
Rationale and Objectives
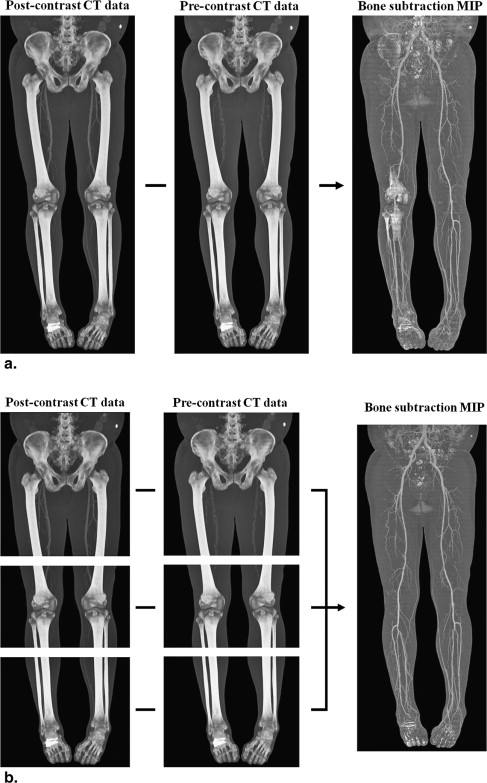
To validate the hypothesis that a multisegmented approach during subtraction computed tomography (CT) angiography of the lower extremities can improve bone removal efficiency by suppressing regional motion.
Materials and Methods
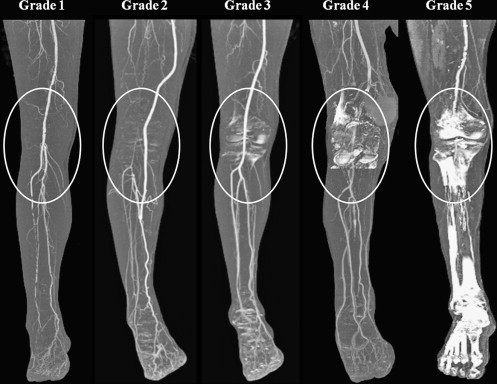
The institutional review board of our hospital approved this retrospective study. One hundred and one consecutive patients that had undergone the lower extremity CT angiography were included in this study. Subtraction CT angiography was performed using two different methods, namely, by single volume subtraction and by multisegmented volume subtraction. Multisegmented volume subtraction was conducted by dividing the whole volume of the CT data into three segments along the z axis of the lower extremities, performing a subtraction process for each segment, and combining segments to form as single subtracted volume. The bone removal efficiencies of the two methods was assessed by analyzing bone subtraction scores on maximum intensity projection (MIP) images for each bone segment in a blinded fashion. In addition, overall MIP image qualities were compared by displaying MIP images produced using the two methods side by side. Differences between bone subtraction scores were tested using Wilcoxon’s signed rank test.
Results
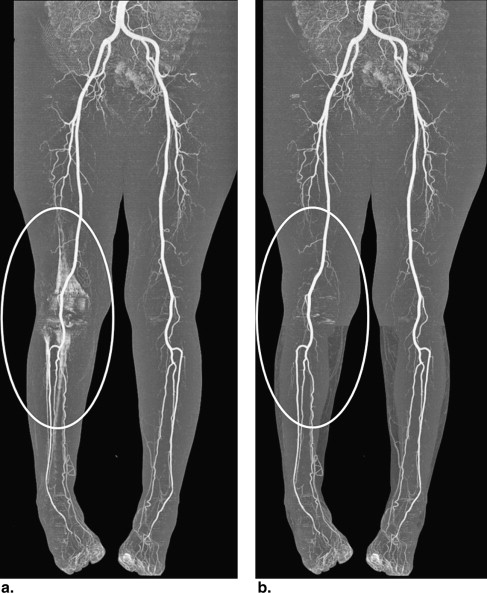
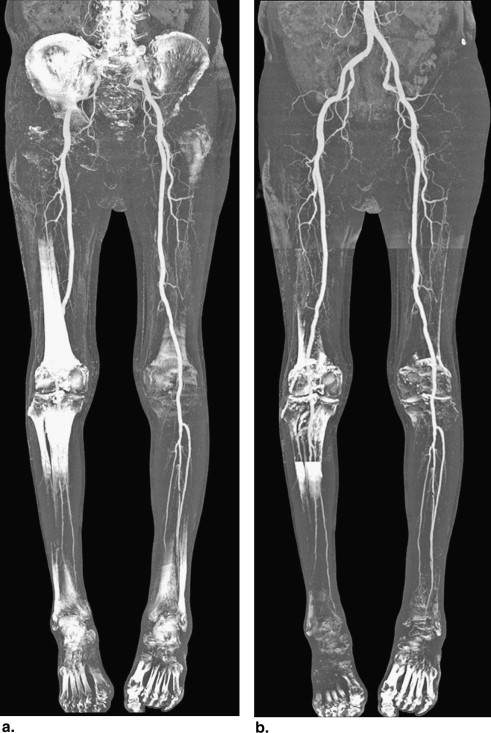
Multisegmented volume subtraction MIP images demonstrated significantly better bone removal for the following bone segments: pelvis ( P < .0001), hip ( P = .0002), thigh ( P = .0258), knee ( P = .0004), ankle ( P = .0008), metatarsal bone ( P < .0001), and toes ( P < .0001). Overall bone subtraction score and subjective image qualities determined by performing side-by-side comparisons were better for the multisegmented volume subtraction method.
Conclusion
Bone removal performance and overall MIP image quality can be increased by adopting multisegmented volume subtraction during subtraction CT angiography of the lower extremities.
Digital subtraction angiography (DSA) is currently the standard imaging reference method for the lower extremities in case of the peripheral arterial occlusive disease, because of its high temporal and spatial resolutions. However, DSA is also invasive, has a small risk of complications, and incurs high costs because of the need for hospitalization .
Technical advances in multidetector computed tomography (CT), which include improvements in spatial and temporal resolutions and scanning of the lower extremity arteries, mean that contrast-enhanced CT angiography is now considered noninvasive potential alternative to conventional DSA for evaluations of lower extremity arteries. Furthermore, several studies have demonstrated that CT angiography is comparable to conventional DSA in terms of performance and accuracy .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Patients
Get Radiology Tree app to read full this article<
CT Angiography
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Reconstruction and Post-processing
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Interpretation and Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Comparison of Bone Subtraction Score Between the Two Subtraction Methods at each Bone Segment
Segment Single Volume Subtraction Multisegmented Volume Subtraction_P_ Value ∗ Pelvis 1.97 ± 1.38 † 1.48 ± 1.02<.0001 Right hip 1.55 ± 1.05 1.27 ± 0.73.0023 Left hip 1.56 ± 1.04 1.34 ± 0.84.0062 Average of both hips 1.56 ± 0.96 1.30 ± 0.73.0002 Right thigh 1.32 ± 0.97 1.15 ± 0.50.0353 Left thigh 1.26 ± 0.90 1.17 ± 0.68 .2500 Average of both thighs 1.29 ± 0.90 1.16 ± 0.53.0258 Right knee 2.34 ± 1.27 1.98 ± 1.14.0021 Left knee 2.12 ± 1.15 1.94 ± 1.09 .0538 Average of both knees 2.23 ± 1.07 1.96 ± 1.02.0004 Right lower leg 1.39 ± 1.08 1.45 ± 1.13 .4143 Left lower leg 1.35 ± 1.03 1.28 ± 0.84 .4648 Average of both lower legs 1.37 ± 0.96 1.36 ± 0.89 .9843 Right ankle 2.59 ± 1.26 2.14 ± 1.17.0010 Left ankle 2.52 ± 1.13 2.34 ± 1.14 .0529 Average of both ankles 2.56 ± 1.04 2.24 ± 1.06.0008 Right metatarsal 2.70 ± 1.51 2.26 ± 1.30.0002 Left metatarsal 2.65 ± 1.32 2.23 ± 1.33.0003 Average of both metatarsals 2.68 ± 1.29 2.24 ± 1.22<.0001 Right toes 2.94 ± 1.41 2.59 ± 1.33.0021 Left toes 3.05 ± 1.31 2.69 ± 1.32.0017 Average of both toes 3.00 ± 1.21 2.64 ± 1.16<.0001 Total score of all segments(average score of all segments) 31.32 ± 13.38
(2.09 ± 0.89) 27.29 ± 11.71
(1.82 ± 0.78)<.0001
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Comparison of Overall Bone Subtraction Score Between the Two Subtraction Methods Depending on the Variable Distal Extent of coverage of Lower Extremity CT Angiography
Extent Reconstruction Method Maximum Score (n = 101)P Value ∗ 1 2 3 4 5 Pelvis-knee Single volume subtraction 13 † (12.9%) ‡ 39 (51.5%) 20 (71.3%) 14 (85.1%) 15 (100%) <.0001 Multisegmented volume subtraction 25 (24.8%) 45 (69.3%) 12 (81.2%) 11 (92.1%) 8 (100%) Pelvis-lower leg Single volume subtraction 13 (12.9%) 38 (50.5%) 20 (70.3%) 14 (84.2%) 16 (100%) <.0001 Multisegmented volume subtraction 24 (23.8%) 44 (67.3%) 13 (80.2%) 12 (92.1%) 8 (100%) Pelvis-ankle Single volume subtraction 4 (4.0%) 29 (32.7%) 26 (58.4%) 22 (80.2%) 20 (100%) <.0001 Multisegmented volume subtraction 8 (7.9%) 46 (53.5%) 18 (71.3%) 19 (90.1%) 10 (100%) Pelvis-toe(all segments) Single volume subtraction 2 (2.0%) 15 (16.8%) 27 (43.6%) 21 (64.4%) 36 (100%) <.0001 Multisegmented volume subtraction 2 (2.0%) 34 (35.6%) 23 (58.4%) 19 (77.2%) 23 (100%)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Side-by-side Comparison of Bone Subtraction Image Quality Between the Two Subtraction Methods in each Individual Patient
Single Volume Subtraction vs. Multisegmented Volume Subtraction Number (%) Single > multisegmented ∗ 1 (1.0 %) Single ≥ multisegmented † 4 (4.0 %) Single ≒ multisegmented ‡ 62 (61.4%) Single ≤ multisegmented § 16 (15.8%) Single < multisegmented ¶ 18 (17.8%) Total 101 (100%)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
References
1. Waugh J.R., Sacharias N.: Arteriographic complications in the DSA era. Radiology 1992; 182: pp. 243-246.
2. Schernthaner R., Stadler A., Lomoschitz F., et. al.: Multidetector CT angiography in the assessment of peripheral arterial occlusive disease: accuracy in detecting the severity, number, and length of stenoses. Eur Radiol 2008; 18: pp. 665-671.
3. Catalano C., Fraioli F., Laghi A., et. al.: Infrarenal aortic and lower-extremity arterial disease: diagnostic performance of multi-detector row CT angiography. Radiology 2004; 231: pp. 555-563.
4. Portugaller H.R., Schoellnast H., Hausegger K.A., et. al.: Multislice spiral CT angiography in peripheral arterial occlusive disease: a valuable tool in detecting significant arterial lumen narrowing?. Eur Radiol 2004; 14: pp. 1681-1687.
5. Willmann J.K., Baumert B., Schertler T., et. al.: Aortoiliac and lower extremity arteries assessed with 16-detector row CT angiography: prospective comparison with digital subtraction angiography. Radiology 2005; 236: pp. 1083-1093.
6. Heijenbrok-Kal M.H., Kock M.C., Hunink M.G.: Lower extremity arterial disease: multidetector CT angiography meta-analysis. Radiology 2007; 245: pp. 433-439.
7. Albrecht T., Foert E., Holtkamp R., et. al.: 16-MDCT angiography of aortoiliac and lower extremity arteries: comparison with digital subtraction angiography. AJR Am J Roentgenol 2007; 189: pp. 702-711.
8. Cernic S., Pozzi Mucelli F., Pellegrin A., et. al.: Comparison between 64-row CT angiography and digital subtraction angiography in the study of lower extremities: personal experience. Radiol Med 2009; 114: pp. 1115-1129.
9. Poletti P.A., Rosset A., Didier D., et. al.: Subtraction CT angiography of the lower limbs: a new technique for the evaluation of acute arterial occlusion. AJR Am J Roentgenol 2004; 183: pp. 1445-1448.
10. Kock M.C., Dijkshoorn M.L., Pattynama P.M., et. al.: Multi-detector row computed tomography angiography of peripheral arterial disease. Eur Radiol 2007; 17: pp. 3208-3222.
11. Raman R., Raman B., Napel S., et. al.: Improved speed of bone removal in computed tomographic angiography using automated targeted morphological separation: method and evaluation in computed tomographic angiography of lower extremity occlusive disease. J Comput Assist Tomogr 2008; 32: pp. 485-491.
12. Alpert N.M., Berdichevsky D., Levin Z., et. al.: Performance evaluation of an automated system for registration and postprocessing of CT scans. J Comput Assist Tomogr 2001; 25: pp. 747-752.
13. Lell M., Anders K., Klotz E., et. al.: Clinical evaluation of bone-subtraction CT angiography (BSCTA) in head and neck imaging. Eur Radiol 2006; 16: pp. 889-897.
14. Venema H.W., den Heeten G.J.: Subtraction helical CT angiography of intra- and extracranial vessels: technical considerations and preliminary experience—rediscovery of matched mask bone elimination?. AJNR Am J Neuroradiol 2003; 24: pp. 1491. author reply 1491–1492
15. Venema H.W., Hulsmans F.J., den Heeten G.J.: CT angiography of the circle of Willis and intracranial internal carotid arteries: maximum intensity projection with matched mask bone elimination-feasibility study. Radiology 2001; 218: pp. 893-898.
16. van Straten M., Venema H.W., Streekstra G.J., et. al.: Removal of bone in CT angiography of the cervical arteries by piecewise matched mask bone elimination. Med Phys 2004; 31: pp. 2924-2933.
17. Lell M.M., Anders K., Uder M., et. al.: New techniques in CT angiography. Radiographics 2006; 26: pp. S45-S62.
18. Hong H., Lee H., Shin Y.G.: Automatic vessel extraction by patient motion correction and bone removal in brain CT angiography. International Congress Series 2005; 1281: pp. 369-374.
19. Fiebich M., Straus C.M., Sehgal V., et. al.: Automatic bone segmentation technique for CT angiographic studies. J Comput Assist Tomogr 1999; 23: pp. 155-161.
20. Fishman E.K., Liang C.C., Kuszyk B.S., et. al.: Automated bone editing algorithm for CT angiography: preliminary results. AJR Am J Roentgenol 1996; 166: pp. 669-672.
21. Ogawa T., Okudera T., Noguchi K., et. al.: Cerebral aneurysms: evaluation with three-dimensional CT angiography. AJNR Am J Neuroradiol 1996; 17: pp. 447-454.
22. Meyer B.C., Werncke T., Hopfenmuller W., et. al.: Dual energy CT of peripheral arteries: effect of automatic bone and plaque removal on image quality and grading of stenoses. Eur J Radiol 2008; 68: pp. 414-422.
23. Sommer W.H., Johnson T.R., Becker C.R., et. al.: The value of dual-energy bone removal in maximum intensity projections of lower extremity computed tomography angiography. Invest Radiol 2009; 44: pp. 285-292.
24. Yamamoto S., McWilliams J., Arellano C., et. al.: Dual-energy CT angiography of pelvic and lower extremity arteries: dual-energy bone subtraction versus manual bone subtraction. Clin Radiol 2009; 64: pp. 1088-1096.