
Rationale and Objectives
The objective of this study was to experimentally test the effect of interruptions on image interpretation by comparing reading time and response accuracy of interrupted case reads to uninterrupted case reads in resident and attending radiologists.
Materials and Methods
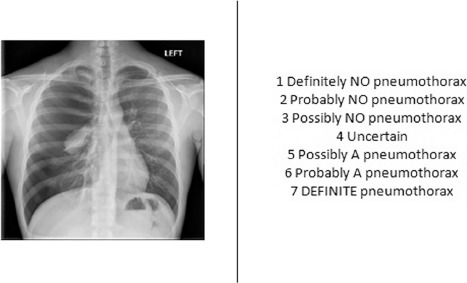
Institutional review board approval was obtained before participant recruitment from an urban academic health-care system during January 2016–March 2016. Eleven resident and 12 attending radiologists examined 30 chest radiographs, rating their confidence regarding the presence or the absence of a pneumothorax. Ten cases were normal (ie, no pneumothorax present), 10 cases had an unsubtle pneumothorax (ie, readily perceivable by a nonexpert), and 10 cases had a subtle pneumothorax. During three reads of each case type, the participants were interrupted with 30 seconds of a secondary task. The total reading time and the accuracy of interrupted and uninterrupted cases were compared. A mixed-factors analysis of variance was run on reading time and accuracy with experience (resident vs attending) as a between-subjects factor and case type (normal, unsubtle, or subtle) and interruption (interruption vs no interruption) as within-subjects factors.
Results
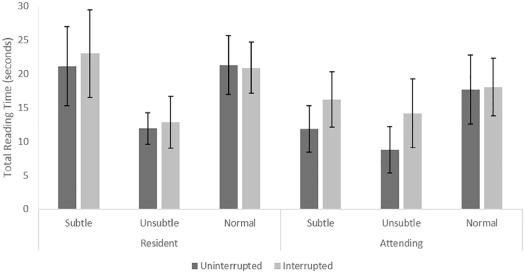
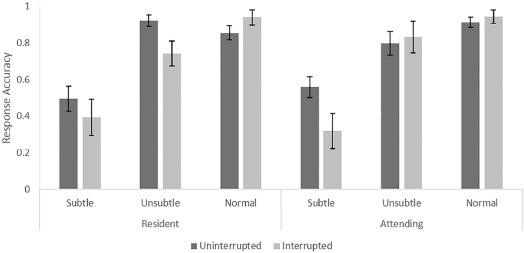
Interrupted tasks had significantly longer reading times than uninterrupted cases ( P = .032). During subtle cases, interruptions reduced accuracy ( P = .034), but during normal cases, interruptions increased accuracy ( P = .038).
Conclusions
Interruptions increased reading times and increased the tendency for a radiologist to conclude that a case is normal for both resident and attending radiologists, demonstrating that interruptions reduce efficiency and introduce patient safety concerns during reads of abnormal cases.
Introduction
The primary responsibility of a radiologist is accurate and efficient image interpretation. The radiologist’s role as a consultant, however, lends itself to frequent interruptions. These interrupting tasks include answering telephone calls, responding to pages, and answering questions in person . During peak call hours, an on-call radiologist could be interrupted two to three times while trying to do the initial interpretation of a case . It has also been found that attending radiologists are interrupted an average of 4.8 times per hour with an average of 2.5 minutes per interruption, which likely results in memory decay of the case read. Most of the interruptions observed by Ratwani and colleagues in this study required complete disengagement from the case read, making it more difficult to resume reading the case after the interruption than if the interruption had only required partial disengagement . Despite the prevalence of interruptions in the radiologist’s workflow, little work has examined the influence of interruptions on radiologists’ ability to perform their primary task of reading cases and providing interpretations.
Some interruptions in a radiologist’s workflow are unavoidable, but previous work has suggested that interruptions cause frustration and introduce patient safety concerns in the health-care environment . Detrimental effects of interruptions have been observed in many areas of health care, including, but not limited to, the following: the emergency department, in which clinicians fail to return to 18.5% of interrupted tasks ; the intensive care unit, in which five of six cases in which patient safety hazards were observed were preceded by an interruption ; and medication administration, in which it has been demonstrated that the occurrence and frequency of interruptions are related to errors in administration . Although these findings provide evidence that interruptions negatively influence patient safety in those environments, the workflow of a radiologist is unique and merits investigation that is designed to address it specifically, particularly given the amount of visual processing most radiologists perform.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Participants
Get Radiology Tree app to read full this article<
TABLE 1
Distribution of Resident Experience and Attending Specialty
Resident Year Count Attending Specialty Count First year 2 Body 4 Second year 3 Breast 2 Third year 4 Chest 1 Fourth year 2 Interventional 3 Musculoskeletal 1 Neuroradiology 1
Get Radiology Tree app to read full this article<
Procedure
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Analysis
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Reading Time
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Response Accuracy
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Ratwani R.M., Wang E., Fong A., et. al.: A human factors approach to understanding the types and sources of interruptions in radiology reading rooms. J Am Coll Radiol 2016; 13: pp. 1102-1105.
2. Yu J.-P.J., Kansagra A.P., Mongan J.: The radiologist’s workflow environment: evaluation of disruptors and potential implications. J Am Coll Radiol 2014; 11: pp. 589-593.
3. Kansagra A.P., Liu K., Yu J.P.J.: Disruption of radiologist workflow. Curr Probl Diagn Radiol 2016; 45: pp. 101-106.
4. Grundgeiger T., Sanderson P.: Interruptions in healthcare: theoretical views. Int J Med Inform 2009; 78: pp. 293-307.
5. Li S.Y.W., Magrabi F., Coiera E.: A systematic review of the psychological literature on interruption and its patient safety implications. J Am Med Inform Assoc 2012; 19: pp. 6-12.
6. Westbrook J.I., Coiera E., Dunsmuir W.T.M., et. al.: The impact of interruptions on clinical task completion. Qual Saf Health Care 2010; 19: pp. 284-289.
7. Drews F.A.: The frequency and impact of task interruptions in the ICU. Proc Hum Factors Ergon Soc 51st Annu Meet 2007; pp. 683-686.
8. Westbrook J.I.: Association of interruptions with an increased risk and severity of medication administration errors. Arch Intern Med 2010; 170: pp. 683.
9. Ratwani R., Trafton J.G.: An eye movement analysis of the effect of interruption modality on primary task resumption. Hum Factors 2010; 52: pp. 370-380.
10. Trafton J.G., Altmann E.M., Ratwani R.M.: A memory for goals model of sequence errors. Cogn Syst Res 2011; 12: pp. 134-143.
11. Altmann E.: Memory for goals: an activation-based model. Cogn Sci 2002; 26: pp. 39-83.
12. Shen Y.J., Jiang Y.V.: Interrupted visual searches reveal volatile search memory. J Exp Psychol Hum Percept Perform 2006; 32: pp. 1208-1220.
13. Kelly B.S., Rainford L.A., Darcy S.P., et. al.: The development of expertise in radiology: In chest radiograph interpretation, “expert” search pattern may predate “expert” levels of diagnostic accuracy for pneumothorax identification. Radiology 2016; 280: pp. 252-260.
14. Balint B.J., Steenburg S.D., Lin H., et. al.: Do telephone call interruptions have an impact on radiology resident diagnostic accuracy?. Acad Radiol 2014; 21: pp. 1623-1628.
15. Altmann E.M., Trafton J.G.: Task interruption: resumption lag and the role of cues. Proc 26th Annu Conf Cogn Sci Soc 2004; pp. 43-48.
16. Ratwani R.M., Trafton J.G.: Spatial memory guides task resumption. Vis Cogn 2008; 16: pp. 1001-1010.
17. Mello-Thoms C., Dunn S.M., Nodine C.F., et. al.: An analysis of perceptual errors in reading mammograms using quasi-local spatial frequency spectra. J Digit Imaging 2001; 14: pp. 117-123.