
Rationale and Objectives
The purpose of this study was to evaluate the noise and image quality of images reconstructed with a knowledge-based iterative model reconstruction (knowledge-based IMR) in ultra-low dose cardiac computed tomography (CT).
Materials and Methods
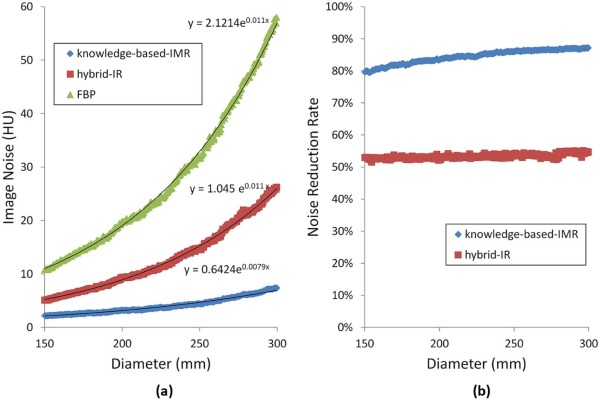
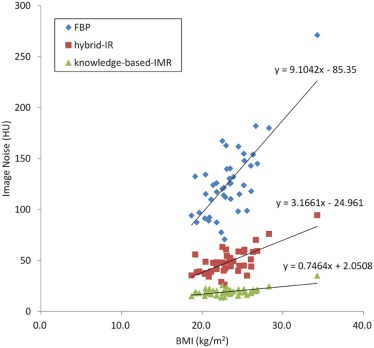
We performed submillisievert radiation dose coronary CT angiography on 43 patients. We also performed a phantom study to evaluate the influence of object size with the automatic exposure control phantom. We reconstructed clinical and phantom studies with filtered back projection (FBP), hybrid iterative reconstruction (hybrid IR), and knowledge-based IMR. We measured effective dose of patients and compared CT number, image noise, and contrast noise ratio in ascending aorta of each reconstruction technique. We compared the relationship between image noise and body mass index for the clinical study, and object size for phantom study.
Results
The mean effective dose was 0.98 ± 0.25 mSv. The image noise of knowledge-based IMR images was significantly lower than those of FBP and hybrid IR images (knowledge-based IMR: 19.4 ± 2.8; FBP: 126.7 ± 35.0; hybrid IR: 48.8 ± 12.8, respectively) ( P < .01). The contrast noise ratio of knowledge-based IMR images was significantly higher than those of FBP and hybrid IR images (knowledge-based IMR: 29.1 ± 5.4; FBP: 4.6 ± 1.3; hybrid IR: 13.1 ± 3.5, respectively) ( P < .01). There were moderate correlations between image noise and body mass index in FBP (r = 0.57, P < .01) and hybrid IR techniques (r = 0.42, P < .01); however, these correlations were weak in knowledge-based IMR (r = 0.27, P < .01).
Conclusion
Compared to FBP and hybrid IR, the knowledge-based IMR offers significant noise reduction and improvement in image quality in submillisievert radiation dose cardiac CT.
Introduction
Attention has recently focused on the potential risks of radiation-induced carcinogenesis from computed tomography (CT) . Although cardiac CT using multidetector CT scanners (MDCT) yields high diagnostic accuracy for the evaluation of coronary artery stenosis and cardiac function, radiation exposure is of concern . According to Hausleiter et al. the mean effective dose (ED) in cardiac CT was 12 mSv; the range was 5–30 mSv about 10 years ago . Low-dose coronary CT angiography (CTA) has recently been performed in several studies ; however, the increased image noise has been a concern, potentially impacting the diagnostic confidence in CTA.
An iterative reconstruction (IR) algorithm was used in the early years of CT but was given up because of the higher computational demands compared to the filtered back projection (FBP) reconstruction algorithms; however, an IR was restored to help reduce the quantum noise at low radiation dose scan . Recent studies suggested the IR technique is well suited for the low-dose cardiac CT . However, these early IR techniques were based on the several simplistic assumptions of the CT system, and the next evolution of the IR technique included a more sophisticated modeling of the real CT system (physical/system models). The knowledge-based iterative model reconstruction (knowledge-based IMR, Philips Healthcare, Cleveland, OH) algorithm is the latest IR technique that includes statistical and physical/system models with a specialized cost function for cardiac, brain, body examinations, and the like. Phantom studies and preliminary clinical studies revealed some promising results from another model-based IR algorithm , but there are only few clinical studies that evaluated the usability of knowledge-based IMR for submillisievert cardiac CT .
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
Phantom Experiment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Patients
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CT Scanning and Contrast Infusion Protocols
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Scan Parameters of Low-Dose Cardiac CT
Scan Parameters Beam collimation (mm) 128 × 0.625 Slice thickness (mm) 0.8 Slice intervals (mm) 0.4 Tube voltage (kVp) 100 Tube current (mA) 303 Rotation time (s) 0.27 Effective mAs (mAs/slice) 110 CTDI vol (mGy) 5.2 DLP (mGy*cm) 68 Total amount of contrast medium (mgI/kg) 370 Injection duration (s) 15 Bolus tracking trigger (HU) 110 Scan mode Prospective ECG-triggered axial Scan delay (s) 9
CT, computed tomography; CTDI vol , CT volume dose index; DLP, dose length product; ECG, electrocardiographic; HU, Hounsfield unit.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CT Image Reconstruction
Get Radiology Tree app to read full this article<
Quantitative Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Qualitative Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Patients
Get Radiology Tree app to read full this article<
Table 2
Patient Characteristics and Patient Radiation Dose
Number of patients 43 Mean age (y) 70.6 ± 8.5 Male-to-female ratio 25:18 Mean weight (kg) 57.8 ± 7.4 Mean BMI (kg/m 2 ) 23.4 ± 1.9 EDs (mSv) 4.4 ± 0.4
BMI, body mass index; ED, effective doses.
Get Radiology Tree app to read full this article<
Phantom Experiment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Quantitative Image Analysis
Get Radiology Tree app to read full this article<
Table 3
Quantitative Image Analysis
FBP Hybrid IR Knowledge-Based IMR_P_ Value_P_ Value (Pairwise Comparisons) FBP vs Hybrid IR FBP vs Knowledge-Based IMR Hybrid IR vs Knowledge-Based IMR Mean attenuation (HU) 550.6 ± 59.2 550.6 ± 59.3 549.7 ± 59.0 .99 — — — Image noise (HU) 126.7 ± 35.0 48.8 ± 12.7 19.4 ± 3.3 <.01 <0.01 <0.01 <0.01 CNR 4.6 ± 1.3 12.1 ± 3.5 29.1 ± 5.4 <.01 <0.01 <0.01 <0.01
CNR, contrast noise ratio; FBP, filtered back projection; HU, Hounsfield unit; IMR, iterative model reconstruction; IR, iterative reconstruction.
Data are shown as the mean ± standard deviation.
Get Radiology Tree app to read full this article<
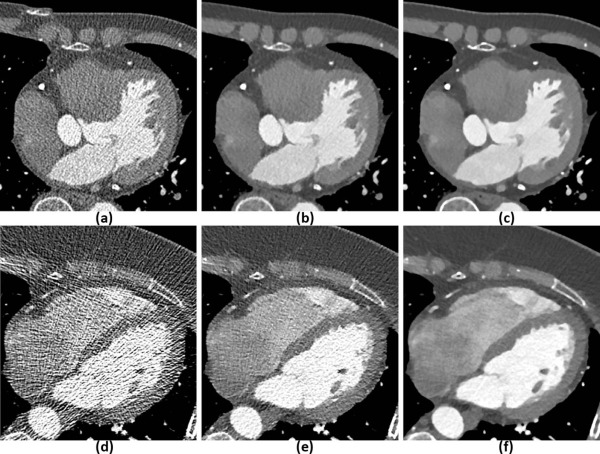
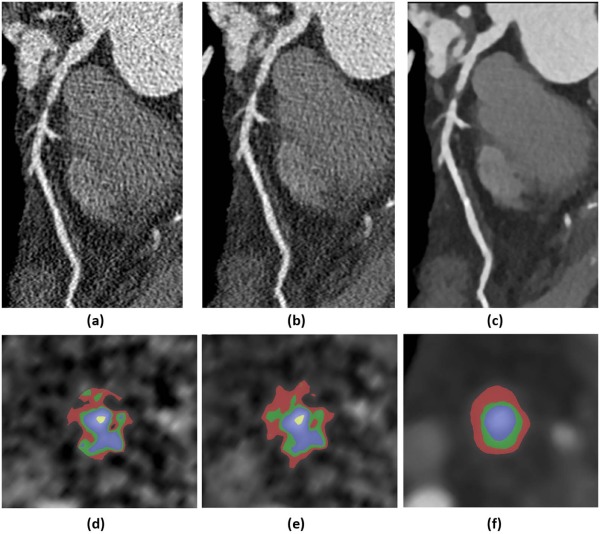
Qualitative Image Analysis
Get Radiology Tree app to read full this article<
Table 4
Results of Qualitative Image Analysis
FBP Hybrid IR Knowledge-Based IMR_P_ Value Kappa_P_ Value (Pairwise Comparisons) FBP vs Hybrid IR FBP vs Knowledge-Based IMR Hybrid IR vs Knowledge-Based IMR Image contrast 3.1 ± 1.0 3.5 ± 0.7 3.6 ± 0.6 .06 0.82 — — — Image noise 1.7 ± 0.6 2.8 ± 0.6 3.9 ± 0.2 <.01 0.76 <0.01 <0.01 <0.01 Image sharpness 1.9 ± 0.7 2.7 ± 0.7 3.8 ± 0.5 <.01 0.61 <0.01 <0.01 <0.01 Image texture 2.8 ± 0.4 2.2 ± 0.5 3.5 ± 0.5 <.01 0.62 <0.01 <0.01 <0.01 Overall image quality 2.0 ± 0.7 2.8 ± 0.5 3.9 ± 0.3 <.01 0.60 <0.01 <0.01 <0.01
FBP, filtered back projection; IMR, iterative model reconstruction; IR, iterative reconstruction.
Data are shown as the mean ± standard deviation.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Sodickson A., Baeyens P.F., Andriole K.P., et. al.: Recurrent CT, cumulative radiation exposure, and associated radiation-induced cancer risks from CT of adults. Radiology 2009; 251: pp. 175-184.
2. Berrington de Gonzalez A., Mahesh M., Kim K.P., et. al.: Projected cancer risks from computed tomographic scans performed in the United States in 2007. Arch Intern Med 2009; 169: pp. 2071-2077.
3. Brenner D.J., Hall E.J.: Computed tomography—an increasing source of radiation exposure. N Engl J Med 2007; 357: pp. 2277-2284.
4. Juergens K.U., Grude M., Fallenberg E.M., et. al.: Using ECG-gated multidetector CT to evaluate global left ventricular myocardial function in patients with coronary artery disease. AJR Am J Roentgenol 2002; 179: pp. 1545-1550.
5. Raff G.L., Gallagher M.J., O’Neill W.W., et. al.: Diagnostic accuracy of noninvasive coronary angiography using 64-slice spiral computed tomography. J Am Coll Cardiol 2005; 46: pp. 552-557.
6. Scheffel H., Alkadhi H., Plass A., et. al.: Accuracy of dual-source CT coronary angiography: first experience in a high pre-test probability population without heart rate control. Eur Radiol 2006; 16: pp. 2739-2747.
7. Hausleiter J., Meyer T., Hadamitzky M., et. al.: Radiation dose estimates from cardiac multislice computed tomography in daily practice: impact of different scanning protocols on effective dose estimates. Circulation 2006; 113: pp. 1305-1310.
8. Hausleiter J., Bischoff B., Hein F., et. al.: Feasibility of dual-source cardiac CT angiography with high-pitch scan protocols. J Cardiovasc Comput Tomogr 2009; 3: pp. 236-242.
9. Gagarina N.V., Irwan R., Gordina G., et. al.: Image quality in reduced-dose coronary CT angiography. Acad Radiol 2011; 18: pp. 984-990.
10. Silva A.C., Lawder H.J., Hara A., et. al.: Innovations in CT dose reduction strategy: application of the adaptive statistical iterative reconstruction algorithm. AJR Am J Roentgenol 2010; 194: pp. 191-199.
11. Heilbron B.G., Leipsic J.: Submillisievert coronary computed tomography angiography using adaptive statistical iterative reconstruction—a new reality. Can J Cardiol 2010; 26: pp. 35-36.
12. Nakaura T., Kidoh M., Sakaino N., et. al.: Low contrast- and low radiation dose protocol for cardiac CT of thin adults at 256-row CT: usefulness of low tube voltage scans and the hybrid iterative reconstruction algorithm. Int J Cardiovasc Imaging 2013; 29: pp. 913-923.
13. Block K.T., Uecker M., Frahm J.: Model-based iterative reconstruction for radial fast spin-echo MRI. IEEE Trans Med Imaging 2009; 28: pp. 1759-1769.
14. Deak Z., Grimm J.M., Treitl M., et. al.: Filtered back projection, adaptive statistical iterative reconstruction, and a model-based iterative reconstruction in abdominal CT: an experimental clinical study. Radiology 2013; 266: pp. 197-206.
15. Pickhardt P.J., Lubner M.G., Kim D.H., et. al.: Abdominal CT with model-based iterative reconstruction (MBIR): initial results of a prospective trial comparing ultralow-dose with standard-dose imaging. AJR Am J Roentgenol 2012; 199: pp. 1266-1274.
16. Katsura M., Matsuda I., Akahane M., et. al.: Model-based iterative reconstruction technique for radiation dose reduction in chest CT: comparison with the adaptive statistical iterative reconstruction technique. Eur Radiol 2012; 22: pp. 1613-1623.
17. Chang W., Lee J.M., Lee K., et. al.: Assessment of a model-based, iterative reconstruction algorithm (MBIR) regarding image quality and dose reduction in liver computed tomography. Invest Radiol 2013; 48: pp. 598-606.
18. Yuki H., Utsunomiya D., Funama Y., et. al.: Value of knowledge-based iterative model reconstruction in low-kV 256-slice coronary CT angiography. J Cardiovasc Comput Tomogr 2014; 8: pp. 115-123.
19. Halpern E.J., Gingold E.L., White H., et. al.: Evaluation of coronary artery image quality with knowledge-based iterative model reconstruction. Acad Radiol 2014; 21: pp. 805-811.
20. Menke J.: Comparison of different body size parameters for individual dose adaptation in body CT of adults. Radiology 2005; 236: pp. 565-571.
21. Imai E., Horio M., Nitta K., et. al.: Modification of the Modification of Diet in Renal Disease (MDRD) Study equation for Japan. Am J Kidney Dis 2007; 50: pp. 927-937.
22. Matsuo S., Imai E., Horio M., et. al.: Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis 2009; 53: pp. 982-992.
23. Hendel R.C., Patel M.R., Kramer C.M., et. al.: ACCF/ACR/SCCT/SCMR/ASNC/NASCI/SCAI/SIR 2006 appropriateness criteria for cardiac computed tomography and cardiac magnetic resonance imaging: a report of the American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group, American College of Radiology, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, American Society of Nuclear Cardiology, North American Society for Cardiac Imaging, Society for Cardiovascular Angiography and Interventions, and Society of Interventional Radiology. J Am Coll Cardiol 2006; 48: pp. 1475-1497.
24. Oda S., Utsunomiya D., Funama Y., et. al.: A low tube voltage technique reduces the radiation dose at retrospective ECG-gated cardiac computed tomography for anatomical and functional analyses. Acad Radiol 2011; 18: pp. 991-999.
25. Cademartiri F., Nieman K., van der Lugt A., et. al.: Intravenous contrast material administration at 16-detector row helical CT coronary angiography: test bolus versus bolus-tracking technique. Radiology 2004; 233: pp. 817-823.
26. Gervaise A., Osemont B., Lecocq S., et. al.: CT image quality improvement using Adaptive Iterative Dose Reduction with wide-volume acquisition on 320-detector CT. Eur Radiol 2012; 22: pp. 295-301.
27. Leipsic J., Labounty T.M., Heilbron B., et. al.: Adaptive statistical iterative reconstruction: assessment of image noise and image quality in coronary CT angiography. AJR Am J Roentgenol 2010; 195: pp. 649-654.
28. Hsieh J.: Computed tomography: principles, design, artifacts, and recent advances.second ed.2009.SPIE and Wileypp. 102.
29. Noel P.B., Fingerle A.A., Renger B., et. al.: Initial performance characterization of a clinical noise-suppressing reconstruction algorithm for MDCT. AJR Am J Roentgenol 2011; 197: pp. 1404-1409.
30. Hara A.K., Paden R.G., Silva A.C., et. al.: Iterative reconstruction technique for reducing body radiation dose at CT: feasibility study. AJR Am J Roentgenol 2009; 193: pp. 764-771.
31. Singh S., Kalra M.K., Hsieh J., et. al.: Abdominal CT: comparison of adaptive statistical iterative and filtered back projection reconstruction techniques. Radiology 2010; 257: pp. 373-383.
32. Brown K.M., Zabic S., Koehler T.: Acceleration of ML iterative algorithms for CT by the use of fast start images. Proc SPIE 2012; 8313: Physics of Medical Imaging
33. De Man B., Basu S.: Distance-driven projection and back projection in three dimensions. Phys Med Biol 2004; 49: pp. 2463-2475.
34. Yasaka K., Katsura M., Akahane M., et. al.: Model-based iterative reconstruction for reduction of radiation dose in abdominopelvic CT: comparison to adaptive statistical iterative reconstruction. Springerplus 2013; 2: pp. 209.
35. Hurwitz L.M., Yoshizumi T.T., Goodman P.C., et. al.: Effective dose determination using an anthropomorphic phantom and metal oxide semiconductor field effect transistor technology for clinical adult body multidetector array computed tomography protocols. J Comput Assist Tomogr 2007; 31: pp. 544-549.