: pp. 313-316.
46. Manoonchai N., Kaewlai R., Wibulpolprasert A., et. al.: Satisfaction of imaging report rendered in emergency setting: a survey of radiology and referring physicians. Acad Radiol 2015; 22: pp. 760-770.
47. Krupinski E.A., Hall E.T., Jaw S., et. al.: Influence of radiology report format on reading time and comprehension. J Digit Imaging 2012; 25: pp. 63-69.
48. Sistrom C.L., Honeyman-Buck J.: Free text versus structured format: information transfer efficiency of radiology reports. AJR Am J Roentgenol 2005; 185: pp. 804-812.
49. Johnson A.J., Chen M.Y., Swan J.S., et. al.: Cohort study of structured reporting compared with conventional dictation. Radiology 2009; 253: pp. 74-80.
50. Vache T., Bratan F., Mege-Lechevallier F., et. al.: Characterization of prostate lesions as benign or malignant at multiparametric MR imaging: comparison of three scoring systems in patients treated with radical prostatectomy. Radiology 2014; 272: pp. 446-455.
51. Houssami N., Boyages J., Stuart K., et. al.: Quality of breast imaging reports falls short of recommended standards. Breast 2007; 16: pp. 271-279.
52. Margolies L.R., Pandey G., Horowitz E.R., et. al.: Breast imaging in the era of big data: structured reporting and data mining. AJR Am J Roentgenol 2016; 206: pp. 259-264.
53. Radiology reporting initiative. Available at: https://www.rsna.org/Reporting_Initiative.aspx
54. Morgan T.A., Helibrun M.E., Kahn C.E.: Reporting initiative of the Radiological Society of North America: progress and new directions. Radiology 2014; 273: pp. 642-645.
55. RadReport template library. Available at: http://www.radreport.org/
56. Al-Hawary M.M., Francis I.R., Chari S.T., et. al.: Pancreatic ductal adenocarcinoma radiology reporting template: consensus statement of the Society of Abdominal Radiology and the American Pancreatic Association. Gastroenterology 2014; 146: pp. 291-304. e1
57. Larson D.B., Towbin A.J., Pryor R.M., et. al.: Improving consistency in radiology reporting through the use of department-wide standardized structured reporting. Radiology 2013; 267: pp. 240-250.
58. Anderson T.J., Lu N., Brook O.R.: Disease-specific report templates for your practice. J Am Coll Radiol 2017; 14: pp. 1055-1057.
59. Goldberg-Stein S., Walter W.R., Amis E.S., et. al.: Implementing a structured reporting initiative using a collaborative multistep approach. Curr Probl Diagn Radiol 2016; 46: pp. 295-299.
60. 2016 radiology preferred specialty measure set. Available at: https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/downloads/Radiology_Specialty_Measure_Set.pdf
61. Choksi V.R., Marn C.S., Bell Y., et. al.: Efficiency of a semiautomated coding and review process for notification of critical findings in diagnostic imaging. AJR Am J Roentgenol 2006; 186: pp. 933-936.
62. Zafar H.M., Chadalavada S.C., Kahn C.E., et. al.: Code abdomen: an assessment coding scheme for abdominal imaging findings possibly representing cancer. J Am Coll Radiol 2015; 12: pp. 947-950.
63. Sevenster M., Travis A.R., Ganesh R.K., et. al.: Improved efficiency in clinical workflow of reporting measured oncology lesions via PACS-integrated lesion tracking tool. AJR Am J Roentgenol 2015; 204: pp. 576-583.
64. Zimmerman S.L., Kim W., Boonn W.W.: Informatics in radiology: automated structured reporting of imaging findings using the AIM standard and XML. Radiographics 2011; 31: pp. 881-887.
65. Alkasab T.K., Bizzo B.C., Berland L.L., et. al.: Creation of an open framework for point-of-care computer-assisted reporting and decision support tools for radiologists. J Am Coll Radiol 2017; 14: pp. 1184-1189.
66. Taylor A.T., Garcia E.V.: Computer-assisted diagnosis in renal nuclear medicine: rationale, methodology, and interpretative criteria for diuretic renography. Semin Nucl Med 2014; 44: pp. 146-158.
67. Wang K.C., Jeanmenne A., Weber G.M., et. al.: An online evidence-based decision support system for distinguishing benign from malignant vertebral compression fractures by magnetic resonance imaging feature analysis. J Digit Imaging 2011; 24: pp. 507-515.
68. Sadigh G., Hertweck T., Kao C., et. al.: Traditional text-only versus multimedia-enhanced radiology reporting: referring physicians’ perceptions of value. J Am Coll Radiol 2015; 12: pp. 519-524.
69. Nayak L., Beaulieu C.F., Rubin D.L., et. al.: A picture is worth a thousand words: needs assessment for multimedia radiology reports in a large tertiary care medical center. Acad Radiol 2013; 20: pp. 1577-1583.
70. Oh S.C., Cook T.S., Kahn C.E.: PORTER: a prototype system for patient-oriented radiology reporting. J Digit Imaging 2016; 29: pp. 450-454.
71. Vining D., Salem U., Duran C., et. al.: Development of the ViSion Ontology for Structured Reporting. Radiological Society of North America 2013 Scientific Assembly and Annual Meeting, December 1–December 6, 2013, Chicago IL; Available at: http://archive.rsna.org/2013/13023813.html