
Rationale and Objectives
Deriving maximum benefit from radiology rotations in medical schools is challenging. Lack of education on appropriate imaging renders students feeling unprepared. This study compares the ability of undergraduate medical students to identify appropriate radiological investigations, both at the beginning and end of their final year of education, to those of residents in their first year of clinical practice.
Materials and Methods
Twelve scenarios were extracted from the American College of Radiology’s Appropriateness Criteria (ACR-AC) and a questionnaire was generated. One topic was selected from each of the 10 sections in the diagnostic section and two from the interventional section. The questionnaire was distributed to three groups. Group A was composed of medical students at the beginning of final year. Group B was composed of medical students at the end of final year. Group C was composed of residents at the end of their first year of clinical practice. Radiology residents were surveyed to assess familiarity with the ACR-AC among trainees in Ireland.
Results
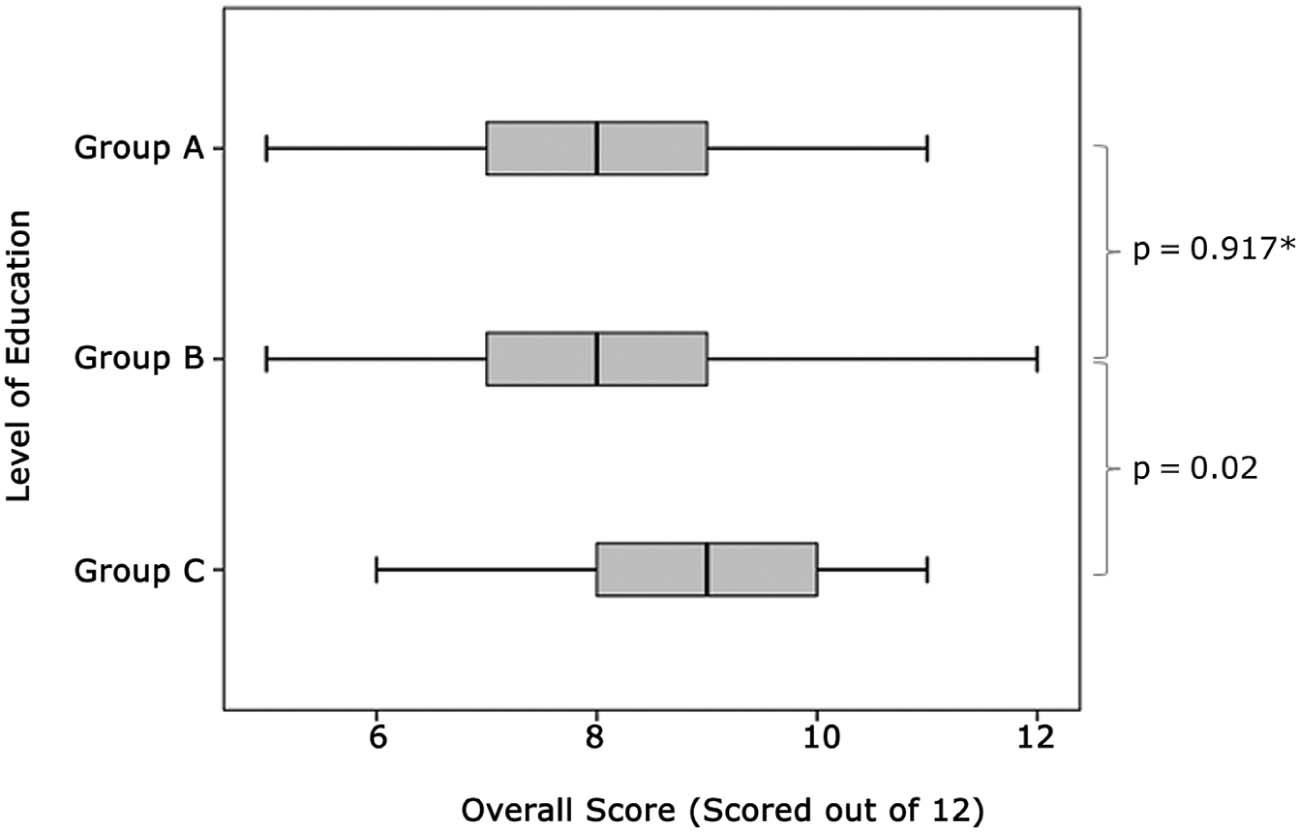
The total cohort included 160 participants. Group C ( n = 35) performed significantly better than group A ( n = 72) and group B ( n = 53). There was no statistical difference in the mean scores achieved by group A and group B. Sixteen (73%) of 22 radiology trainees were familiar with the ACR-AC.
Conclusions
A minimal improvement in the knowledge of medical students in requesting radiological investigations over the course of the final medical year, yet a significant impact of a relatively short period of “on-the-job” learning in the clinical setting, was indicated. Emphasis on education on appropriateness may offer an improvement in the utilization of radiology services and improve patient care.
Introduction
Radiological investigations are important diagnostic tools in the evaluation of patients. Although the interpretation and reporting of radiological investigations are a core clinical activity for radiologists, an awareness of the utility, limitations, and risks associated with different imaging modalities is important for all doctors. Recent technological advances in computed tomography (CT), ultrasonography, and magnetic resonance imaging have greatly increased the number of requests for these investigations by doctors . A combination of expeditious imaging processing and greater diagnostic information from the imaging modalities has rendered diagnostic imaging more attractive . The majority of specialties increasingly request medical imaging, and this has seen an upsurge in diagnostic imaging examinations performed in recent years .
With access to multiple imaging modalities becoming more commonplace, the reliance by healthcare providers on imaging has intensified significantly . Imaging services are estimated to have grown at twice the rate of other healthcare technologies over the last decade . Rise in the use of imaging in patient care means that, although imaging is being used to positively impact patient welfare in most circumstances, it is also being used inappropriately. The selection of the most appropriate radiological investigation is a combination of multiple competencies: the interpretation of the clinical presentation, due regard for available evidence and best practice, cost-effectiveness, limitations, and risk-benefit analysis. Deficiencies in the knowledge of the requesting doctor may contribute to inappropriate imaging, leading to subsequent image overutilization . Furthermore, inappropriate scanning may lead to identification of incidental findings unrelated to the patient’s clinical presentation, may expose the patient to unnecessary risk, or may falsely reassure the patient or the clinician. Educational efforts by medical organizations have attempted to address this, and the need for improvement has been reiterated for a number of years .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
Questionnaire Design and Administration
Get Radiology Tree app to read full this article<
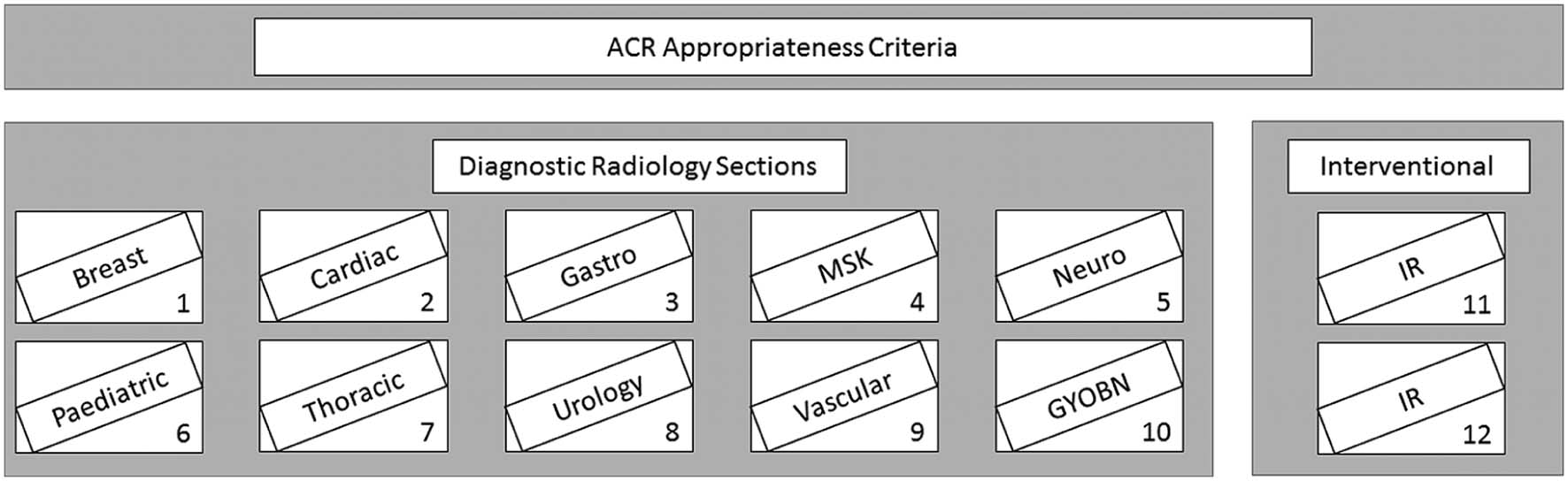
TABLE 1
The 12 Multiple Choice Questions Detailed in the Questionnaire with the Correct Answer Highlighted and Underlined
Question Answer Choice (correct answer is underlined) 1 Breast
What is the initial evaluation for a woman, forty years of age with a palpable breast lump? Image-guided fine needle aspiration
Image-guided core biopsy
Diagnostic mammography
US breast
MRI breast 2 Cardiovascular
Which investigation, if any, should be used to assess the risk of coronary artery disease in an asymptomatic patient?No imaging required
Transthoracic echocardiography
X-ray chest
Transesophageal echocardiography
CTA coronary arteries with contrast 3 General surgery
Identify the most appropriate imaging for a typical abdominal pain, with increased amylase and lipase in a patient presenting for the first time. CT abdomen without contrast
MRI abdomen
Chest x-ray
US abdomen
Abdominal x-ray 4 Orthopedic
What is the most appropriate imaging investigation for an adult who has turned heavily on his ankle, is unable to bear weight immediately after the injury, and has point tenderness over the medial malleolus? No imaging required
X-ray ankle (AP, lateral and mortise)
CT ankle without contrast
MRI ankle
US ankle 5 Neurology
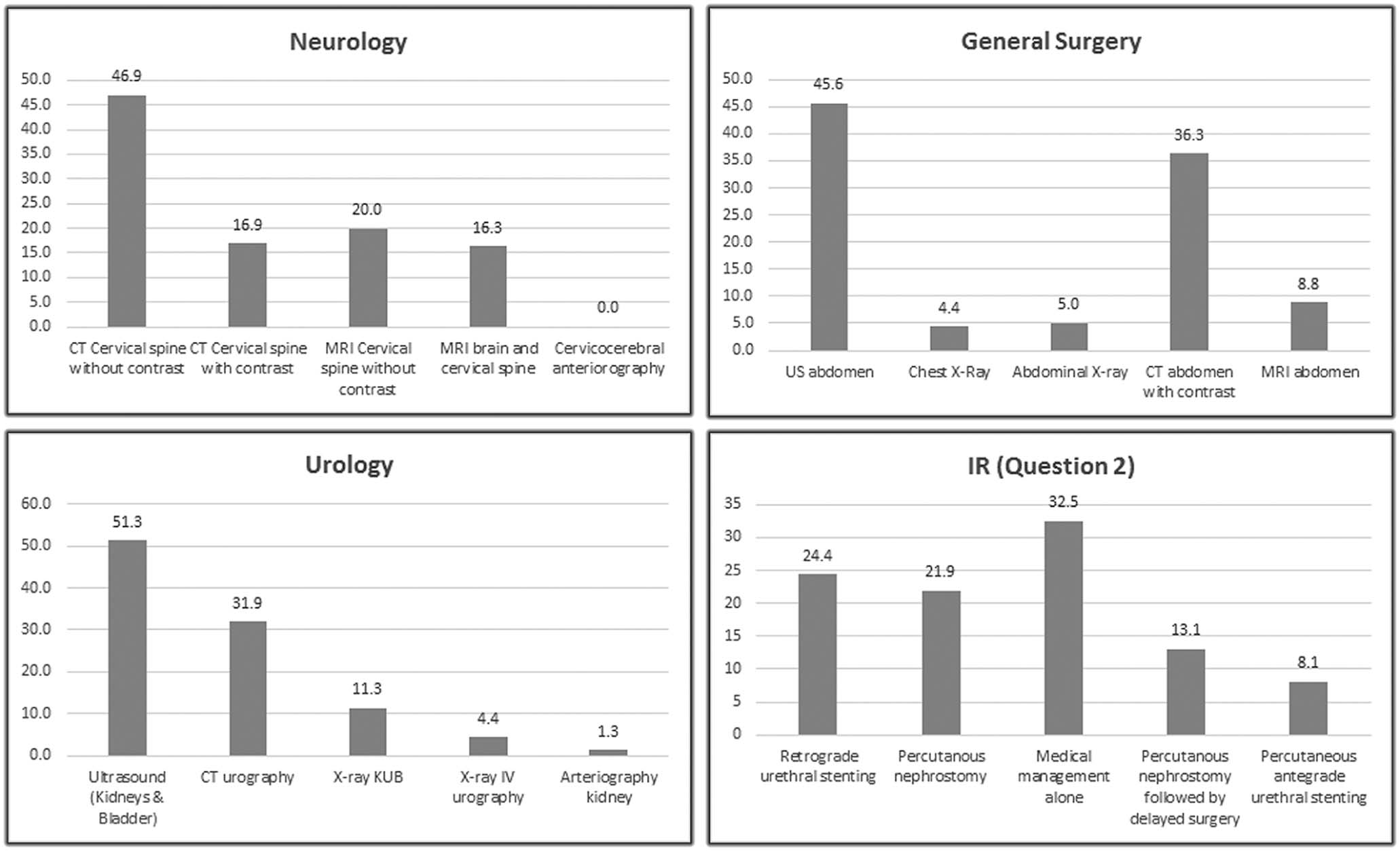
First line imaging for a suspected acute cervical spine trauma. Imaging indicated by clinical criteria (NEXUS or CCR). No myelopathy or neuropathy specified.CT cervical spine without contrast
CT cervical spine with contrast
MRI cervical spine without contrast
MRI brain and cervical spine
Cervicocerebral arteriography 6 Pediatric
Identify appropriate imaging, if any, for a moderate or severe head injury (GCS ≤13) or minor head trauma with high-risk factors (eg, altered mental status, clinical evidence of basilar skull fracture) in an 11-year-old child. X-ray head
Arteriography cerebral
MRI head without contrast
Imaging not appropriate
CT head without contrast 7 Respiratory
What is the most appropriate initial imaging investigation for a 40 year-old-patient with recurrent hemoptysis (>30 pack-year history)? Pulmonary arteriography
CT Pulmonary angiogram
X-ray chest
Bronchial arteriography
No imaging required 8 Urology
What is the most appropriate imaging for patients with painless frank hematuria with a normal cystoscopy? X-ray intravenous urography
CT urography
US kidneys and bladder
Arteriography kidney
X-ray abdomen and pelvis (KUB) 9 Vascular
What is the most appropriate initial imaging for a suspected case of acute mesenteric ischemia? Arteriography of the abdomen
X-ray abdomen
US abdomen
CTA abdomen with contrast
MRI abdomen without contrast 10 Gynecology
What is the most appropriate initial imaging for a clinically suspected adnexal mass in a girl of reproductive age?US pelvis transvaginal
CT pelvis with contrast
MRI pelvis without contrast
CT pelvis without contrast
FDG-PET/CT whole body 11 Interventional
What is the most appropriate procedure for an elderly patient with a history of abdominal pain after meals for the past few months and weight loss? CT scan of the abdomen shows aortic atherosclerotic disease and suggests SMA origin stenosis with occlusion of celiac origin and an occluded inferior mesenteric artery (IMA). Surgical bypass or endarterectomy
Systemic anticoagulation
Supportive measures only
MRI abdomen without contrast
Angiography with possible angioplasty 12 Interventional
What is the most appropriate management for an adult patient with a 7-day history of right flank pain, fever, and leukocytosis? Urinalysis is positive for blood. CT scan shows a 10 mm stone in the right ureter without hydronephrosis. Medical management
Retrograde ureteral stenting
Percutaneous nephrostomy
Antegrade ureteral stenting
Nephrostomy and delayed surgery
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Assessing Awareness of ACR-AC
Get Radiology Tree app to read full this article<
Statistical Analyses
Get Radiology Tree app to read full this article<
Results
Participants
Get Radiology Tree app to read full this article<
TABLE 2
Details of the Performance of Group A (Students Entering Their Final Year of Medical School), Group B (Students at the End of Their Final Year of Medical Education), and Group C (Residents Who Have Just Completed 1 Year of Clinical Practice)
Correct Answer, n (%) Question Topic Group A, n = 72 Group B, n = 53 Group C, n = 35 Breast 53(74) 33(62) 34(97) Cardiovascular 58(81) 43(82) 29(83) General surgery 36(50) 24(45) 17(49) Orthopedic 69(96) 53(100) 34(97.1) Neurology 27(38) 28(53) 17(49) Pediatrics 66(93) 49(93) 34(97) Respiratory 66(92) 47(89) 29(83) Urology 21(29) 16(30) 17(49) Vascular 45(63) 32(60) 32(91) Gynecology 62(86) 47(89) 29(83) IR 51(71) 39(74) 27(77) IR 10(14) 10(19) 22(66) Mean score(%) 80.3 ± 15.6 80.6 ± 14.9 90.9 ± 15
IR, interventional radiology.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Limitations of the Study
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
References
1. Bhargavan M., Sunshine J.H.: Utilization of radiology services in the United States: levels and trends in modalities, regions, and populations. Radiology 2005; 234: pp. 824-832.
2. Bautista A.B., Burgos A., Nickel B.J., et. al.: Do clinicians use the American College of Radiology Appropriateness Criteria in the management of their patients?. AJR Am J Roentgenol 2009; 192: pp. 1581-1585.
3. Kondo K.L., Swerdlow M.: Medical student radiology curriculum: what skills do residency program directors believe are essential for medical students to attain?. Acad Radiol 2013; 20: pp. 263-271.
4. Gunderman R.B., Siddiqui A.R., Heitkamp D.E., et. al.: The vital role of radiology in the medical school curriculum. AJR Am J Roentgenol 2003; 180: pp. 1239-1242.
5. Chan S.: The importance of strategy for the evolving field of radiology. Radiology 2002; 224: pp. 639-648.
6. Maitino A.J., Levin D.C., Parker L., et. al.: Practice patterns of radiologists and nonradiologists in utilization of noninvasive diagnostic imaging among the Medicare population 1993–1999. Radiology 2003; 228: pp. 795-801.
7. Hendee W.R., Becker G.J., Borgstede J.P., et. al.: Addressing overutilization in medical imaging. Radiology 2010; 257: pp. 240-245.
8. Ip I.K., Schneider L.I., Hanson R., et. al.: Adoption and meaningful use of computerized physician order entry with an integrated clinical decision support system for radiology: ten-year analysis in an urban teaching hospital. J Am Coll Radiol 2012; 9: pp. 129-136.
9. Dillon J.E., Slanetz P.J.: Teaching evidence-based imaging in the radiology clerkship using the ACR appropriateness criteria. Acad Radiol 2010; 17: pp. 912-916.
10. Prezzia C., Vorona G., Greenspan R.: Fourth-year medical student opinions and basic knowledge regarding the field of radiology. Acad Radiol 2013; 20: pp. 272-283.
11. Kourdioukova E.V., Valcke M., Derese A., et. al.: Analysis of radiology education in undergraduate medical doctors training in Europe. Eur J Radiol 2011; 78: pp. 309-318.
12. Pascual T.N., Chhem R., Wang S.C., et. al.: Undergraduate radiology education in the era of dynamism in medical curriculum: an educational perspective. Eur J Radiol 2011; 78: pp. 319-325.
13. General Medical Council. : Tomorrow’s doctors—outcomes and standards for undergraduate medical education. Available at: http://www.gmc-uk.org/ Accessed June 14, 2016
14. The Royal College of Radiologists. : Undergraduate radiology curriculum. Available at: https://www.rcr.ac.uk/sites/default/files/Undergraduate_Radiology_Curriculum_2012.pdf Accessed June 14, 2016
15. Lee J.S., Aldrich J.E., Eftekhari A., et. al.: Implementation of a new undergraduate radiology curriculum: experience at the University of British Columbia. Can Assoc Radiol J 2007; 58: pp. 272-278.
16. Naeger D.M., Phelps A., Kohi M., et. al.: Reading room electives: say goodbye to the “radi-holiday”. J Am Coll Radiol 2013; 10: pp. 442-448.
17. Deitte L.A., Gordon L.L., Zimmerman R.D., et. al.: Entrustable professional activities: ten things Radiologists do. Acad Radiol 2016; 23: pp. 374-381.
18. Saha A., Roland R.A., Hartman M.S., et. al.: Radiology medical student education: an outcome-based survey of PGY-1 residents. Acad Radiol 2013; 20: pp. 284-289.
19. Subramaniam R., Hall T., Chou T., et. al.: Radiology knowledge in new medical graduates in New Zealand. N Z Med J 2005; 118: pp. U1699.
20. O’Connor P., Lydon S., Offiah G., et. al.: Impact of working 48 h per week on opportunities for training and patient contact: the experience of Irish interns. Int J Qual Health Care 2015; 27: pp. 492-498.
21. Council I.M.: Your training counts—trainee experiences of clinical learning environments in Ireland 2015.M. Council National trainee survey.2015.medicalcouncil.ieDublin 2, Ireland:pp. 48.
22. Bosanquet D., Cho J., Williams N., et. al.: Requesting radiological investigations—do junior doctors know their patients? A cross-sectional survey. JRSM Short Rep 2013; 4: pp. 3.
23. Murphy K.P., Crush L., O’Malley E., et. al.: Medical student knowledge regarding radiology before and after a radiological anatomy module: implications for vertical integration and self-directed learning. Insights Imaging 2014; 5: pp. 629-634.
24. Leong S., Keeling A.N., Lee M.J.: A survey of interventional radiology awareness among final-year medical students in a European country. Cardiovasc Intervent Radiol 2009; 32: pp. 623-629.
25. Nyhsen C.M., Lawson C., Higginson J.: Radiology teaching for junior doctors: their expectations, preferences and suggestions for improvement. Insights Imaging 2011; 2: pp. 261-266.
26. Nyhsen C.M., Steinberg L.J., O’Connell J.E.: Undergraduate radiology teaching from the student’s perspective. Insights Imaging 2013; 4: pp. 103-109.
27. IMC : “Your Training Counts”. Available at: http://www.medicalcouncil.ie/News-and-Publications/Reports/Your-Training-Counts-Survey.pdf Accessed May 28, 2016
28. Boggis C., Cook P., Denison A., et. al.: The place of clinical radiology and imaging in medical education: objectives, content and delivery of teaching.2007.The Royal College of Radiologists UKLondon May
29. McInerney N.M., Larkin J.O., O’Callaghan A.P., et. al.: Changes in medical student’s perspective on priorities in undergraduate education and training following completion of internship. Int J Innov Res Educ Sci 2014; 2: pp. 54-59.
30. Kozak B., Webb E.M., Khan B.K., et. al.: Medical student usage of the American College of Radiology Appropriateness Criteria. Acad Radiol 2015; 22: pp. 1606-1611.
31. Sheng A.Y., Castro A., Lewiss R.E.: Awareness, utilization, and education of the ACR appropriateness criteria: a review and future directions. J Am Coll Radiol 2016; 13: pp. 131-136.
32. Powell D.K., Silberzweig J.E.: The use of ACR appropriateness criteria: a survey of radiology residents and program directors. Clin Imaging 2015; 39: pp. 334-338.
33. American College of Radiology : A. Topic development process. Available at: http://www.acr.org/~/media/ACR/Documents/AppCriteria/Overview.pdf Accessed June 26, 2016
34. Van Der Molen A.J., Cowan N.C., Mueller-Lisse U.G., et. al.: CT urography: definition, indications and techniques. A guideline for clinical practice. Eur Radiol 2008; 18: pp. 4-17.