
Rational and Objectives
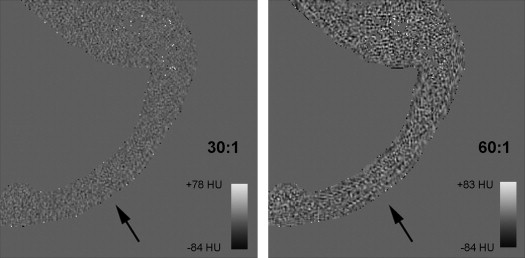
To investigate the effect of the Joint Photographic Experts Group (JPEG2000) 30:1 and 60:1 lossy compression on the detection of cranial vault fractures when compared to JPEG2000 lossless compression.
Materials and Methods
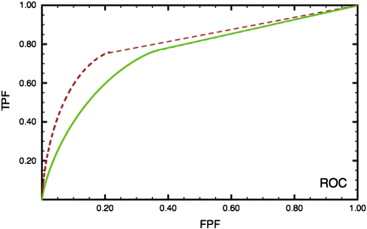
Fifty cranial computed tomography (CT) images were processed with three different level of JPEG2000 compression (lossless, 30:1 lossy, and 60:1 lossy) creating three sets of images. These were presented to five musculoskeletal specialists and five neuroradiologists. Each reader read at two of the three compression levels. Twenty-two cases contained a single fracture; the remaining 28 cases contained no fractures. Observers were asked to identify the presence or absence of a fracture, to locate its site, and rate their degree of confidence. Receiver operating characteristic (ROC), jackknife free-response receiver operating characteristic (JAFROC) and the Dorfman-Berbaum-Metz multiple reader multiple case (DBM-MRMC) analyses were used to explore differences between the lossless and lossy compressed images.
Results
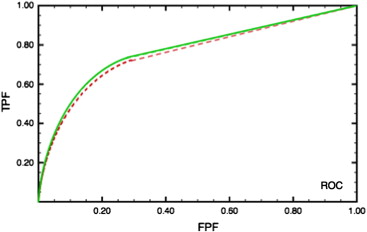
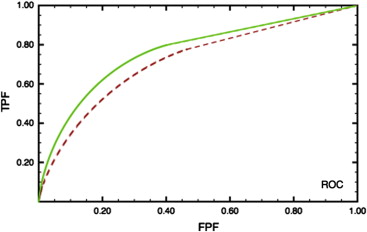
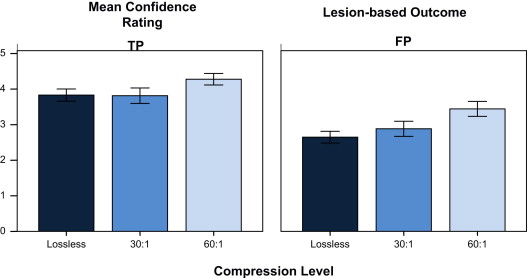
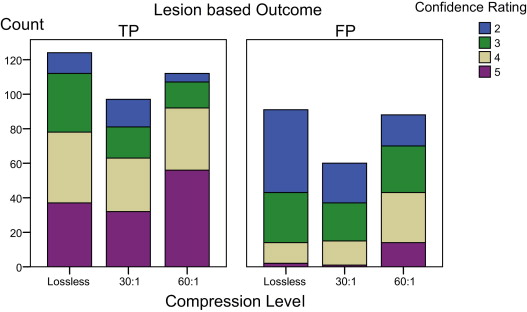
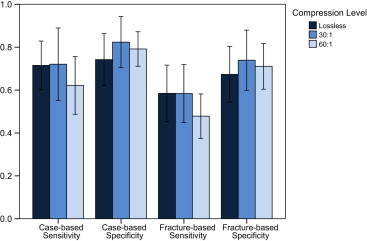
JPEG2000 lossless and 30:1 lossy compression demonstrated no significant difference in their performance with JAFROC and DBM-MRMC analysis ( P < .416); however, JPEG2000 30:1 lossy compression demonstrated significantly better performance than 60:1 lossy compression ( P < .016). A significant increase in misplaced confidence ratings was also seen with 60:1 ( P < .037) over 30:1 lossy and lossless compression.
Conclusion
JPEG2000 60:1 compression degrades the detection of skull fractures significantly while increasing the confidence with which readers rate fractures compared with 30:1 lossy and lossless compression. JPEG2000 30:1 lossy compression does not significantly change performance when compared to JPEG2000 lossless for the detection of skull fractures on CT.
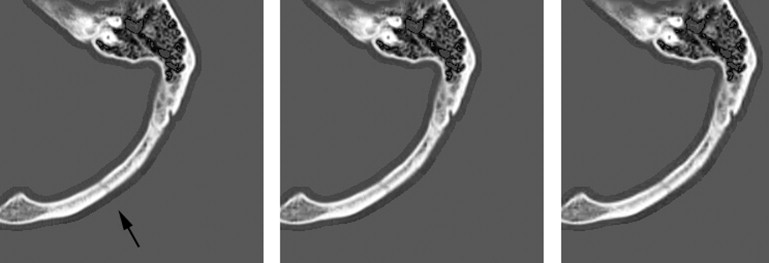
Increasing volumes of data generated by medical imaging is a problem for image storage, management, transmission, and display . Data compression is a possible solution to this problem but it has limitations. Compression can be performed in a lossless, reversible manner, where no information is lost. However, this only allows a 2:1 to 3:1 reduction in data size for medical images . On the other hand, compressing in a lossy, irreversible manner allows much higher levels of compression, but some information has to be discarded. At lower levels of compression, much of the discarded information is high-frequency uncorrelated noise, and image degradation is imperceptible to the human eye . At higher levels of compression, perceptible changes occur, though the image may still be acceptable for diagnostic use. The current study investigates how much compression can be tolerated in skull computed tomography (CT) before the diagnostic quality for detection of fractures is affected.
Previous studies have examined the effect of image compression on various imaging applications, for example, chest radiographs , musculoskeletal radiographs , mammograms , chest CT , abdominal CT , cerebral CT , nuclear medicine studies , and coronary angiograms . The tolerance of images to compression varies by modality and region and hence the acceptable compression threshold identified by these studies is varied. There are also several ways to define this threshold, such as quantitative metrics based on numerical assessment of pixel values before and after compression , the visually lossless threshold (the maximum compression at which the compressed image cannot be distinguished from the noncompressed image by a human observer) that is felt to be a relatively conservative threshold , and diagnostic accuracy.
Get Radiology Tree app to read full this article<
Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Image compression Expressed as Effective Bits Per Pixel
Nominal Compression Level 512 × 512 Image Data Size Bits Stored Bits Used ∗ Bits/Pixel Effective Compression Bits/Pixel Effective Compression 0 (lossless) 524,288 16 None 14 None 30:1 (lossy) 16,951 0.52 30.9:1 0.52 27.1:1 60:1 (lossy) 8416 0.26 62.3: 0.26 54.7:1
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 2
The JAFROC FOM and ROC AUC Results for the Four Readers That Read Both Lossless and 60:1 Compressed Images
ID Specialty JAFROC FOM ROC AUC Lossless 60:1 Lossless 60:1 1 MSK (ABR)0.734 0.6740.776 0.715 2 MSK 0.6630.703 0.7130.703 3 NR 0.7040.740 0.7260.760 4 NR (ABR) 0.7270.777 0.7780.820 Reader averaged FOMs/AUCs and 95% CI 0.715 (0.627, .8023) 0.723 (0.6226, 0.8240) 0.748 (0.666, 0.829) 0.749 (0.64, 0.85) Mean difference (SD) and P value 0.047 (0.011) P ≤ .197 0.037 (0.021) P ≤ .946
ABR, examining radiologist of the American Board of Radiology; AUC, area under the curve; FOM, figure of merit; JAFROC, jackknife free-response ROC; NR, neuroradiologist; ROC, receiver operating characteristic; TMSK, musculoskeletal radiologist.
The highest scoring reading is in bold. P values given are for readers and cases considered random.
Table 3
The JAFROC FOM and ROC AUC Results for the Four Readers That Read Both Lossless and 30:1 Compressed Images
ID Speciality JAFROC FOM ROC AUC Lossless 30:1 Lossless 30:1 5 MSK (ABR)0.810 0.7600.852 0.782 6 NR (ABR)0.804 0.7770.824 0.817 7 NR (ABR)0.784 0.776 0.8080.835 Reader averaged FOMs/AUCs and 95% CI 0.799 (0.7165, 0.8818) 0.711 (0.675, 0.867) 0.827 (0.753, 0.90) 0.811 (0.72, 0.898) Mean difference (SD) and P value 0.028 (0.021) P ≤ .416 0.035 (0.032) P ≤ .681
ABR, examining radiologist of the American Board of Radiology; AUC, area under the curve; FOM, figure of merit; JAFROC, jackknife free-response ROC; NR, neuroradiologist; ROC, receiver operating characteristic; TMSK, musculoskeletal radiologist.
The highest scoring reading is in bold. The P values given are for readers and cases considered random.
Table 4
The JAFROC FOM and ROC AUC Results for the Four Readers That Read Both 30:1 and 60:1 Compressed Images
ID Speciality JAFROC FOM ROC AUC 30:1 60:1 30:1 60:1 8 NR (ABR)0.669 0.5670.712 0.607 9 MSK (ABR)0.815 0.7690.815 0.811 10 MSK (ABR)0.666 0.5850.773 0.718 Reader averaged FOMs/AUCs and 95% CI 0.723 (0.5710, 0.874) 0.640 (0.416, 0.864) 0.766 (0.664,0.869) 0.711 (0.5, 0.92) Mean difference (SD) and P value 0.076 (0.028) P ≤ .016 ∗ 0.055 (0.051) P ≤ .194
ABR, examining radiologist of the American Board of Radiology; AUC, area under the curve; FOM, figure of merit; JAFROC, jackknife free-response ROC; NR, neuroradiologist; ROC, receiver operating characteristic; TMSK, musculoskeletal radiologist.
The highest scoring reading is in bold. The P values given are for readers and cases considered random.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. Rubin G.D.: Data explosion: the challenge of multidetector-row CT. Eur J Radiol 2000; 36: pp. 74-80.
2. Tamm E.P., Thompson S., Venable S.L., et. al.: Impact of multislice CT on PACS resources. J Digit Imaging 2002; 15: pp. 96-101.
3. Karson T.H., Chandra S., Morehead A.J., et. al.: JPEG compression of digital echocardiographic images: impact on image quality. J Am Soc Echocardiogr 1995; 8: pp. 306-318.
4. Wong S., Zaremba L., Gooden D., et. al.: Radiological image compression: a review. Proc IEEE 1995; 83: pp. 194-218.
5. Sung M.M., Kim H.J., Yoo S.K., et. al.: Clinical evaluation of compression ratios using JPEG2000 on computed radiography chest images. J Digital Imaging 2002; 15: pp. 78-83.
6. Bramble J.M., Cook L.T., Murphy M.D., et. al.: Image data compression in magnification hand radiographs. Radiology 1989; 170: pp. 133-136.
7. Penedo M., Souto M., Tahoces P.G., et. al.: Free-response receiver operating characteristic evaluation of Lossy JPEG2000 and object-based set partitioning in hierarchical stress compression of digital mammograms. Radiology 2005; 237: pp. 450-457.
8. Kim B., Lee K.H., Kim K.J., et. al.: Prediction of perceptible artifacts in JPEG2000-compressed chest CT images using mathematical and perceptual quality metrics. AJR Am J Roentgenol 2008; 190: pp. 328-334.
9. Woo H.S., Kim K.J., Kim T.J.: JPEG2000 compression of abdominal CT: difference in tolerance between thin- and thick- section CT. AJR Am J Roentgenol 2007; 189: pp. 535-541.
10. Ringl H., Schernthaner R., Sala E., et. al.: Lossy 3D JPEG2000 compression of abdominal CT images in patients with acute abdominal complaints: effect of compression ratio on diagnostic confidence and accuracy. Radiology 2008; 248: pp. 476-484.
11. Ohgiya Y., Gokan T., Nobusawa H., et. al.: Acute cerebral infarction: effect of JPEG compression on detection at CT. Radiology 2003; 227: pp. 124-127.
12. Chameroy V., Di Paolo R.: High compression of nuclear medicine dynamic studies. Int J Cardiol Imaging 1990; 5: pp. 261-269.
13. Silber S., Doee R., Zindler G., et. al.: Impact of various compression rates on interpretation of digital coronary angiogram. Int J Cardiol 1997; 60: pp. 195-200.
14. Erickson B.J., Manduca A., Palisson P., et. al.: Wavelet compression of medical images. Radiology 1998; 206: pp. 599-607.
15. Slone R.M., Foos D.H., Whiting B.R., et. al.: Assessment of visually lossless irreversible image compression: comparison of three methods by using an image-comparison workstation. Radiology 2000; 215: pp. 543-553.
16. DICOM Standards Committee Working Group 4: Compression: Supplement 61: JPEG2000 Transfer Syntaxes.2000.NEMAVirginia
17. Manduca A.: Interactive wavelet-based 2-D and 3-D image compression. Proc SPIE 1897; 1993: pp. 307-318.
18. Christopoulos C., Ebrahimi T.: The JPEG2000 still image coding system: an overview. IEEE Trans Cons Electronics 2000; 46: pp. 1103-1127.
19. Persons K.R., Palisson P., Manduca A., et. al.: An analytical look at the effects of image compression on medical images. J Digit Imaging 1997; 10: pp. 60-66.
20. Erickson B.J., Manduca A., Persons K.R., et. al.: Evaluation of irreversible compression of digitized PA chest radiographs. J Digit. Imaging 1997; 10: pp. 97-102.
21. Brennan P.C., Mc Entee M.F., Evanoff M.G., et. al.: Ambient lighting: effect of illumination on softcopy viewing of radiographs of the wrist. AJR Am J Roentgenol 2007; 188: pp. W177-W180.
22. Kotter E., Roesner A., Torsten Winterer J., et. al.: Evaluation of Lossy data compression of chest X-rays: a receiver operating characteristic study. Invest Radiol 2003; 38: pp. 243-249.
23. Dorfman D., Berbaum K., Metz C.E.: Receiver operating characteristic rating analysis. Generalization to the population of readers and patients with the jackknife method. Invest Radiol 1992; 27: pp. 723-731.
24. Hillis S., Obuchowski N., Schartz K.M., et. al.: A comparison of the Dorfman-Berbaum-Metz and Obuchowski-Rockette methods for receiver operating characteristic (ROC) data. Stat Med 2005; 24: pp. 1579-1607.
25. Krupinski E.: Technology and perception in the 21st-century reading room. J Am Coll Radiol 2006; 3: pp. 433-440.
26. Kundel H.L.: History of research in medical image perception. J Am Coll Radiol 2006; 3: pp. 402-408.
27. Chakraborty D.: Validation and statistical power comparison of methods for analyzing free-response observer performance studies. Acad Radiol 2008; 15: pp. 1554-1566.
28. Kundel H.L., Berbaum K., Dorfman D., et. al.: Receiver operating characteristic analysis in medical imaging. J Intl Commission Radiation Units Measurements 2006; 8: pp. 1-62.
29. Metz C.E.: ROC methodology in radiologic imaging. Invest Radiol 1996; 21: pp. 720-733.
30. Savcenko V., Erickson B.J., Palisson P.M., et. al.: Detection of subtle abnormalities on chest radiographs after irreversible compression. Radiology 1998; 206: pp. 609-616.
31. Baudin O., Baskurt A., Moll T., et. al.: ROC assessment of compressed wrist radiographs. Eur J Radiol 1996; 22: pp. 228-231.
32. Li F., Sone S., Takashima S., et. al.: Effects of JPEG and wavelet compression of spiral low-dose CT images on detection of small lung cancers. Acta Radiol 2001; 42: pp. 156-160.
33. Ko J.P., Rusinek H., Naidich D.P., et. al.: Wavelet compression of low-dose chest CT data: effect on lung nodule detection. Radiology 2003; 228: pp. 70-75.
34. Bajpai V., Lee K.H., Kim B., et. al.: Differences in compression artifacts on thin- and thick-section lung CT images. AJR Am J Roentgenol 2008; 191: pp. W38-W43.
35. Kim T.J., Lee K.H., Kim B., et. al.: Regional variance of visually lossless threshold in compressed chest CT images: lung versus mediastinum and chest wall. Eur J Radiol 2009; 69: pp. 483-488.
36. Lee K.H., Kim Y.H., Kim B.H., et. al.: Irreversible JPEG 2000 compression of abdominal CT for primary interpretation: assessment of visually lossless threshold. Eur Radiol 2007; 17: pp. 1529-1534.
37. Erickson B.J., Krupinski E., Andriole K.P.: A multicenter observer performance study of 3D JPEG2000 compression of thin-slice CT. J Digit Imaging 2010; 23: pp. 639-643.
38. Nikolovski I., McEntee M.F., Bourne R., et. al.: The effect of compression on confidence during the detection of skull fractures in CT. Proc SPIE 2012; 8318: pp. 83181O.