
Rationale and Objectives
Patients with tetralogy of Fallot have right ventricular outflow and pulmonary valve stenosis. They may also have more distal peripheral pulmonary artery stenoses. Peripheral stenosis is believed to be part of the spectrum of the genetic manifestation of tetralogy. Our hypothesis was that narrowing of the right pulmonary artery may be due to compression from the adjacent dilated ascending aorta.
Materials and Methods
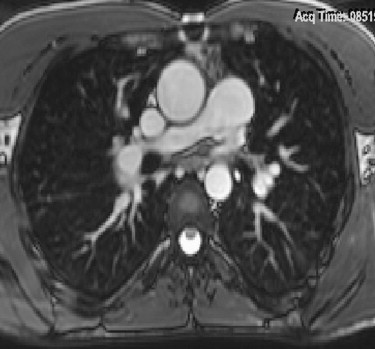
We identified 27 patients with tetralogy of Fallot who underwent magnetic resonance imaging scanning postoperatively, most often for evaluation of pulmonary valve stenosis and regurgitation. On the axial image at the level of the right pulmonary artery, we measured the transverse diameters of the ascending and descending aorta, and the minimum and maximum right pulmonary artery diameters.
Results
There was a significant correlation between the ratios of the ascending:descending aorta diameters and the maximum:minimum right pulmonary artery diameters. Thus, increasing ascending aorta size is associated with decreasing size of the adjacent right pulmonary artery.
Conclusions
In our patient population with tetralogy of Fallot, right pulmonary artery narrowing is at least partly because of compression from the adjacent enlarged ascending aorta.
Patients with tetralogy of Fallot have the classical findings of ventricular septal defect, aortic override of the ventricular septum, pulmonary outflow stenosis, and right ventricular hypertrophy. Tetralogy results from malposition of the truncal septum as it divides the truncus arteriosus into the pulmonary artery and the ascending aorta. Instead of lying in the middle of the truncus, the septum comes to lie over to one side. This results in a narrow pulmonary artery and a large ascending aorta. Patients with tetralogy may have many other associated cardiovascular anomalies, including focal peripheral pulmonary artery stenoses . These pulmonary artery stenoses have also been believed to be part of the genetic syndrome . However, it is possible that at least one type of pulmonary arterial stenosis often found in patients with tetralogy is not genetic in origin. This is focal, mild to moderate narrowing of the proximal right pulmonary artery (RPA). Our hypothesis is that this narrowing is not genetic in origin, but secondary to compression from a dilated ascending aorta lying immediately anterior to the right pulmonary artery. Our study was designed to see if there was a correlation between the amount of the ascending aortic dilatation and the amount of narrowing of the adjacent right pulmonary artery.
Methods and materials
We identified 27 consecutive patients with tetralogy of Fallot who underwent magnetic resonance imaging scanning at our facility between January 2004 and December 2005. All patients were scanned on a Siemens Avanto machine (Siemens, Erlangen, Germany), using a truefisp sequence and breath hold. The age range was 3.5–43 years. All patients had been referred for postoperative evaluation of pulmonary valve stenosis and regurgitation, or right ventricle function. Some patients had received right ventricle-pulmonary artery conduits. No patient had prior surgery/intervention to either pulmonary artery. No patient had an absent pulmonary valve. This study was approved by our institutional review board, with waiver of informed consent.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Measurements of the Diameters of the Aorta and the Right Pulmonary Artery (RPA)
Patient age (years) Ascending aorta diameter (mm) Descending aorta diameter (mm) Minimum RPA diameter (behind the asc. aorta) (mm) Maximum RPA diameter (anywhere along its length) (mm) 18 32.6 14.6 4.0 6.4 17 32.7 15.6 11.2 16.5 18 30.6 17.5 17.0 18.7 43 32.3 17.3 23.2 23.9 14 24.4 12.0 9.4 10.1 15 22.4 14.6 10.8 13.3 24 30.1 13.1 2.3 8.5 32 32.4 20.4 21.7 24.7 22 27.7 14.5 13.1 15.8 14 40.7 17.2 5.3 10.0 19 27.6 13.7 13.4 14.2 3.5 16.7 10.0 4.2 9.7 18 30.7 16.3 8.2 10.2 35 37.8 15.6 11.9 20.4 12 27.4 14.8 11.0 13.9 10 28.1 13.9 8.6 10.3 3.5 14.0 8.3 6.8 9.6 15 28.7 15.5 11.3 14.6 8 19.2 12.5 10.1 10.1 29 29.5 14.1 14.4 18.2 15 20.6 10.5 7.0 10.8 37 30.4 15.0 9.9 19.4 15 24.0 14.6 9.4 12.0 16 35.1 17.7 11.8 14.4 25 33.5 21.0 8.4 14.8 27 26.4 15.9 12.0 13.2 15 32.1 15.1 11.3 14.1
Table 2
Descriptive Statistics of Ratios
1 2 Mean 1.91 1.46 SD 0.25 0.55 Median 1.91 1.26 Range 1.53 to 2.42 1.00 to 3.70
1 = ascending aorta diameter/descending aorta diameter; 2 = right pulmonary artery maximum diameter/minimum diameter; SD = standard deviation.
All comparisons are Pearson’s correlation, with coefficient R and P values: Comparison: 1 vs. 2; R = 0.3902; P = .0442.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Variation in Size of Diameters of Aorta and Right Pulmonary Artery (RPA)
The % decrease from max RPA diameter to minimal RPA diameter Mean decrease in RPA 25.4% SD 17.7 Median 20.9% Range 0 to 72.9% Mean decrease in size of the aorta from the ascending to the descending aorta measured at the level of the RPA Mean decrease in aorta 46.9% SD 7.0 Median 47.7% Range 34.8 to 58.7%
SD, standard deviation.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Beekman R.P., Beek F.J., Meijboom E.J.: Usefulness of MRI for the pre-operative evaluation of the pulmonary arteries in tetralogy of Fallot. Magn Reson Imaging 1997; 15: pp. 1005-1015.
2. Bostan Ö.M., Çil E.: Case of tetralogy of Fallot associated with hypoplasia of the right pulmonary artery. Int J Cardiovasc Imaging 2005; 21: pp. 369-371.
3. Sharma S.N., Sharma S., Shrivastava S., et. al.: Pulmonary arterial anatomy in tetralogy of Fallot. Int J Cardiol 1989; 25: pp. 33-37.
4. Fellows K.E., Smith J., Keane J.F.: Preoperative angiocardiography in infants with tetrad of Fallot. Review of 36 cases. Am J Cardiol 1981; 47: pp. 1279-1285.
5. Boechat M.I., Ratib O., Williams P.L., et. al.: Cardiac MR imaging and MR angiography for assessment of complex tetralogy of Fallot and pulmonary atresia. RadioGraphics 2005; 25: pp. 1535-1546.
6. Holmqvist C., Hochbergs P., Bjorkhem G., et. al.: Pre-operative evaluation with MR in tetralogy of Fallot and pulmonary atresia with ventricular septal defect. Acta Radiol 2001; 42: pp. 63-69.
7. Shinebourne E.A., Anderson R.H.: Fallot’s tetralogy.Anderson R.H.Baker E.J.Pediatric cardiology.2002.Churchill LivingstoneNew York:pp. 1213-1220.