
Rationale and Objectives
A lack of pancreatic duct compliance and decreased duodenal filling on secretin-stimulated magnetic resonance cholangiopancreatography (s-MRCP) has been noted in patients with chronic pancreatitis. Whether endoscopic sphincterotomy can affect pancreatic duct compliance and duodenal filling on diagnostic s-MRCP is unknown.
Materials and Methods
A retrospective review of patients referred to the authors’ clinic from December 2006 to December 2007 was performed. Those patients with no evidence of chronic pancreatitis who underwent s-MRCP were studied. Findings on s-MRCP were analyzed, specifically noting change in pancreatic duct diameter size from baseline to maximum dilation and duodenal filling after secretin administration (0.2 μg/kg intravenous dose of human secretin).
Results
Of the 34 patients studied, 12 underwent endoscopic sphincterotomy, and 22 had intact sphincters of Oddi. In the sphincterotomy group, there was a mean change of 0.2 cm (range, 0.0–0.4 cm), while in the nonsphincterotomy group, the mean change was 0.9 cm (range, 0.3–2.0 cm) after secretin administration. The difference was significant ( P < .005).
Conclusion
Endoscopic sphincterotomy significantly decreases pancreatic duct dilation in response to secretin on s-MRCP. However, further studies are required to determine the effect sphincterotomy has on the amount of duodenal filling and the rate at which duodenal filling occurs.
The diagnosis of chronic pancreatitis is based on the evaluation of both functional and structural characteristics of the pancreas. On secretin-stimulated magnetic resonance cholangiopancreatography (s-MRCP), both pancreatic exocrine function and pancreatic ductal morphology can be evaluated ( ), the former of which is indirectly determined on s-MRCP by the degree of duodenal filling immediately after secretin stimulation. Although standard MRCP without secretin stimulation can assess pancreatic ductal morphology according to the Cambridge classification, small side-branch ectasia may not be seen without exocrine stimulation of the gland . Thus, better visualization of ectatic side branches after secretin stimulation may increase confidence in the diagnosis of chronic pancreatitis.
In recent years, investigators have noted that changes in the main pancreatic duct in response to secretin can also suggest the presence or absence of chronic pancreatitis . Most notably, these same investigators reported that in patients with chronic pancreatitis, there is limited secretin-stimulated dilatation of the pancreatic duct (compliance), compared to normal controls, and that the time to reach maximal pancreatic duct diameter is prolonged, suggesting that fibrosis in the gland may prohibit the pancreatic duct from having normal compliance.
Get Radiology Tree app to read full this article<
Materials and methods
Patient Population
Get Radiology Tree app to read full this article<
Magnetic Resonance Imaging Technique
Get Radiology Tree app to read full this article<
Image Analysis
Get Radiology Tree app to read full this article<
Parameters Analyzed
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Patient Demographics
Variable Group 1 Group 2 Number of patients 22 12 Mean age (y) 44 48.5 Men/women 9/13 3/9 Sphincterotomy 0 12 (8 D, 4 B)
B, biliary sphincterotomy only; D, dual sphincterotomy.
Get Radiology Tree app to read full this article<
Pancreatic Duct
Get Radiology Tree app to read full this article<
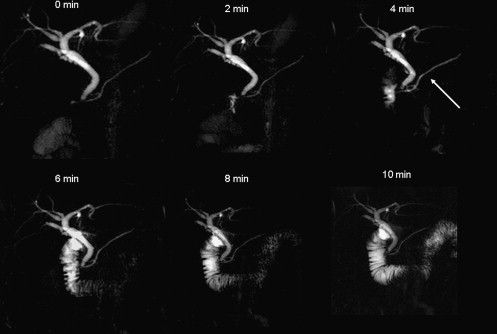
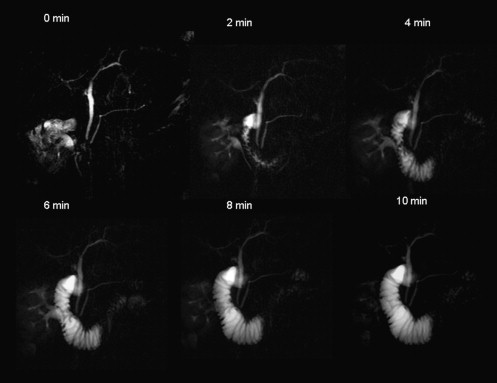
Table 2
Pancreatic Duct Compliance After Secretin
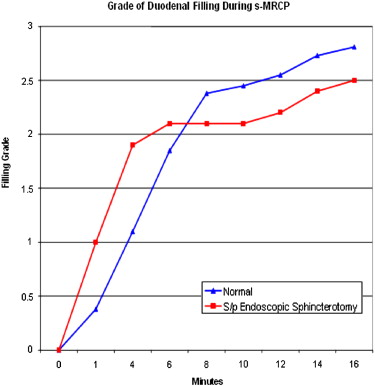
Variable Group 1 Group 2 Absolute change in pancreatic duct diameter (cm) ∗ 0.9 (0.3–2.0) 0.2 (0.0–0.4) Percentage change in pancreatic duct diameter ∗ 60% (13%–123%) 10% (1%–38%) Time to reach maximal pancreatic duct diameter (min) 5.6 (3–17) 5.3 (1–10) Mean pancreatic duct diameter at peak (cm) 2.45 2.04 Duodenal filling at peak pancreatic duct diameter 1.5 (0–3) 1.8 (0–3) Time to maximal duodenal filling (min) 8.0 6.4
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Duodenal Filling
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Manfredi R., Costamagna G., Brizi M., et. al.: Severe chronic pancreatitis versus suspected pancreatic disease: dynamic MR cholangiopancreatography after secretin stimulation. Radiology 2000; 214: pp. 849-855.
2. Matos C., Metens T., Deviere J., et. al.: Pancreatic duct: morphologic and functional evaluation with dynamic MR pancreatography after secretin stimulation. Radiology 1997; 203: pp. 435-441.
3. Czako L.: Diagnosis of early-stage chronic pancreatitis by secretin-enhanced magnetic resonance cholangiopancreatography. J Gastroenterol 2007; 42: pp. 113-117.
4. Czako L., Endes J., Takacs T., et. al.: Evaluation of pancreatic exocrine function by secretin-enhanced magnetic resonance cholangiopancreatography. Pancreas 2000; 23: pp. 323-328.
5. Sica G., Braver J., Cooney M., et. al.: Comparison of endoscopic retrograde cholangiopancreatography with MR cholangiopancreatography in patients with pancreatitis. Radiology 1999; 210: pp. 605-610.
6. Cappeliez O., Delhaye M., Deviere J., et. al.: Chronic pancreatitis: evaluation of pancreatic exocrine function with MR pancreatography after secretin stimulation. Radiology 2000; 215: pp. 358-364.
7. Chan J.H., Tsui E.Y., Yuen M.K., et. al.: Gadopentetate dimeglumine as an oral negative gastrointestinal contrast agent for MRCP. Abdom Imaging 2000; 25: pp. 405-408.
8. Balci N.C., Alkaade S., Magas L., et. al.: Suspected chronic pancreatitis with normal MRCP: findings on MRI in correlation secretin MRCP. J Magn Reson Imaging 2008; 27: pp. 125-131.
9. Fukukura Y., Fujiyoshi F., Sasaki M., et. al.: Pancreatic duct: morphologic evaluation with MR cholangiopancreatography after secretin stimulation. Radiology 2002; 222: pp. 674-680.
10. Ladas S.D., Tassios P.S., Giorgiotis K., et. al.: Pancreatic duct width: its significance as a diagnostic criterion for pancreatic disease. Hepatogastroenterology 1993; 40: pp. 52-55.
11. Geenen J., Hogan W., Dodds W., et. al.: Intraluminal pressure recording from the human sphincter of Oddi. Gastroenterology 1980; 78: pp. 317-324.
12. Pereira S.P., Gillams A., Sgouros S.N., et. al.: Prospective comparison of secretin-stimulated magnetic resonance cholangiopancreatography with manometry in the diagnosis of sphincter of Oddi dysfunction types II and III. Gut 2007; 56: pp. 809-813.