
Rationale and Objectives
18-Fluoro-2-deoxyglucose (18F-FDG) positron emission tomography (PET) is effective but costly in the early detection of recurrence for nasopharyngeal carcinoma (NPC) in patients after treatment. In this study, we developed a decision tree model to analyze the cost utility of 18F-FDG PET in detecting loco-regional recurrences for NPC patients after therapy.
Materials and Methods
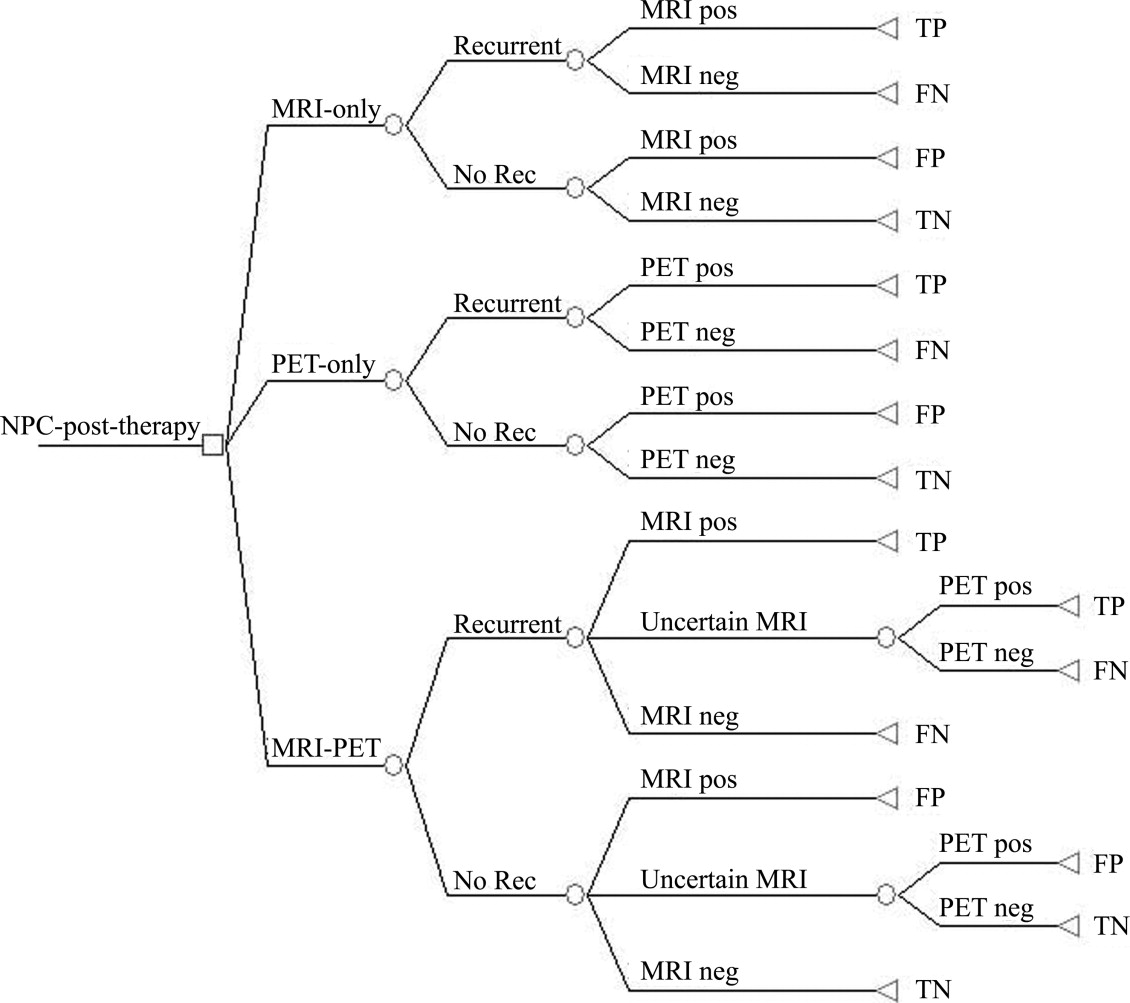
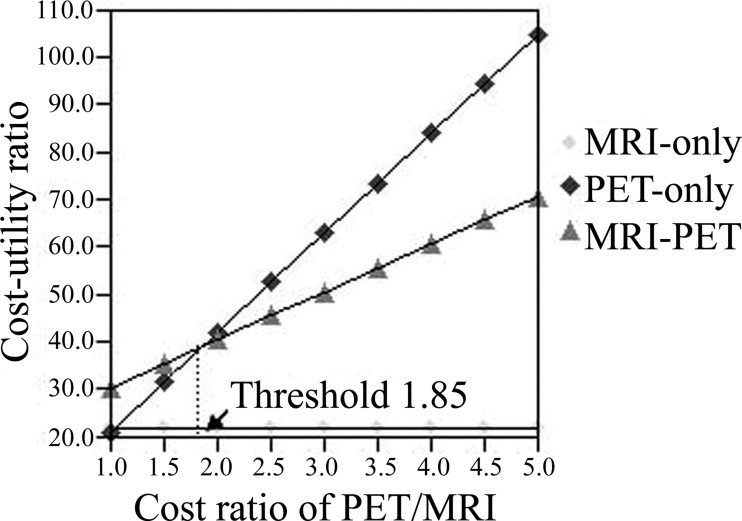
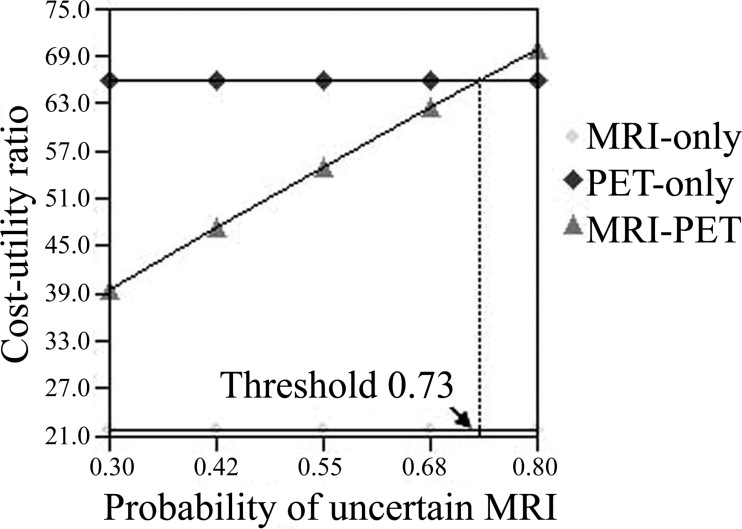
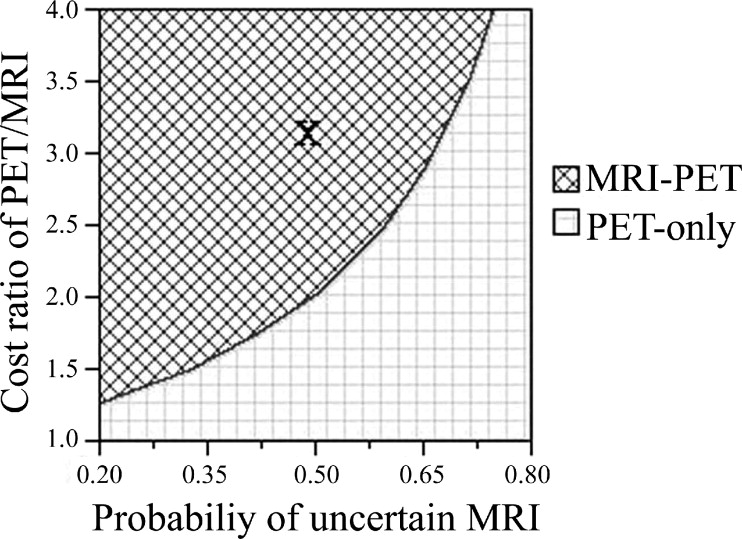
The analysis for cost utility is based on the decision-tree model for three different strategies: 1) magnetic resonance imaging (MRI)-only, 2) PET-only, and 3) MRI-PET (performing PET if MRI result is uncertain). Sensitivity analyses have been performed to examine changes in the cost ratio of PET/MRI and the probability of uncertain MRI.
Results
After inputting the data for utilities and life expectancies into the decision tree model, the quality-adjusted life expectancies turn out to be 16.16 quality-adjusted life-years (QALYs) for strategy 1, 16.70 QALYs for strategy 2, and 17.35 QALYs for strategy 3. The additional cost per additional QALYs for strategy 3 relative to strategy 1 is calculated to be US $462. Strategy 3 dominates over strategy 2 because strategy 3 costs less and yields more QALYs than strategy 2. If the cost ratio of PET/MRI is less than 1.85 or the probability of uncertain MRI is greater than 73%, then the PET-only strategy becomes more cost-effective than the MRI-PET strategy.
Conclusion
Our analysis shows that the MRI-PET strategy is the most cost-effective for now. It is likely the PET-only strategy will become the most cost-effective for recurrent NPC in patients in the near future as the cost of PET has decreased in a faster rate than the cost of MRI.
In Southern China and Southeast Asia, nasopharyngeal carcinoma (NPC) is one of the more common malignant tumors ( ), with an incidence rate of 10–30 persons per 100,000 people per year. The loco-regional recurrence is one of the crucial prognostic factors for NPC patients who have undergone radiotherapy (RT) or RT with adjuvant chemotherapy ( ). The conventional structure based diagnostic tools, such as magnetic resonance imaging (MRI) and computed tomography (CT), have been proved ineffective in the early detection of residual or recurrent foci for NPC patients ( ).
In contrast, it has been demonstrated in previous studies that 18-fluoro-2-deoxyglucose (18F-FDG) positron emission tomography (PET) is an effective tool for distinguishing recurrent tumors from post-treatment changes, such as tissue necrosis or fibrosis in the nasopharynx ( ). However, 18F-FDG PET scan is not routinely scheduled for the follow-up of NPC patients in our center due to its prohibitive cost. It is performed only when suspicious recurrences have been revealed in the results of other conventional radiologic findings during follow-up.
Get Radiology Tree app to read full this article<
Materials and methods
Decision Analysis Model
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
The Baseline Case
Get Radiology Tree app to read full this article<
Probabilities
Get Radiology Tree app to read full this article<
Table 1
Probabilities Used in the Decision Tree
Variables Value (%) Range Reference For MRI-only MRI Sensitivity 60 50–70 MRI Specificity 60 50–70 For PET-only PET Sensitivity (low pretest probability) 70 60–80 PET Specificity (low pretest probability) 70 60–80 For MRI-PET Probability of an indeterminate MRI 50 20–80 MRI Sensitivity 75 65–85 MRI Specificity 75 65–85 PET Sensitivity (high pretest probability) 90 75–95 PET Specificity (high pretest probability) 90 75–95
MRI, magnetic resonance imaging; PET, positron emission tomography.
Get Radiology Tree app to read full this article<
Outcome Measures
Utility
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Utilities Estimated from Visual Analog Scale
Status Utility Standard Deviation Post-initial treatment disease free 0.76 0.14 During treatment for recurrence 0.35 0.15 Recurrence after treatment 0.57 0.18 Recurrence delayed treatment 0.32 0.11
Get Radiology Tree app to read full this article<
Life expectancy
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Life Expectancies for NPC Patients After Initial Chemoradiation without Recurrence, Recurrence with Immediate Treatment, and Recurrence but Delayed Treatment
Status 5-y Disease-specific Mortality Life Expectancy Reference Recurrence free 0% 32 Recurrence with immediate treatment 50% 7.7 Recurrence but delayed treatment 80% 3.5
Get Radiology Tree app to read full this article<
Costs
Get Radiology Tree app to read full this article<
Table 4
Costs of Magnetic Resonance Imaging (MRI) and Positron Emission Tomographic (PET) Scans
Study Cost (US$) MRI scan 350 PET scan 1,100
Get Radiology Tree app to read full this article<
Diagnostic accuracy
Get Radiology Tree app to read full this article<
Cost-utility analysis
Get Radiology Tree app to read full this article<
ICUR=[cost(strategyX)−cost(strategyY)]/[utility(strategyX)−utility(strategyY)]. ICUR
=
[
cost
(
strategy
X
)
−
cost
(
strategy
Y
)
]
/
[
utility
(
strategy
X
)
−
utility
(
strategy
Y
)
]
.
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 5
Baseline Results from Cost-utility Analysis
Strategy Cost ($) Diagnostic Accuracy QALY Incremental Cost Per QALY ($) MRI-only 350 0.60 16.16 — PET-only 1100 0.70 16.70 1389 MRI-PET only 900 0.82 17.35 462
MRI, magnetic resonance imaging; PET, positron emission tomography; QALY, quality-adjusted life years.
Get Radiology Tree app to read full this article<
Diagnostic Accuracy
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
QALYs
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Sensitivity Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Acknowledgment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Huang D.P.: Epidemiology of nasopharyngeal carcinoma. Ear Nose Throat J 1990; 69: pp. 222-225.
2. Liu M.T., Hsieh C.Y., Chang T.H., Lin J.P., Huang C.C., Wang A.Y.: Prognostic factors affecting the outcome of nasopharyngeal carcinoma. Jpn J Clin Oncol 2003; 33: pp. 501-508.
3. Farias T.P., Dias F.L., Lima R.A., et. al.: Prognostic factors and outcome for nasopharyngeal carcinoma. Arch Otolaryngol Head Neck Surg 2003; 129: pp. 794-799.
4. Chong V.F., Fan Y.F.: Detection of recurrent nasopharyngeal carcinoma: MR imaging versus CT. Radiology 1997; 202: pp. 463-470.
5. Ng S.H., Chang J.T., Ko S.F., Wan Y.L., Tang L.M., Chen W.C.: MRI in recurrent nasopharyngeal carcinoma. Neuroradiology 1999; 41: pp. 855-862.
6. Olmi P., Fallai C., Colagrande S., Giannardi G.: Staging and follow-up of nasopharyngeal carcinoma: magnetic resonance imaging versus computerized tomography. Int J Radiat Oncol Biol Phys 1995; 32: pp. 795-800.
7. Kao C.H., ChangLai S.P., Chieng P.U., Yen R.F., Yen T.C.: Detection of recurrent or persistent nasopharyngeal carcinomas after radiotherapy with 18-fluoro-2-deoxyglucose positron emission tomography and comparison with computed tomography. J Clin Oncol 1998; 16: pp. 3550-3555.
8. Kao C.H., Shiau Y.C., Shen Y.Y., Yen R.F.: Detection of recurrent or persistent nasopharyngeal carcinomas after radiotherapy with technetium-99m methoxyisobutylisonitrile single photon emission computed tompgraphy and conputed tomography. Cancer 2002; 94: pp. 1981-1986.
9. Yen R.F., Hung R.L., Pan M.H., Wang Y.H., Huang K.M., Lui L.T., et. al.: 18-fluoro-2-deoxyglucose positron emission tomography in detecting residual/recurrent nasopharyngeal carcinomas and comparison with magnetic resonance imaging. Cancer 2003; 98: pp. 283-287.
10. Ng S.H., Chang T.C., Chan S.C.: Clinical usefulness of 18F-FDG PET in nasopharyngeal carcinoma patients with questionable MRI findings for recurrence. J Nucl Med 2004; 45: pp. 1669-1676.
11. Yen R.F., Hong R.L., Tzen K.Y., Pan M.H., Chen T.H.: Whole-body 18-fluoro-2-deoxyglucose positron emission tomography in recurrent/metastatic nasopharyngeal carcinoma. J Nucl Med 2005; 46: pp. 770-774.
12. Tsai M.H., Shiau Y.C., Kao C.H., Shen Y.Y., Lin C.C., Lee C.C.: Detection of recurrent nasopharyngeal carcinomas with positron emission tomography using 18-fluoro-2-deoxyglucose in patients with indeterminate magnetic resonance imaging findings after radiotherapy. J Cancer Res Clin Oncol 2002; 128: pp. 279-282.
13. Goerres G.W., Mosna-Firlejczyk K., Steurer J., von Schulthess G.K., Bachmann L.M.: Assessment of clinical utility of 18F-FDG PET in patients with head and neck cancer: a probability analysis. Eur J Nucl Med Mol Imaging 2003; 30: pp. 562-571.
14. Gold M.R.Siegel J.E.Russell L.B.Weinstein M.C.Cost-effectiveness in health and medicine.1996.Oxford University PressNew York:
15. Elliot R., Payne K.: Essentials of economic evaluation in healthcare.2005.Pharmaceutical PressLondon
16. Cooper J.S., Scott C., Marcial V., et. al.: The relationship of nasopharyngeal carcinomas and second independent malignancies based on the Radiation Therapy. Cancer 1991; 67: pp. 1673-1677.
17. Sham J.S., Wei W.I., Tai P.T., Choy D.: Multiple malignant neoplasms in patients with nasopharyngeal carcinoma. Oncology 1990; 47: pp. 471-474.
18. Beck J.R., Kassirer J.P., Pauker S.G.: A convenient approximation of life expectancy (the “DEALE”): I. Am J Med 1982; 73: pp. 883-888.
19. Chua D.T., Wei W.I., Sham J.S., Chen A.C., Au G.: Treatment outcome for synchronous locoregional failures of nasopharyngeal carcinoma. Head Neck 2003; 25: pp. 585-594.
20. Poon D., Yap s.p., Wong Z.W., et. al.: Concurrent chemoradiotherapy in locoregionally recurrent nasopharyneal carcinoma. Int J Radiat Oncol Biol Phys 2004; 59: pp. 1312-1318.
21. Shin S.S., Ahn Y.C., Lim do H., Park W., Huh S.J.: High dose 3-dimensional re-irradiation for locally recurrent nasopharyngeal cancer. Yonsei Med J 2004; 45: pp. 100-106.