
Rationale and Objectives
Cardiac computed tomography is increasingly being used to assess the degree of stenosis in coronary arteries. It has been shown in multiple studies to have high negative predictive value for obstructive disease compared to invasive cardiac catheterization (ICA). However, calcified segments are interpreted differently in each study. The aim of this study was to examine the association of calcified plaques on multi–detector row cardiac computed tomography (MDCT) with the degree of stenosis on ICA.
Materials and Methods
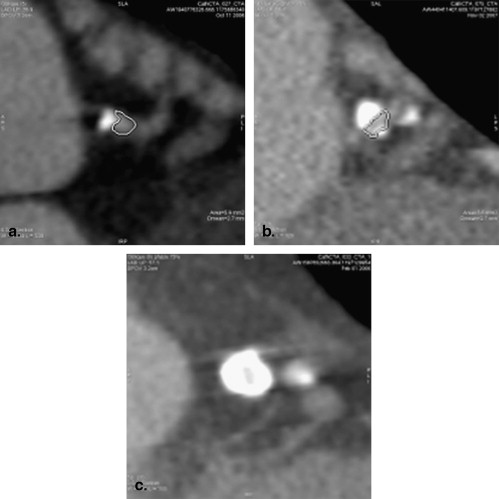
A total of 129 consecutive patients who underwent coronary evaluation on MDCT and also underwent ICA within 1 month of MDCT were included in the study. Each segment in the coronary artery was classified as mixed, calcified, or noncalcified. All segments with calcified plaque were evaluated, further classifying them as mild, moderate, or severe, and obstructive disease on ICA was used as the reference standard, in a blinded fashion.
Results
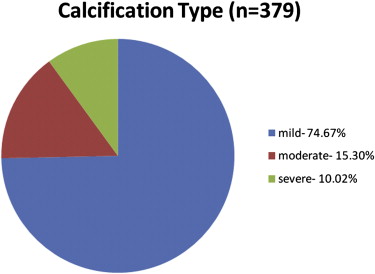
The average age of the patients was 60.8 ± 9.5 years. A total of 379 calcified segments were included in the study. Among these segments, 363 (95.8%) were found to be nonobstructive (<70% stenosis) on ICA. Calcifications were categorized as mild, moderate, and severe in 283 (74.7%), 58 (15.3%), and 38 (10.0%) segments, respectively. When calcium was incomplete in the cross-section of the lumen (mild or moderate calcification), 98.5% of these segments (336 of 341) were associated with nonobstructive disease, decreasing to 71% with severe calcification.
Conclusion
Calcified plaques seen on MDCT were commonly associated with nonobstructive disease on invasive angiography. Increasing focal calcification increased the likelihood of obstructive disease, but only 29% of severe segments were associated with significant obstructive disease.
Coronary artery disease (CAD) is the most common cause of morbidity and mortality around the world, often leading to myocardial infarction or death. Invasive cardiac catheterization (ICA) is currently the gold standard in diagnosing CAD but is insensitive in detecting calcified plaques . Cardiac computed tomography (CCT) is also used in assessing the degree of stenosis and is able to assess coronary plaque composition to a greater degree than ICA. In multiple studies, CCT has been shown to have high negative predictive value compared to ICA . Computed tomography (CT) is able to provide risk stratification more accurately than traditional risk factor assessment . It is used commonly to assess coronary artery calcium (CAC) as a predictor of coronary atherosclerosis burden and cardiovascular risk . In this study, we looked at the association of calcified plaques on multi–detector row CCT (MDCT) with the degree of stenosis on ICA. We sought to specifically evaluate the degree of stenosis associated with calcified segments and validate the fact that a calcified segment is not necessarily obstructive, as seen at times on ICA.
Materials and methods
Study Population
We initially included 145 patients from those who underwent catheterization and CCT within 1 month. Of this subset of 145 initially reviewed for our study, 129 were found to have calcifications in their coronary arteries on MDCT and were included for further analysis in the cohort.
Cardiac Computed Tomographic Image Acquisition and Postprocessing
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Catheterization Image Acquisition and Postprocessing
Get Radiology Tree app to read full this article<
Assessment of Coronary Calcium on CCT
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Demographics ( n = 129)
Variable Value Age (y) 60.8 ± 9.5 Dyslipidemia 73 (56.6%) Obesity 31 (24.0%) Hypertension 65 (50.4%) Diabetes 21 (16.3%) Family history of coronary artery disease 69 (53.5%) Lifestyle (sedentary) 24 (18.6%) Tobacco (primarily smoking) 51 (39.5%)
Data are expressed as mean ± standard deviation or as number (percentage).
Get Radiology Tree app to read full this article<
Calcification of Coronary Segments on CCT
Get Radiology Tree app to read full this article<
Table 2
Number of Segments for Each Type of Calcification on Cardiac Computed Tomography
Calcification Type Mild ( n = 283) Moderate ( n = 58) Severe ( n = 38) Total ( n = 379) Obstruction on catheterization (<70%) 280 (98.94%) 56 (96.55%) 27 (71.05%) 363 (95.78%) Obstruction on catheterization (>70%) 3 (1.06%) 2 (3.45%) 11(28.95%) 16 (4.22%)
Prob > | z | = .000 (ie, P value for trend mild to moderate to severe calcification for obstruction > 70%). Pearson’s χ 2 (1) = 63.8585 ( P = .000) (when combining mild and moderate calcification into one group).
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Limitations
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. Zhang S., Levin D.C., Halpern E.J., Fischman D., Savage M., Walinsky P.: Accuracy of MDCT in assessing the degree of stenosis caused by calcified artery plaques. AJR Am J Roentgenol 2008; 191: pp. 1676-1683.
2. Stolzmann P., Scheffel H., Leschka S., et. al.: Influence of calcifications on diagnostic accuracy using prospective ECG triggering. AJR Am J Roentgenol 2008; 191: pp. 1684-1689.
3. Eroglu E., Bayrak F., Gemici G., et. al.: Prevalence of coronary artery disease in low to moderate asymptomatic women: a multislice computed tomography study. Turk Kardiyol Dern Ars Arch Turk Soc Cardiol 2008; 36: pp. 439-445.
4. Raggi P., Cooil B., Ratti C., Callister T.Q., Budoff M.: Progression of coronary artery calcium and occurrence of myocardial infarction in patients with and without diabetes mellitus. Hypertension 2005; 46: pp. 238-243.
5. Raggi P., Callister T.Q., Shaw L.J.: Progression of coronary artery calcium and risk of first myocardial infarction in patients receiving cholesterol-lowering therapy. Arterioscler Thromb Vasc Biol 2004; 24: pp. 1272-1277.
6. Budoff M.J., Dowe D., Jollis J.G., et. al.: Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial. J Am Coll Cardiol 2008; 52: pp. 1724-1732.
7. Budoff M.J., Yang T.P., Shavelle R.M., Lamont D.H., Brundage B.H.: Ethnic differences in coronary atherosclerosis. J Am Coll Cardiol 2002; 39: pp. 408-412.
8. Budoff M.J., Achenbach S., Naurla J.: Atlas of cardiovascular computed tomography.2007.SpringerHong Kong, China 46
9. Nair D., Carrigan T.P., Curtin R.J., et. al.: Association of coronary atherosclerosis detected by multislice computed tomography and traditional risk-factor assessment. Am J Cardiol 2008; 102: pp. 316-320.
10. Liu X., Zhao X., Huang J., et. al.: Comparison of 3D free-breathing coronary MR angiography and 64-MDCT angiography for detection of coronary stenosis in patients with high calcium scores. AJR Am J Roentgenol 2007; 189: pp. 1326-1332.
11. Callister T.Q., Cooil B., Raya S.P., Lippolis N.J., Russo D.J., Raggi P.: Coronary artery disease: improved reproducibility of calcium scoring with an electron-beam CT volumetric method. Radiology 1998; 208: pp. 807-814.
12. Cho J.R., Kim Y.J., Ahn C.M., et. al.: Quantification of regional calcium burden in chronic total occlusion by 64-slice multi-detector computed tomography and procedural outcomes of percutaneous coronary intervention. Int J Cardiol 2009; 10: pp. 1-6.
13. Deetjen A.G., Conradi G., Mollmann S., et. al.: Diagnostic value of the 16-detector row multislice spiral computed tomography for the detection of coronary artery stenosis in comparison to invasive coronary angiography. Clin Cardiol 2007; 30: pp. 117-123.
14. Shaw L.J., Raggi P., Callister T.Q., Berman D.S.: Prognostic value of coronary artery calcium screening in asymptomatic smokers and non-smokers. Eur Heart J 2006; 27: pp. 968-975.
15. Budoff M.J., Shaw L.J., Liu S.T., et. al.: Long-term prognosis associated with coronary calcification. J Am Coll Aardiol 2007; 49: pp. 1860-1870.